




Información del artículo
Texto completo
Bibliografía
Descargar PDF
Estadísticas
Figuras (2)
Tablas (2)
Table 1. Assessment of the severity of aortic stenosis based on the main echocardiographic parameters.

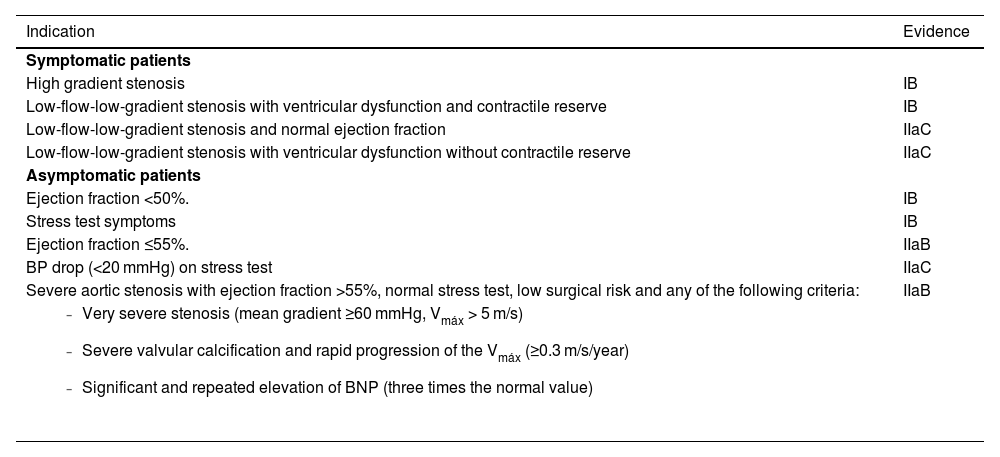
Table 2. Indications for valve replacement in severe aortic stenosis according to the European Society of Cardiology.12
Mostrar másMostrar menos
Artículo
Opciones para acceder a los textos completos de la publicación Medicina Clínica (English Edition)
Suscriptor
Suscribirse

Comprar
Comprar acceso al artículo
Comprando el artículo el PDF del mismo podrá ser descargado
Precio 19,34 €
Comprar ahora
Comprando el artículo el PDF del mismo podrá ser descargado
Precio 19,34 €
Comprar ahora
Contactar
Teléfono para suscripciones e incidencias
De lunes a viernes de 9h a 18h (GMT+1) excepto los meses de julio y agosto que será de 9 a 15h
Llamadas desde España
932 415 960
Llamadas desde fuera de España
+34 932 415 960
E-mail
