




Cardiac involvement in systemic sclerosis (SS) is frequently silent and a major cause of mortality in these patients. This work aims to study the prevalence and associations of left ventricular dysfunction (LVD) and arrhythmias in SS.
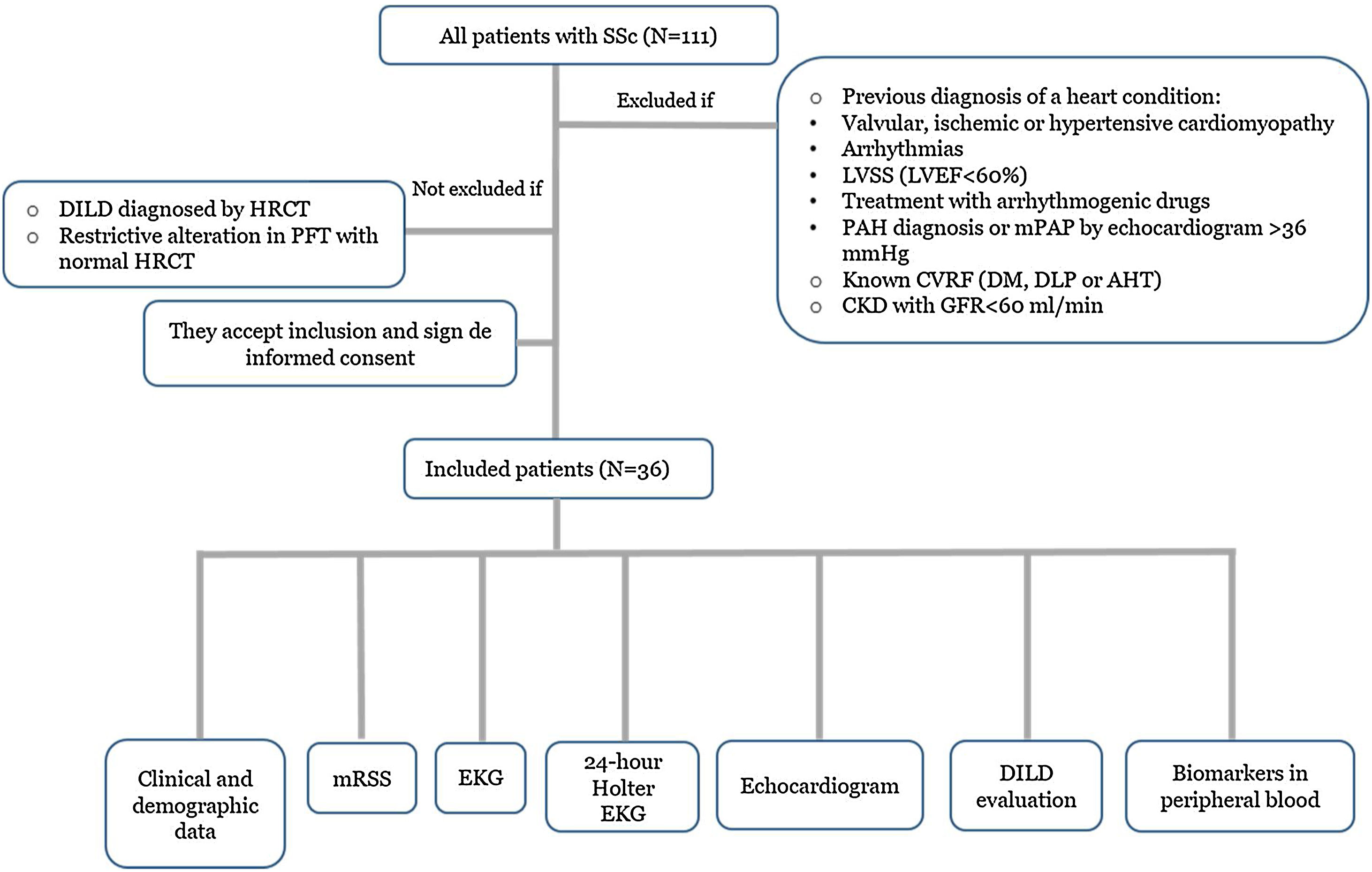
Methods and resultsProspective study of SS patients (n=36), excluding those with symptoms of (or) cardiac disease, pulmonary arterial hypertension or cardiovascular risk factors (CVRF). A clinical, analytical, electrocardiogram (EKG), Holter, and echocardiogram with global longitudinal strain (GLS) assessment were performed. Arrhythmias were classified into clinically significant arrhythmias (CSA) and non-significant.
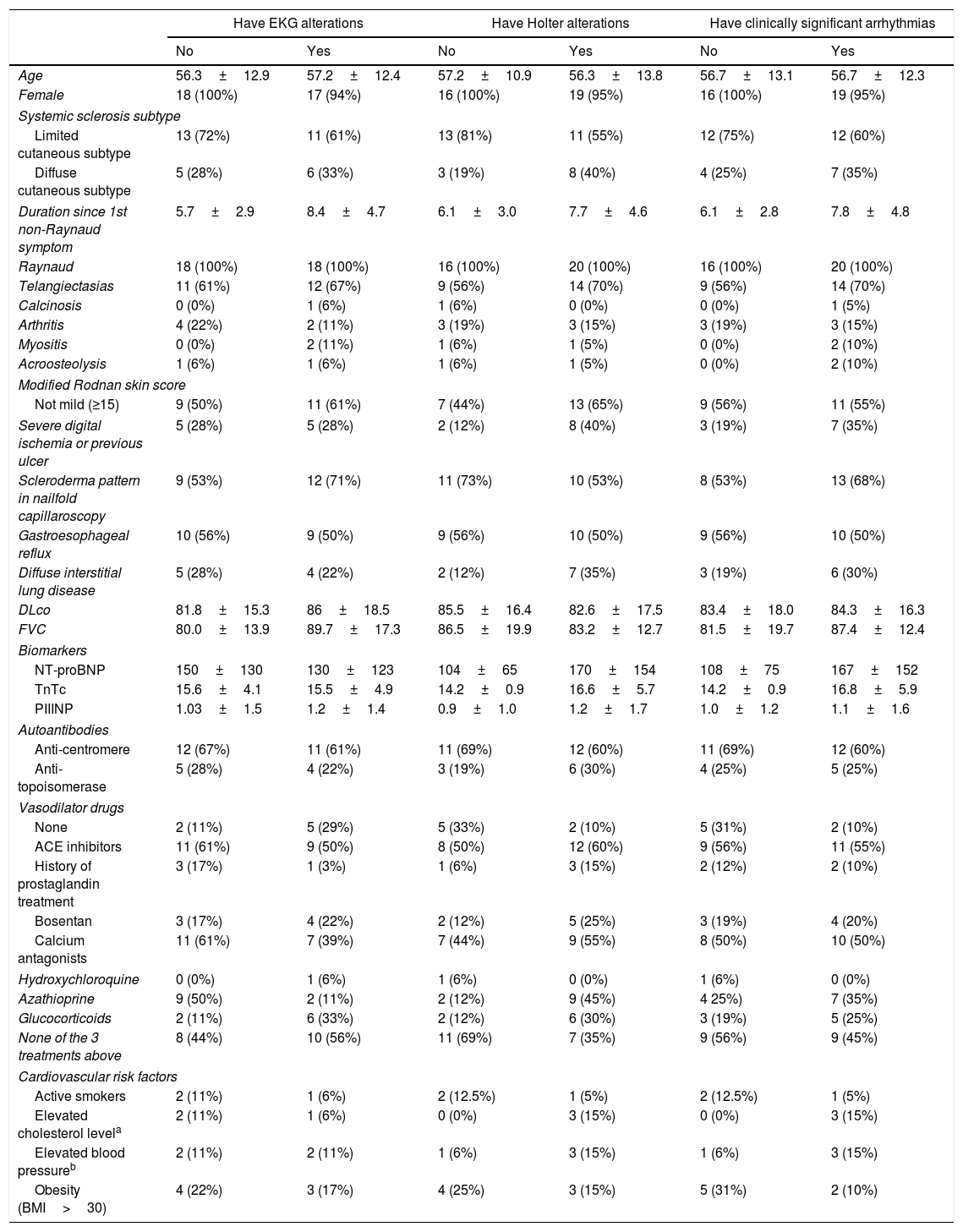
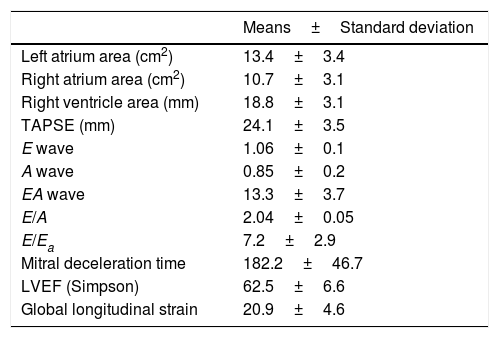
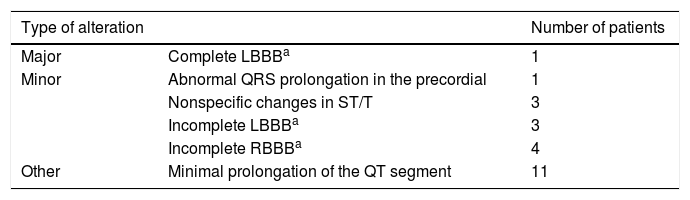
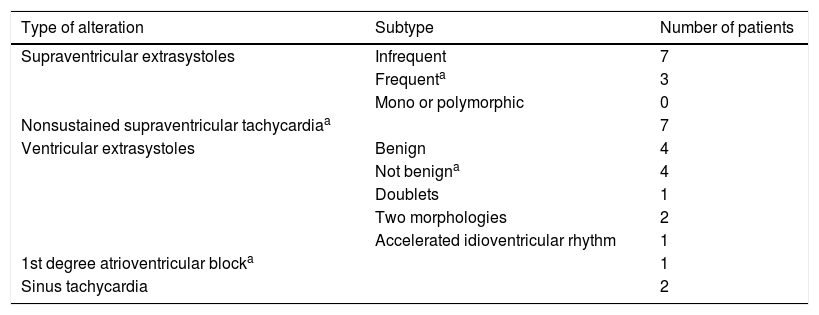
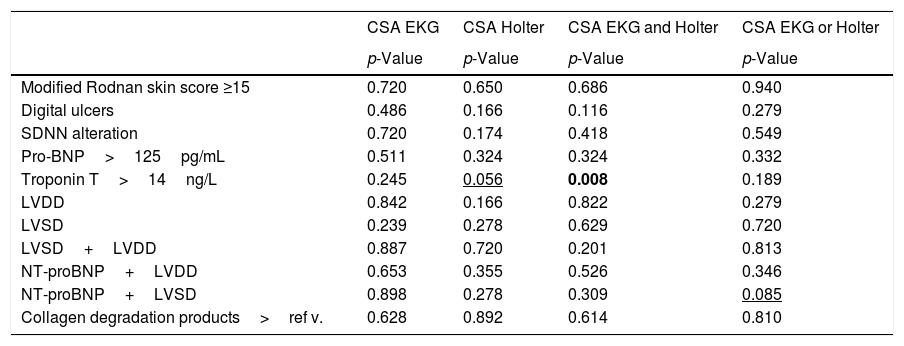
Twenty-eight percent had left ventricular diastolic dysfunction (LVDD), 22% LV systolic dysfunction (LVSD) according to the GLS, 11.1% both, and 16.7% cardiac dysautonomia. Fifty percent presented alterations by EKG (44% CSA), 55.6% by Holter (75% CSA) and 8.3% CSA by both. An association was found between the elevation of troponin T (TnTc) and CSA and between the elevation of both NT-proBNP and TnTc with LVDD.
ConclusionsWe found a higher prevalence of LVSD than in the literature, detected by GLS and being 10 times higher than that detected by LVEF, which justifies the need to incorporate this technique in the routine evaluation of these patients. The association of TnTc and NT-proBNP with LVDD suggests that they can be used as minimally invasive biomarkers of this affectation. The absence of correlation between LVD and CSA indicates that the arrhythmias could be due, not only to a supposed structural alteration of the myocardium, but to an independent and early cardiac involvement, which should be actively investigated even in asymptomatic patients without CVRF.
La afectación cardiaca en la esclerosis sistémica (ES) es frecuentemente asintomática y se asocia con una mortalidad importante. Este trabajo tiene como objetivo estudiar la prevalencia y las asociaciones de la disfunción ventricular izquierda (DVI) y las arritmias en la ES.
Métodos y resultadosEstudio prospectivo de pacientes con ES (n = 36), excluyendo aquellos con síntomas o enfermedad cardiaca, hipertensión arterial pulmonar o factores de riesgo cardiovascular (FRCV). Se les realizó una evaluación clínica, analítica, con electrocardiograma (ECG), Holter y ecocardiograma con strain longitudinal global (SLG). Las arritmias se clasificaron en arritmias clínicamente significativas (ACS) y no significativas.
De los pacientes estudiados, 27,8% presentaba disfunción diastólica del ventrículo izquierdo (DDVI), 22% disfunción sistólica del VI (DSVI) según el SLG, 11,1% ambas y 16,7% disautonomía cardiaca; 50% presentó alteraciones por ECG (44% ACS), 55,6% por Holter (75% ACS) y 8,3% ACS por ambos. Se encontró una asociación entre la elevación de troponina T (TnTc) y ACS y entre la elevación NT-proBNP y TnTc con la DDVI.
ConclusionesEncontramos una prevalencia de DSVI mayor que en la literatura, detectada por SLG y siendo 10 veces superior a la detectada por FEVI, lo que justifica la necesidad de incorporar esta técnica en la evaluación rutinaria de estos pacientes. La asociación de TnTc y NT-proBNP con DDVI sugiere que pueden ser utilizados como biomarcadores mínimamente invasivos de esta afectación. La ausencia de correlación entre DVI y ACS indica que las arritmias podrían deberse, no solo a una supuesta alteración estructural del miocardio, sino a un compromiso cardiaco independiente y temprano, que debe investigarse activamente incluso en pacientes asintomáticos sin FRCV.

