




El tratamiento de la tromboembolia pulmonar (TEP) aguda con riesgo de mortalidad intermedio-alto a los 30 días, sigue sin estar bien definido, recomendándose por las últimas guías clínicas de la European Society of Cardiology2019 el tratamiento anticoagulante exclusivamente, reduciendo la indicación de trombectomía mecánica a pacientes de riesgo alto o pacientes con riesgo intermedio-alto con mala evolución hemodinámica. Nuestro objetivo fue comprobar la mejoría ecocardiográfica, respiratoria y hemodinámica en las primeras horas de los pacientes sometidos a trombectomía mecánica con tromboembolia pulmonar de riesgo intermedio-alto.
Material y métodosSe analizó la evolución cardíaca por ecocardiografía (diámetro de ventrículo derecho, TAPSE, Onda S e hipertensión pulmonar), hemodinámica, respiratoria y clínica de los pacientes en las primeras 24 horas tras trombectomía mecánica por aspiración, así como las complicaciones hemorrágicas y mortalidad del procedimiento.
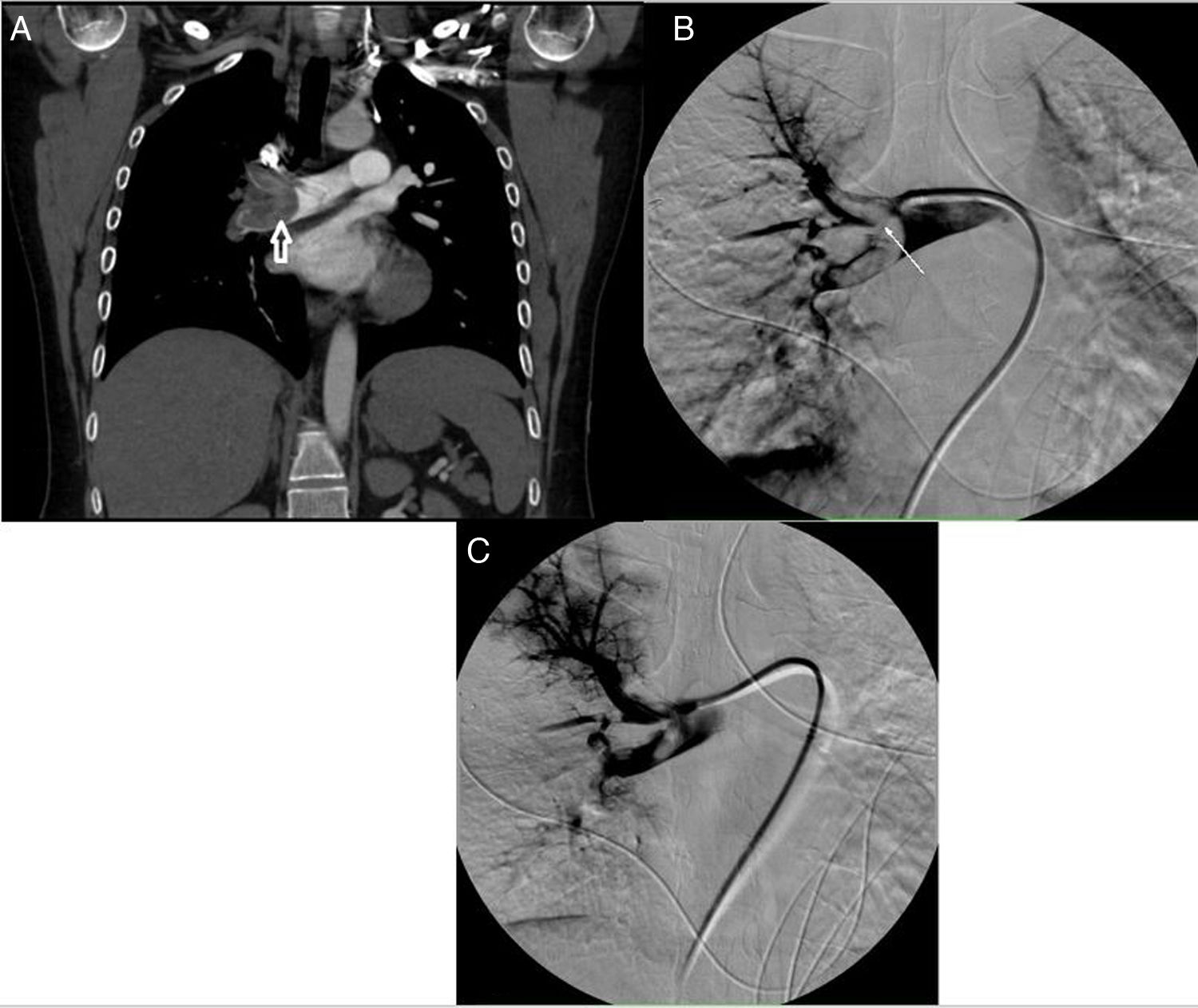
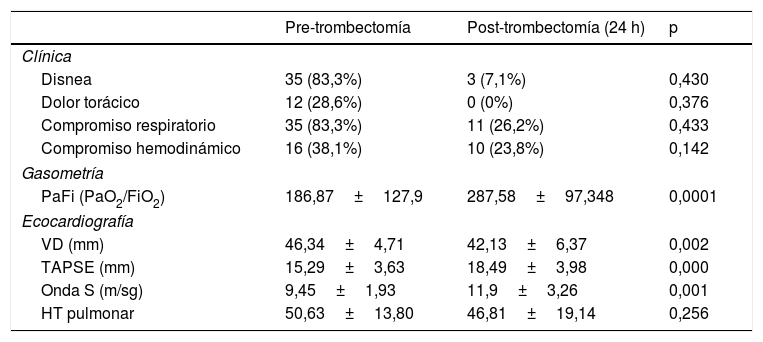
ResultadosSe llevaron a cabo 42 trombectomías mecánicas, 16 con inestabilidad hemodinámica (TEP masivo) y 26 estables hemodinámicamente (TEP submasivo). Se obtuvo mejoría (p<0,05) en el diámetro de ventrículo derecho, TAPSE, Onda S y presión arterial oxígeno/fracción inspiratoria de oxígeno (PaFi). Ocho pacientes recibieron tratamiento fibrinolítico, presentando 4 de ellos (50%) complicaciones hemorrágicas. Solo un paciente presentó complicación directa por el procedimiento (rotura arteria pulmonar). Ocho pacientes fallecieron en la fase aguda de la enfermedad.
ConclusionesLa trombectomía mecánica por aspiración es una técnica segura y efectiva, observando una mejoría de la situación respiratoria, hemodinámica y ecocardiográfica de los pacientes en las primeras 24 horas postprocedimiento con baja tasa de complicaciones frente al tratamiento fibrinolítico.
The treatment of acute pulmonary embolism (PE) with an intermediate-high risk of mortality at 30 days is still not well defined, recommending the latest clinical guidelines of the European Society of Cardiology 2019 exclusively anticoagulant treatment, reducing the indication for mechanical thrombectomy to high-risk patients or intermediate-high risk patients with poor hemodynamic evolution. Our purpose is to determine the safety and efficacy of aspiration thrombectomy in intermediate-high risk patients with PE and to analyze possible differences in these results between hemodynamically unstable patients (massive PE) and hemodynamically stable patients (submassive PE).
MethodsWe analyzed all patients who underwent aspiration thrombectomy for PE at our tertiary university hospital during a 34-month period. We compared echocardiographic parameters (right ventricular diameter, tricuspid plane annular plane systolic excursion (TAPSE), S′ wave, and pulmonary hypertension), respiratory parameters (PaO2/FiO2 ratio), and clinical parameters recorded before and 24h after the procedure. We also analyzed bleeding complications and mortality.
ResultsIn the 42 patients included (16 with massive PE and 26 with submassive PE), aspiration thrombectomy resulted in significant improvements in right ventricular diameter, TAPSE, S′ wave, andPaO2/FiO2 ratio. Of the 8 patients administered fibrinolysis, 4 developed bleeding complications. Only one direct complication of the procedure was observed (pulmonary artery rupture). Eight patients died in the acute phase.
ConclusionsAspiration thrombectomy for PE is safe and effective, significantly improving respiratory and hemodynamic parameters in the first 24h after the procedure with a low rate of complications compared to fibrinolysis.
