




In multiple sclerosis (MS), fetal exposure to DME carries varying degrees of risk. We aim to analyze the clinical and obstetric outcomes of MS patients (MSp) exposed to DMDs during pregnancy.
MethodsObservational study. We analyzed clinical-obstetric data of a cohort MSp, who became pregnant between 2007-2017. They were prospectively followed during pregnancy and postpartum. Control group: healthy pregnant women (HPW).
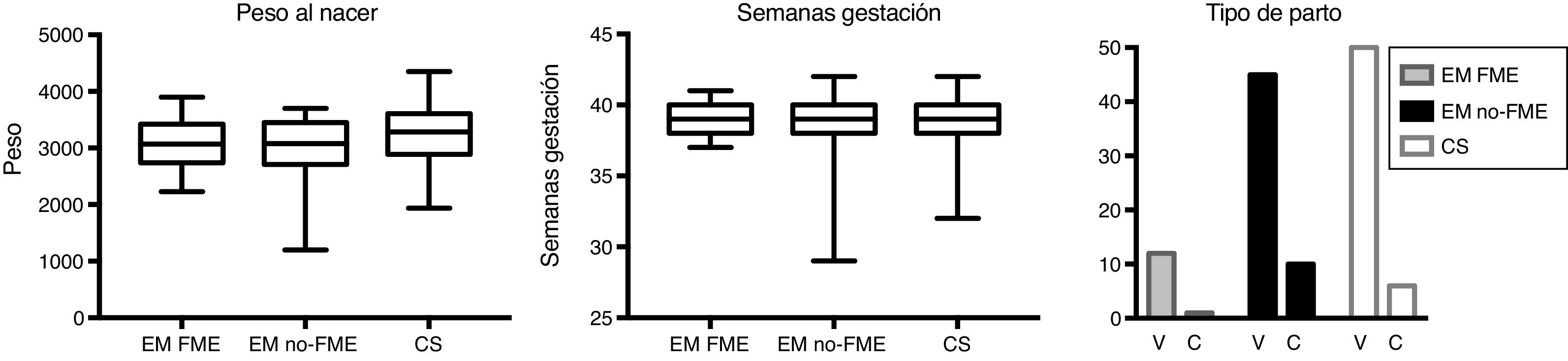
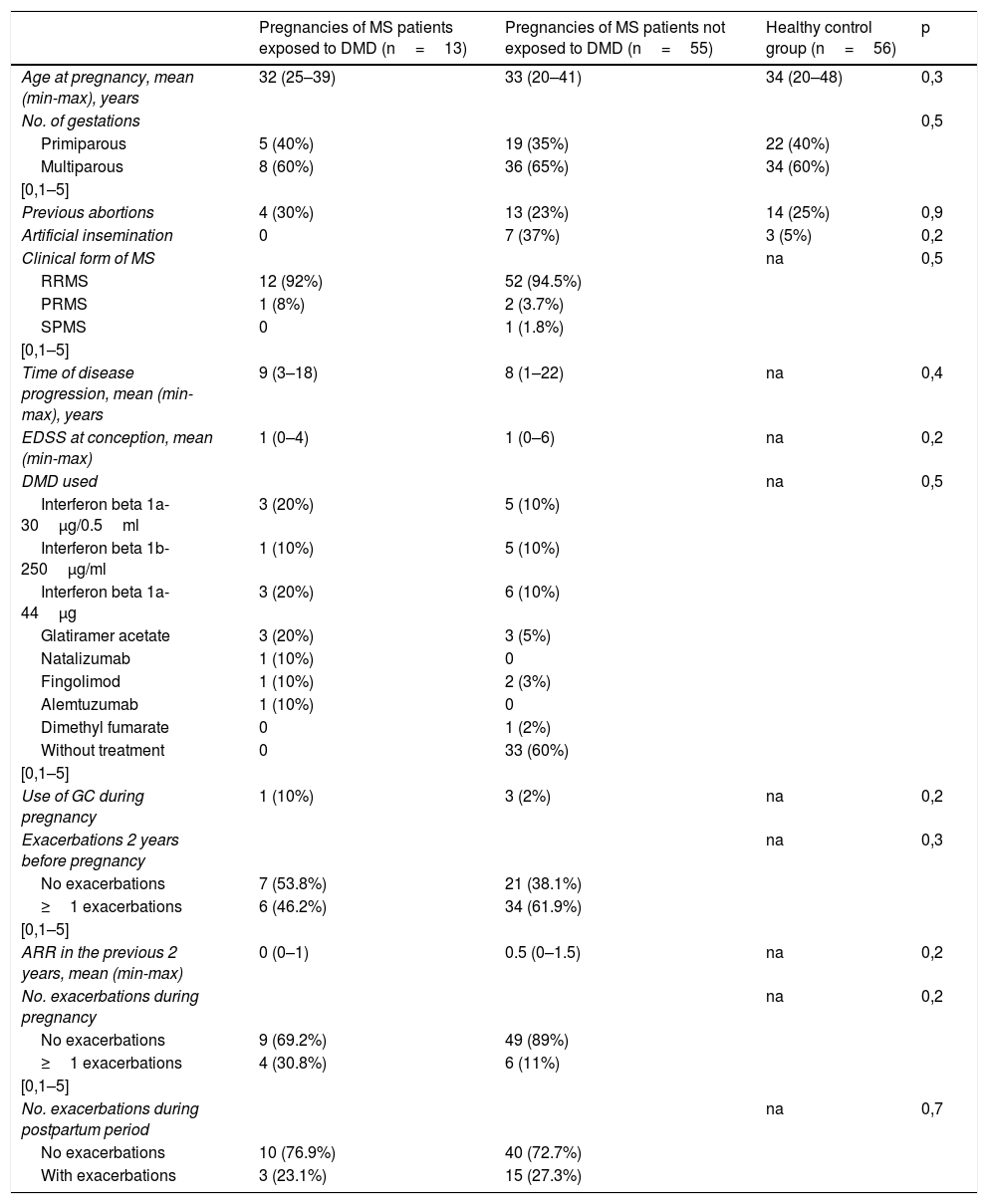
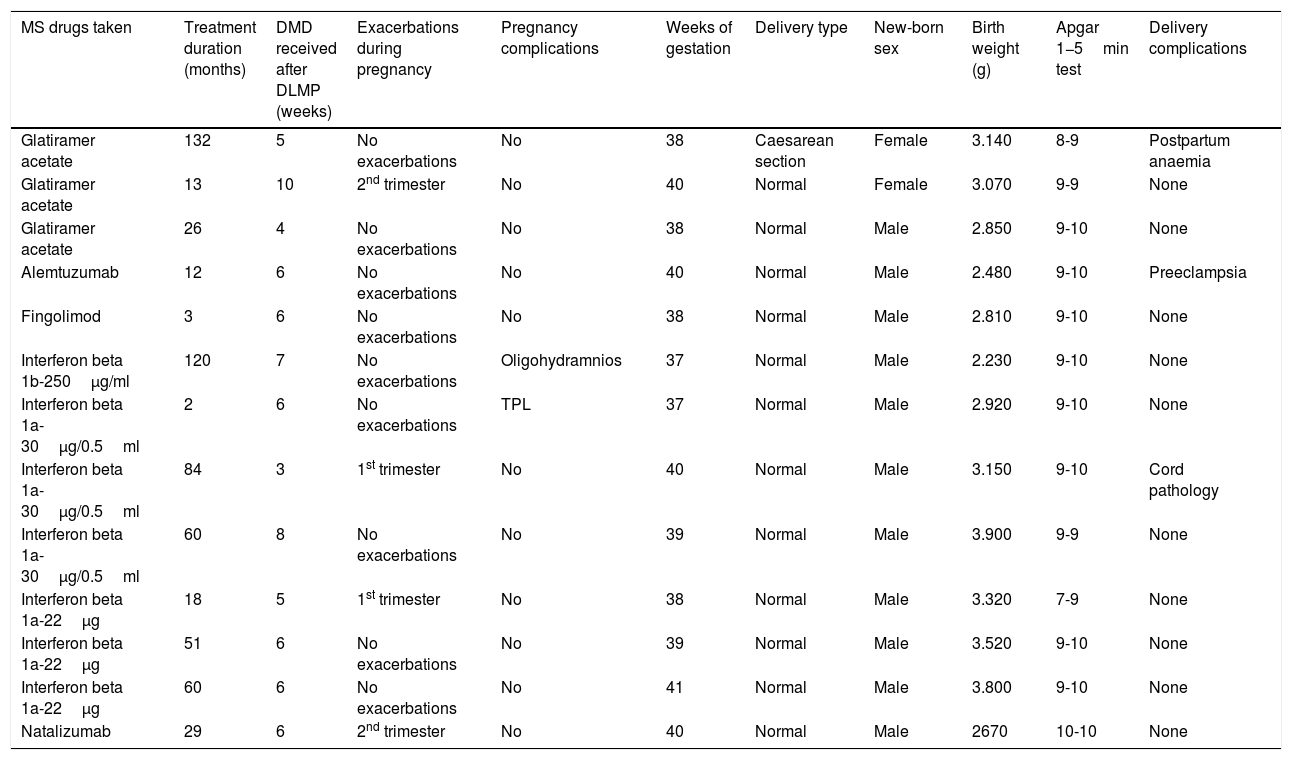
ResultsSixty-eight pregnancies in MSp. Fifty-six HPW. Thirteen MSp were exposed to DMDs during pregnancy. Obstetric outcome: 2(15%) infants had low birth weight, no preterm deliveries. Fifty-five MSp were not exposed to DMDs: 22(40%) discontinued DMD before pregnancy, 33(60%) naïve. Five infants (9%) had low birth weight and 7(12%) were preterm. HPW: 56. Low birth weight 6 (11%), preterm delivery 6 (11%). There were no differences in relapse incidence during pregnancy-puerperium between MSp groups. There were no differences in birth weight, gestation time, delivery-cesarean section. We found no special obstetric morbidity in women exposed to DMDs.
ConclusionsThere were no significant differences in the clinical and obstetric variables analyzed between pregnant women exposed to DMDs, unexposed, and HPW.
En esclerosis múltiple (EM), la exposición fetal a fármacos modificadores de la enfermedad (FME) conlleva distintos grados de riesgo. Objetivo: analizar nuestra experiencia en relación a los casos de exposición fetal involuntaria a FME.
Pacientes y métodosEstudio observacional. Se analizaron los datos clínico-obstétricos de una cohorte de pacientes con EM, entre 2007-2017. Grupo: pacientes con EM con embarazos expuestos a FME. Control: pacientes con EM no expuestas y embarazadas sanas.
Resultados68 embarazos en pacientes EM. Control: 56 mujeres sanas. Grupo EM expuestas a FME durante embarazo: 13, bajo peso al nacer: 2(15%), parto pretérmino 0. Grupo EM no expuestas a FME: 55. Veintidós (40%) suspendieron FME previo embarazo, 33 (60%) naïve. Bajo peso al nacer 5 (9%), pretérmino 7 (12%). Grupo mujeres sanas: bajo peso al nacer 6(11%), parto pretérmino 6(11%). No hubo diferencias clínicas estadísticamente significativas entre pacientes EM. Tampoco hubo diferencias en peso al nacer, tiempo gestación o morbilidad obstétrica en expuestas a FME.
ConclusionesNo hubo diferencias clínicas estadísticamente significativas, ni mayor morbilidad obstétrica, entre pacientes expuestas a FME, no expuestas y embarazadas sanas.

