



Colpocephaly (CC) can be observed in radiological findings from brain computed tomography (BCT) and magnetic resonance imaging (MRI). These images show dilated lateral ventricles, specifically in the occipital and temporal horns, and the third ventricle. Frontal horns retain their normal size. This type of hydrocephalus of the posterior half of the brain is a congenital malformation. It can be associated with myelocele, microgyria, cerebellar atrophy, total or partial absence of the corpus callosum, and other structural anomalies. Neurological manifestations occur mainly in children, and include cognitive and motor developmental delay, and epileptic seizures. Diagnosis in adult patients who have learned to perform activities of daily living normally is very infrequent. Imaging studies will show malformations, and differential diagnosis is required to rule out obstructive and non-obstructive ventriculomegaly.1–5 Case 1 is a 67-year-old man who presented sudden loss of consciousness with no seizures or loss of sphincter control. He regained consciousness, cognitive functions, and motor functions after 1 or 2minutes. According to his personal history, his developmental progression was normal and he had been working as administrative clerk until his retirement. Ten years before the event, he was diagnosed with arterial hypertension and had since been treated with enalapril dosed at 5mg twice a day. Clinical, cardiological, and neurological examinations did not show any abnormalities 2hours after the event, and neither did the electrocardiogram and blood test. The BCT performed in the emergency department revealed very pronounced posterior ventricular dilatation. The patient was then admitted for subsequent studies. A head MRI revealed CC and partial agenesis of the corpus callosum. The electroencephalogram did not show any abnormalities, thus ruling out adult onset of epileptic seizures.6 On the following day, cognitive tests and exploration of ideomotor, ideational, and limb-kinetic praxis showed normal results, and no interhemispheric disconnection syndrome could be detected.7,8 A lumbar puncture did not reveal any inflammatory or infectious processes. Given the normal structure of frontal ventricles, we ruled out normal pressure hydrocephalus (gait, sphincter control, and cognition were unaltered). The transient nature of the clinical manifestation led us to consider syncope as the probable diagnosis, regardless of any brain malformations. Fig. 1 shows findings of CC and agenesis of the corpus callosum. Case 2 is a 60-year-old man admitted to our hospital due to respiratory tract infection. He presented confusional syndrome during a hyperthermic episode. Throughout the patient's personal history, he had been independent for activities of daily living and was able to work satisfactorily as keeper and doorman in a condominium. A neurological examination of motor function and cranial nerves yielded no anomalous results. Cardiological examination and blood count results were also within normal limits. No inflammatory activity was detected in CSF extracted by lumbar puncture. A head MRI revealed CC and partial agenesis of the corpus callosum (Fig. 2). Once hyperthermia and the confusional syndrome had resolved, cognitive and praxis assessments yielded normal results, as in case 1. The patient was discharged after one week of hospitalisation. He displayed normal gait and sphincter control, which ruled out normal pressure hydrocephalus. As in the other case, our clinical assessment did not link cerebral malformation to the confusional syndrome. In both cases, the posterior to anterior ratio described by Noorani et al.4 was higher than 3 (CC), indicating a larger diameter of occipital ventricles than of frontal ventricles. In case 1, frontal sulci were found to be strikingly smaller than those in the posterior half of the brain, but no frontal microgyria could be diagnosed. An examination of these cases admitted in 2013 found no other similar cases in the hospital's records in the preceding 30 years. Whipple disease was considered in both cases since it can cause symmetric or asymmetric hydrocephalus. However, no history of this disease was reported for either patient, and CSF analysis showed normal results.9 A recently published study reported the case of an 88-year-old patient diagnosed with agenesis of the corpus callosum and CC. The patient had been asymptomatic until that moment, and the absence of clinical symptoms related to his malformations was thought to be due to neuroplasticity.10 CC is a congenital malformation which causes enlargement of the posterior half of the brain ventricles; it is frequently associated with total or partial agenesis of the corpus callosum. Manifestations are heterogeneous during childhood, but CC can also manifest incidentally in asymptomatic adults. Differential diagnosis to rule out normal pressure hydrocephalus should be performed before proceeding to surgical treatment, since the marked difference in diameter between the occipital and frontal ventricles will help identify the congenital malformation.
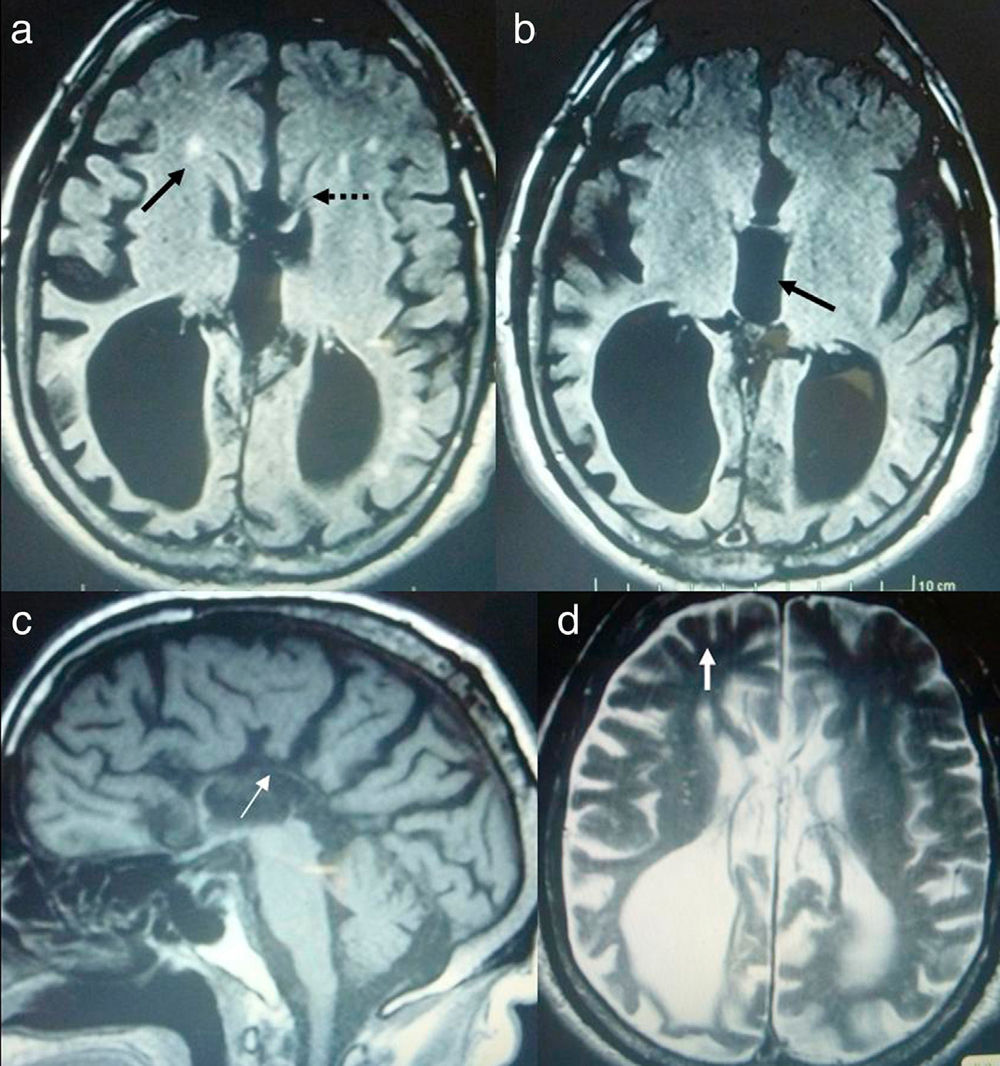
 Axial FLAIR sequence. Frontal ventricles (dotted arrow) are small, and the frontal parenchyma features small hyperintense images (arrow) that could be associated with arterial hypertension. The third ventricle and occipital horns are dilated (CC). b) Axial FLAIR sequence. The third ventricle appears dilated (arrow) and the upper part of the corpus callosum is very thin. c) T1-weighted sagittal slice: the genu and trunk of the corpus callosum (arrow) seem faint. The fourth ventricle is normal-sized. d) T2-weighted axial slice. Frontal sulci are much smaller than cortical sulci on the posterior part of the brain.")
Head MRI scan of case 1. a) Axial FLAIR sequence. Frontal ventricles (dotted arrow) are small, and the frontal parenchyma features small hyperintense images (arrow) that could be associated with arterial hypertension. The third ventricle and occipital horns are dilated (CC). b) Axial FLAIR sequence. The third ventricle appears dilated (arrow) and the upper part of the corpus callosum is very thin. c) T1-weighted sagittal slice: the genu and trunk of the corpus callosum (arrow) seem faint. The fourth ventricle is normal-sized. d) T2-weighted axial slice. Frontal sulci are much smaller than cortical sulci on the posterior part of the brain.
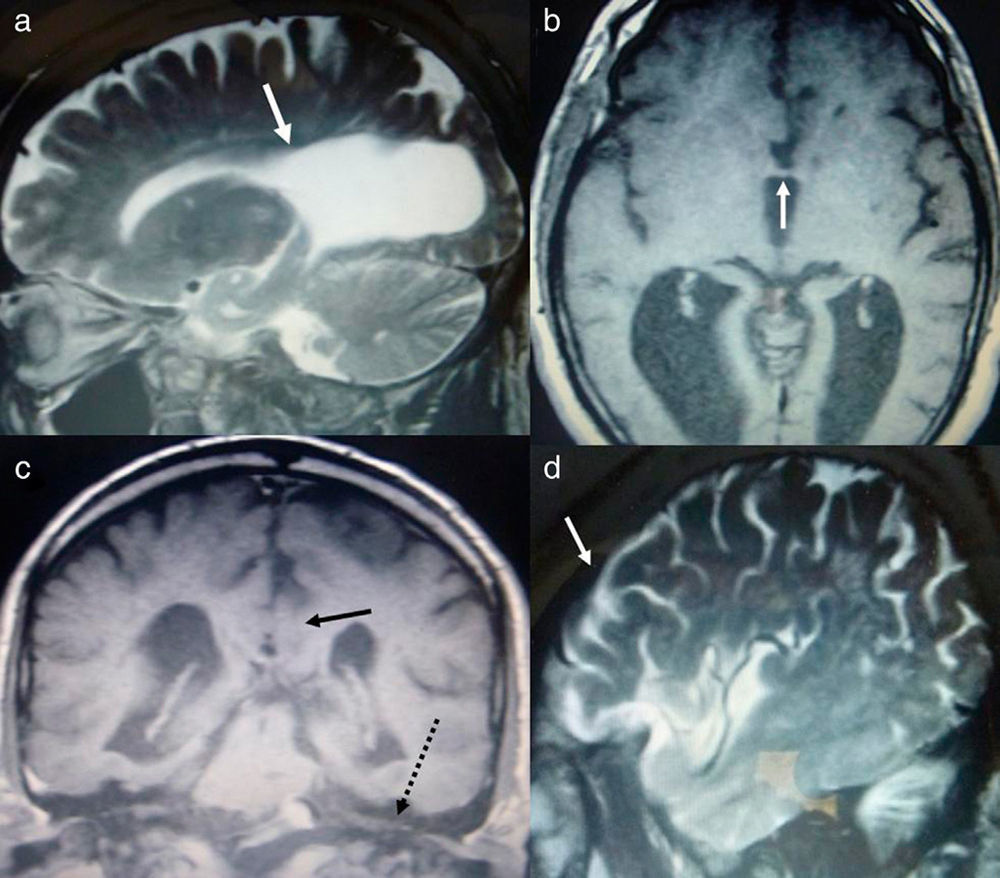
 T2-weighted sagittal sequence. We can observe a great difference in size between the normal anterior horn of the lateral ventricle and the very enlarged portion (from the arrow onwards) in the occipital region. b) T1-weighted axial slice. View of the third ventricle with an arrow indicating the thin genu of the corpus callosum. c) T1-weighted coronal slice. The splenium of the corpus callosum (arrow) is shown crossing the midline at the posterior fossa level (dotted arrow over the cerebellar tentorium). d) T2-weighted sagittal slice: Frontal and occipital cortical sulci show similar degrees of dilatation, unlike in case 1.")
Head MRI scan of case 2. a) T2-weighted sagittal sequence. We can observe a great difference in size between the normal anterior horn of the lateral ventricle and the very enlarged portion (from the arrow onwards) in the occipital region. b) T1-weighted axial slice. View of the third ventricle with an arrow indicating the thin genu of the corpus callosum. c) T1-weighted coronal slice. The splenium of the corpus callosum (arrow) is shown crossing the midline at the posterior fossa level (dotted arrow over the cerebellar tentorium). d) T2-weighted sagittal slice: Frontal and occipital cortical sulci show similar degrees of dilatation, unlike in case 1.
This study has not received funding from any sources. All authors are aware of the manuscript content and have approved it for publication.
Please cite this article as: Bartolomé EL, Cottura JC, Britos Frescia R, Domínguez RO. Colpocefalia y agenesia parcial de cuerpo calloso asintomáticos. Neurología. 2016;31:68–70.
