



Nervus intermedius neuralgia is a rare cause of facial and ear pain consisting of recurrent, short-lasting paroxysms of severe pain in the external auditory canal, auricula, and mastoid process, occasionally radiating to the temporoparietal region or the angle of the mandible. The condition may be accompanied by tearing and alterations in taste and salivation.1 Diagnosis is clinical, and can be challenging due to the location of the pain (which is similar to that of other neuralgias) and the occasional presence of such symptoms as tearing, which also occur in other headache disorders. Brain MRI helps to detect neurovascular compression and to rule out underlying processes that may cause neuralgia. Few studies have addressed the management of nervus intermedius neuralgia; pharmacological treatment constitutes the first line of treatment, followed by surgery (microvascular decompression or transection of the nervus intermedius and/or the geniculate ganglion) in refractory cases.2,3 No cases have been reported of the use of botulinum toxin to treat this entity. We describe the case of a patient with nervus intermedius neuralgia refractory to pharmacological treatment that was successfully managed with botulinum toxin.
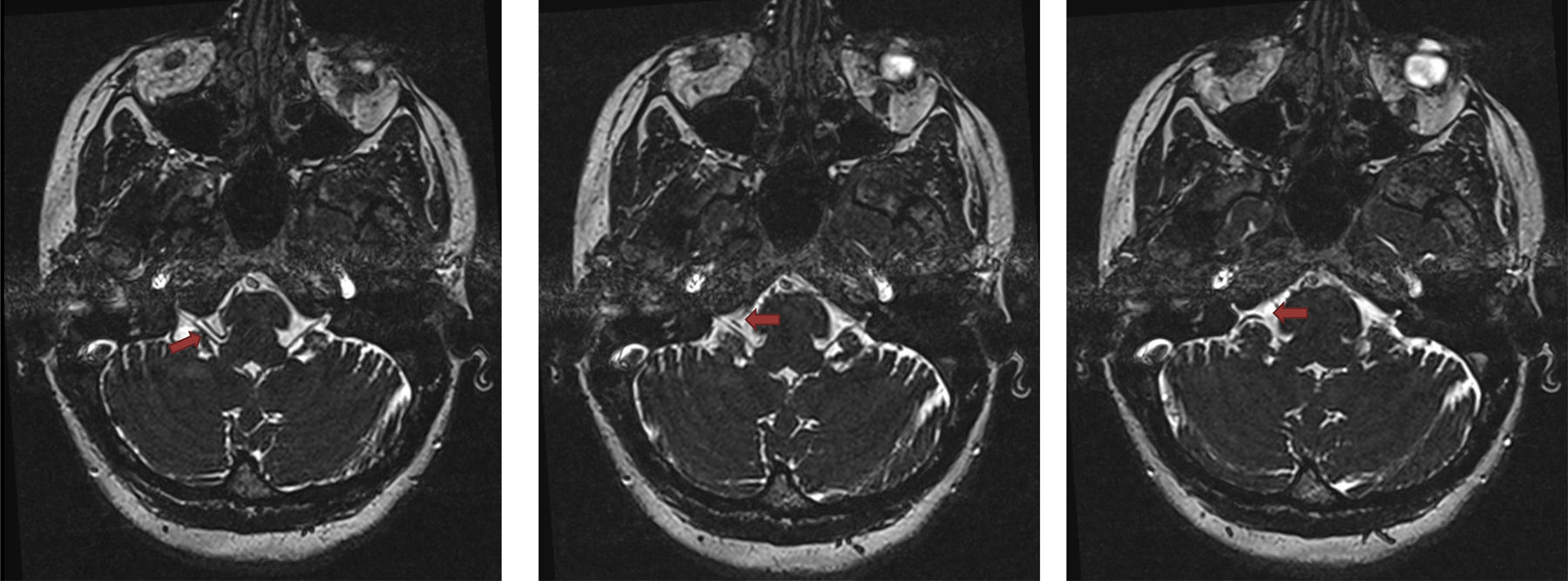
Our patient was a 43-year-old woman with 10-year history of idiopathic nervus intermedius neuralgia. She had received carbamazepine, pregabalin, lamotrigine, lacosamide, duloxetine, and nortriptyline at therapeutic doses, showing no response. She experienced 14-16 episodes per month of severe pain associated with a sensation of heat; episodes lasted several seconds and started deep inside the right external auditory canal, radiating to the mastoid process. Pain was sometimes triggered by touch in the periauricular area and was spontaneous on other occasions. The patient occasionally presented tearing. The neurological examination detected no alterations. A brain MRI study (3T scanner) revealed neurovascular compression involving the right glossopharyngeal nerve and the anterior inferior cerebellar artery (Fig. 1). The patient was diagnosed with idiopathic nervus intermedius neuralgia refractory to pharmacological treatment. We administered 50 IU of botulinum toxin type A (10 injection points, 5 IU per injection point) in the territory of the posterior auricular nerve (a branch of the facial nerve). She presented complete, sustained response for over 3 months, requiring no pharmacological treatment during that period. Pain reappeared after 3 months, and the patient again underwent botulinum toxin infiltration, again showing complete response.
 showing compression of the right glossopharyngeal nerve by the anterior inferior cerebellar artery.")
The MRI evidence of compression of the right glossopharyngeal nerve by the anterior inferior cerebellar artery was both a useful finding and a confounding factor, since the pain distribution and radiation observed in our patient are not typical of glossopharyngeal neuralgia but are typical of nervus intermedius neuralgia. Despite the value of brain MRI for the aetiological diagnosis of craniofacial neuralgias, the results should be interpreted with caution, as the diagnosis of these conditions is clinical.1 The associated symptoms (tearing in our patient) and the territory of radiation help in establishing a diagnosis.
Although botulinum toxin type A is known to be useful for treating such other neuralgias as trigeminal neuralgia,4,5 there is no published evidence of its use for nervus intermedius neuralgia. In the case of trigeminal neuralgia, the drug is thought to act on neurogenic inflammatory mediators and to mediate neurotransmitter release in sensory and autonomic nerve endings involved in pain.5 The same action mechanism may be involved in patients with nervus intermedius neuralgia. We wished to share our experience with botulinum toxin type A in this patient, since this treatment may be an intermediate step before resorting to surgery. Descriptive, analytical studies including larger samples should be conducted to evaluate the effectiveness and administration parameters (site, dose, and frequency of infiltration) of botulinum toxin for the treatment of nervus intermedius neuralgia.
FundingThis study has received no funding of any kind.
Please cite this article as: Erdocia-Goñi A, Hernando de la Bárcena I. Toxina botulínica tipo A en la neuralgia del nervio intermediario. Neurología. 2020;35:617–619.
