




Dear Editor:
Brain intraventricular (IVT) metastases by themselves are an exceedingly rare condition. Furthermore, IVT involvement in melanoma is unusual,1 as most cases of CNS metastases are intraparenchymal, leptomeningeal or dural. Until now, there have been very few published cases of IVT melanoma metastases and even less with histopathology.2 Herein, we report an excellently illustrated case of IVT, that contributes to the knowledge of this exceptionally rare condition.
An 88-year-old previously autonomous male was admitted in August 2020 to hospital due to epigastralgia, weight loss and mood disorder. During the previous 3 months, he had suffered from tremor, decline in cognitive and walking abilities and an 8 kg-weight loss. He had previously, among other conditions, undergone a surgical excision of a lumbar skin melanoma in 2015. He was re-operated and started with prembrolizumab treatment in 2017 due to local relapse. Mediastinal, and hiliar lymph node progression was suspected due to CT findings. No other systemic lesions were found then.
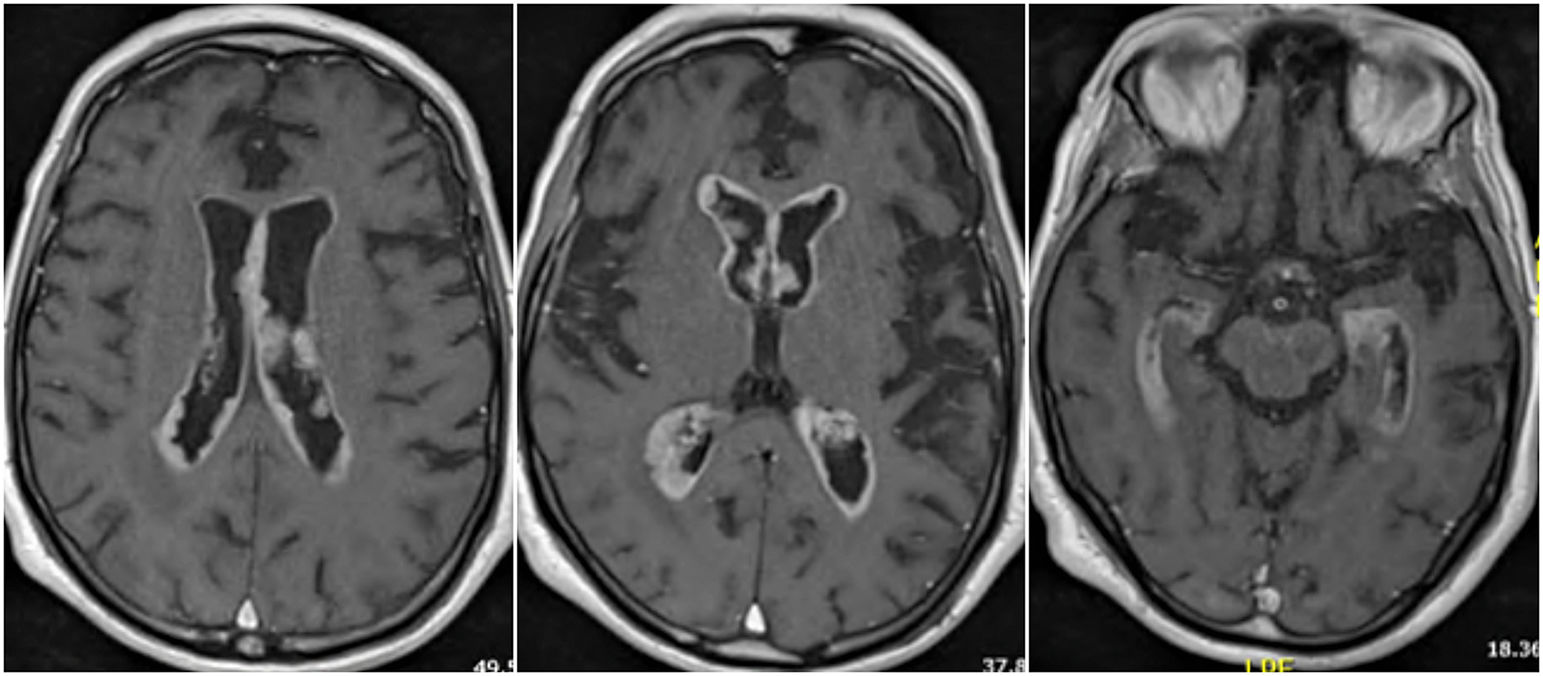
During neurological examination dysarthria, postural limb tremor with myoclonic interferences and cephalic myoclonus were found together with generalized increased tendon reflexes. The brain MRI images revealed an extensive pathological contrast uptake of the ependymal–subependymal surface, with variable and irregular thickness, throughout the infra- and supratentorial ventricular system (Fig. 1). No pachy- or leptomeningeal uptake of other brain parenchymal structures were observed. Blood analysis and toracoabdominal-pelvic CT scan were unremarkable. CFS examination revealed a lymphocytic predominant (83%) white blood cell count of 18/μL, a protein and ADA concentration of 266 mg/dL and 12,20 U/L; glucose, ACE and flow cytometry were normal. The microbiological research was negative, including tests for tuberculosis (mycobacterial culture, M.tuberculosis DNA and auramine stain), Toxoplasma gondii, Treponema pallidum, cryptococcus and virus (enterovirus, HSV-1, HSV-2, VZV and polyomavirus JC). CSF cytologic evaluation revealed an increased cellularity consisting mainly of lymphocytes and monocytes, and the presence of isolated epitheloid cells without striking atypical changes or mitosis. IHC study was inconclusive due to scarce material. The administration of pyracetam was effective for myoclonus and another lumbar puncture was planned to complete the IHC study.

Nevertheless, the patient's neurological and respiratory status rapidly declined. In order to avoid suffering and due to his foreseeable poor outcome, adequacy of therapeutic effort was decided, prioritizing comfort measures. After the patient's decease, autopsy was performed.
Post-mortem histopathological investigation demonstrated a metastatic IVT dissemination of a malignant melanoma covering the walls of the ventricular system and extending through all the horns and cavities, to the most caudal area of the bulb. The macroscopic examination (Fig. 2, A–B) revealed a brownish colored irregular lesion with an irregular internal surface of a multinodular appearance limited to the ventricular and subventricular area, without in-depth of the nervous parenchyma. Microscopic examination corresponded to an infiltrate of cells with malignant characteristics (large cells of epithelioid habit with large hyperchromatic nuclei, marked pleomorphism with areas of necrosis and abundant mitoses) that upholster the ventricular walls (Fig. 2, C–D). The lesion does not deeply infiltrate the white nor gray matter of the basal ganglia and the cortex. Some of these cells have a slight dun pigment. Tumor cells stained positively for S-100, melan-A and SOX-10, but negative for synaptophysin, CK(AE1/AE3) and GFAP (Fig. 2, E–F). No other organs were affected by metastases.

Histopathology of brain autopsy. A–B, Macroscopic examination demonstrates a granular brownish colored irregular lesion that lines the inner surface of the lateral ventricles bilaterally, including the septum pellucidum. C, H&E staining demonstrates a very cellular solid lesion with an ependymal–subependymal distribution that lines ventricular walls. D, H&E shows groupings of large cells with an epithelioid habit with large, oval and highly hyperchromatic nuclei, with a very marked pleomorphism and prominent nucleoli. There are abundant mitosis figures, necrotic areas, intense melanic pigment, and binucleated cells that are relatively common in melanoma. E, positive S-100 staining. F, positive melan-A staining
This case contributes to the characterization of this irregularly reported entity. However, despite being infrequent, melanoma metastases should always be considered in case of IVT lesions. Moreover, our patient's history illustrates the high risk of rapid deterioration and poor prognosis of this condition. Thus, we highlight the need for registration of this disease, in order to define a clear diagnosis and treatment guideline.
Ethical considerationsWe declare that we followed our centre's protocols on the publication of patient data.
Conflict of interestThe authors have no conflicts of interest to declare.
