






The long-term primary patency rates for percutaneous transluminal angioplasty using first and second generation stents for the treatment of the popliteal artery have been disappointing. However, results with the new nitinol stents seem promising. Our objective was to evaluate short-term clinical outcomes using the superflexible nitinol stent in the treatment of atherosclerotic lesions in popliteal segments.
MethodsRetrospective longitudinal study conducted from April to December 2013. Population characteristics, procedure-related data and imaging tests were assessed at 6 months. Stent patency and limb salvage rates were obtained.
ResultsA total of 14 patients with mean age of 73 ± 11 years were included, of which 50% were male and 64.3% diabetic. All patients had trophic lesions in the treated limbs. The arteriographic lesions were classified according to the criteria of the Trans-Atlantic Inter-Society Consensus (TASC) criteria as TASC B and C inequal proportions. In the assessment of below-the-knee runoff, 78.6% of the patients had only one distal pervious artery, of which the fibular artery was the most frequently observed. The stent landing zone was the mid segment of the popliteal artery in 57.1% of the cases and the distal segment, crossing the knee joint, in the remaining patients. During the 6 month follow-up there were no stent fractures. The primary patency rate was 85.7% and the limb salvage rate was 100%.
ConclusionsIn our study, angioplasty using the super flexible nitinol stent demonstrated to be safe and effective for the treatment of atherosclerotic lesions of the popliteal artery.
Resultados do Uso de Stent de Nitinol Superflexível em Artérias Poplíteas
IntroduçãoAs taxas de patência primària no longo prazo para a angioplastia transluminal percutânea, com implante de stents de primeira e segunda geração, no tratamento da artéria poplítea, têm sido desapontadoras. No entanto, resultados com novos stents de nitinol parecem promissores. Nosso objetivo foi avaliar desfechos clínicos no curto prazo do uso de stents de nitinol superflexíveis no tratamento de lesoes ateroscleróticas nos segmentos poplíteos.
MétodosEstudo retrospectivo, longitudinal, realizado no período de abril a dezembro de 2013. Foram avaliados as características populacionais, os dados do procedimento e os exames de imagem aos 6 meses, sendo obtidas as taxas de patencia do stent e de salvamento de membro.
ResultadosIncluímos nesta análise, 14 pacientes, com idade de 73 ± 11 anos, 50% do sexo masculino e 64,3% diabéticos. Todos os pacientes apresentavam lesão trófica nos membros tratados. As lesões arteriografias foram classificadas pelo critério Trans-Atlantic Inter-Society Consensus (TASC) em B e C em igual proporção. Na avaliação do leito de escoamento, 78,6% dos pacientes possuíam apenas uma artéria pérvia, sendo a artéria fibular a mais frequentêmente observada. As zonas de aterrissagem dos stents foram o segmento mèdio da artéria poplítea em 57,1% dos casos e, nos demais, o segmento distal da artéria, cruzando a articulagao do joelho. Durante o seguimento de 6 meses, nao foram observadas fraturas dos stents. A taxa de patencia primària foi de 85,7% e a de salvamento do membro foi de 100%.
ConclusõesA angioplastia com uso de stent de nitinol superflexível demonstrou ser segura e efetiva no tratamento das lesoes ateroscleróticas da artéria poplítea.
Lower-limb revascularization with the use of stents for the treatment of peripheral obstructive arterial disease (POAD) is usually restricted to segments not submitted to external compression, or to regions without mobility, due to the complex mechanisms of forces acting on the vessels, with generation of considerable biomechanical stress, especially in the popliteal artery.1 Even today, the results are not ideal, with stents of first and second generation showing patency rates below those of conventional surgical treatment. The rates of stent fracture, when the device is implanted in the popliteal artery, range from zero to 65% in different cohorts.2
A new generation of more flexible and resistant stents3,4 has shown comparable results, in the short-and medium-term, versus surgical treatment, which is still considered the standard technique for the treatment of these lesions.1 With the development of third-generation superflexible stents, endoluminal therapy has increasingly replaced surgical revascularization.4–6
This study aimed to evaluate the clinical outcomes in the short-term use of superflexible nitinol stents in the treatment of atherosclerotic lesions of popliteal segments.
METHODSStudy typeThis was a retrospective, longitudinal, observational study in a referral center for cardiovascular diseases, conducted in the period from April to December 2013. A total of 66 patients underwent angioplasty with stenting of the lower limbs, with 14 cases in the popliteal artery.
Inclusion and exclusion criteriaPatients of both genders, with limiting intermittent claudication, pain at rest in the affected limb or with ipsilateral trophic lesion, and with lesions restricted to the popliteal artery and the presence of at least one leg artery for distal run-off, were treated. Patients with creatinine clearance < 30 mL/kg/min, history of severe allergy to iodinated contrasts, and those with significant atherosclerotic disease in aortoiliac and/or femoral territories were excluded from the procedures.
Preoperative arteriography was used to classify the lesions according to: (1) the Trans-Atlantic Inter-Society Consensus II (TASC-II) 7 criteria: A, B, C, or D (Box); (2) type of lesion: stenosis, occlusion, dissection, or restenosis; and (3) location relative to the articular line: proximal, middle, or distal (Figure 1).
A Lesions that produce the best results and that should be treated by endovascular route.
B Lesions that produce sufficiently good results with endovascular methods, so that this is still the preferred approach, unless surgical revascularization is required to treat other lesions in the same anatomic area.
C Lesions exhibiting superior long-term results with surgery, so that endovascular methods should be used only in patients at high surgical risk.
D Lesions that do not produce good enough results with endovascular methods to justify them as primary treatment.

Schematic representation of the segments of popliteal artery. P1 corresponds to the proximal segment, from the channel of adductor muscles to the upper border of patella; P2 is the middle segment, from the upper border of patella to the joint line; P3 corresponds to the distal segment, from the joint line to the emergence of anterior tibial artery.
All procedures were performed by the same team at the Hemodynamics Laboratory, Center for Endovascular Interventions, Instituto Dante Pazzanese de Cardiologia.
Clopidogrel (75 mg/day) and acetylsalicylic acid (100 mg) were started at least three days before the procedure. Clopidogrel was maintained for at least 30 days and acetylsalicylic acid was maintained indefinitely.
The participants were treated with local anesthetic, and antimicrobial prophylaxis was performed with 1.5g of cefuroxime immediately before the beginning of the procedure. Radiographic control was obtained with an AXIOM Artis Flat Panel device (Siemens Healthcare Sector, Forchheim, Germany) or in a hybrid room with a Zeego Artis device (Siemens Healthcare Sector, Forchheim, Germany).
The approach was preferentially performed through the ipsilateral common femoral artery, with anterograde puncture, using a Prelude® (Merit Medial Systems, South Jordan, United States) 6F valved sheath. In the case of impossibility of using this access route, or when it was not possible to cross the target lesion, a retrograde access by puncturing one of the leg arteries was chosen, with a Prelude®4F valved sheath. 5F MPA-1 and/or 4F STR diagnostic catheters (Cordis Corporation, Warren, United States) were used, and the crossing of target lesions was performed by luminal or sub-intimal route, with the help of a Radiofocus® (Terumo Interventional Systems, Somerset, United States) hydrophilic guide wire (wire size, 0.035″ × 150 cm). Pre-dilation was conducted in cases of occlusion, or when a proper positioning of the stent was not possible. In all cases, the sinus-SuperFlex® (Optimed, Ettlingen, Germany) nitinol stent was used (Figure 2).
 Digital subtraction arteriogram showing occlusion of popliteal artery with distal filling in the interline. (B) Pre-dilation. (C) Positioning of the stent in the distal segment of popliteal artery. (D) Final arteriogram with return of axial flow. (E) Arteriography in leg flexion, without exhibiting kinking or blood flow-limiting injuries.")
Angioplasty of popliteal artery with landing zone in the distal segment of this artery. (A) Digital subtraction arteriogram showing occlusion of popliteal artery with distal filling in the interline. (B) Pre-dilation. (C) Positioning of the stent in the distal segment of popliteal artery. (D) Final arteriogram with return of axial flow. (E) Arteriography in leg flexion, without exhibiting kinking or blood flow-limiting injuries.
In all cases, the immediate postoperative period occurred in the ward, and local hemostasis was performed with manual compression for 30 minutes.
Postoperative follow-upThe follow-up was performed with outpatient evaluation, consisting of physical examination and ankle-brachial index (ABI) determination at 15, 30, 90, and 180 days after angioplasty. The control with Doppler ultrasound (USG-D) was performed at 30, 90, and 180 days after surgery, with the aim of identifying restenoses (Figure 3). Radiographs of the knee joint in posteroanterior (PA) and lateral views were performed at 30 and 180 days, with the aim of identifying stent fractures (Figure 4).
 Color-mode image without signs suggestive of stent fracture. (B) Color-mode image, showing laminar flow without vortices and no signs of neointimal hyperplasia. (C) Doppler Ultrasound demonstrating spectral curve of speed in native artery. (D) Doppler Ultrasound demonstrating spectral curve of intra-stent speed with a velocity of 70 cm/s and a speed ratio of 1.")
Ultrasonographic control at 6 months of stenting in the middle segment of popliteal artery. (A) Color-mode image without signs suggestive of stent fracture. (B) Color-mode image, showing laminar flow without vortices and no signs of neointimal hyperplasia. (C) Doppler Ultrasound demonstrating spectral curve of speed in native artery. (D) Doppler Ultrasound demonstrating spectral curve of intra-stent speed with a velocity of 70 cm/s and a speed ratio of 1.
 Radiography of knee in semi-flexion, with no signs of stent twisting or fracture. (B) Radiography of knee in posteroanterior view and with no signs of fracture. (C) Radiography of knee without evidence of compression at the level of adductor canal.")
The analyzed outcomes were: (1) immediate technical success, when the target lesion was treated in the manner previously planned, with residual lesion < 30% in the angiographic control; (2) primary patency, indicating an uninterrupted permeability after the revascularization procedure; and assisted primary patency, indicating cases where a new percutaneous intervention was applied, in order to prevent the impending occlusion or the progression of stenosis; (3) perioperative morbidity/mortality, for complications and deaths recorded for up to 30 days postoperatively; (4) major amputation: transfemoral and transtibial amputations; (5) restenoses, for in-stent lesions > 50% detected with USG-D, with peak systolic velocity > 200 cm/s or a pre-and post-stenosis rate ≥ 2; (6) fractures, for disconnection or twisting of stent meshes; and (7) rate of limb salvage.
RESULTSFourteen patients with symptomatic POAD, treated with primary angioplasty (without employing other adjuvant methods of arterial unblocking) with stent implantation in popliteal arteries, were included in the study.
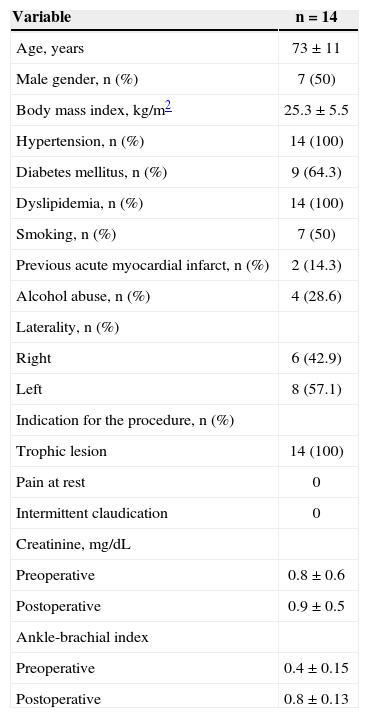
Characteristics of the populationThe demographic characteristics, comorbidities, and indications for treatment are described in Table 1. Mean age was 73 ± 11 years, 50% of patients were male, and approximately two-thirds were diabetic. The left leg was the most frequently treated limb (57.1%) and all patients had trophic lesions with tissue loss. Patients with intermittent claudication or pain at rest were not treated.
Baseline clinical characteristics
| Variable | n = 14 |
|---|---|
| Age, years | 73 ± 11 |
| Male gender, n (%) | 7 (50) |
| Body mass index, kg/m2 | 25.3 ± 5.5 |
| Hypertension, n (%) | 14 (100) |
| Diabetes mellitus, n (%) | 9 (64.3) |
| Dyslipidemia, n (%) | 14 (100) |
| Smoking, n (%) | 7 (50) |
| Previous acute myocardial infarct, n (%) | 2 (14.3) |
| Alcohol abuse, n (%) | 4 (28.6) |
| Laterality, n (%) | |
| Right | 6 (42.9) |
| Left | 8 (57.1) |
| Indication for the procedure, n (%) | |
| Trophic lesion | 14 (100) |
| Pain at rest | 0 |
| Intermittent claudication | 0 |
| Creatinine, mg/dL | |
| Preoperative | 0.8 ± 0.6 |
| Postoperative | 0.9 ± 0.5 |
| Ankle-brachial index | |
| Preoperative | 0.4 ± 0.15 |
| Postoperative | 0.8 ± 0.13 |
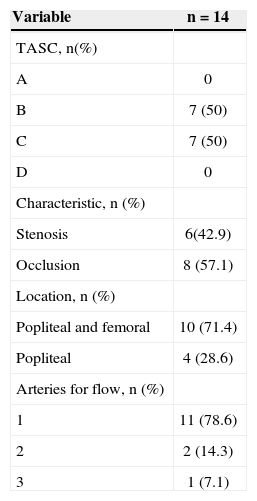
The lesions were classified into TASC B (50%) and C (50%). Regarding their location, 71.4% of cases were in the proximal segment of popliteal artery (P1), and in 28.6% of the cases were in middle or distal segments, in equal proportion (P2 and P3). In eight cases (57.1%), the stents were implanted in previously occluded vessels, with pre-dilation performed in all lesions.
In the evaluation of the run-off bed, the majority of patients had only one patent artery (78.6%) and the fibular artery was the most frequently observed. A mean of 1.3 ± 0.4 arteries by treated limb was obtained (Table 2).
Angiographic characteristics of lesions
| Variable | n = 14 |
|---|---|
| TASC, n(%) | |
| A | 0 |
| B | 7 (50) |
| C | 7 (50) |
| D | 0 |
| Characteristic, n (%) | |
| Stenosis | 6(42.9) |
| Occlusion | 8 (57.1) |
| Location, n (%) | |
| Popliteal and femoral | 10 (71.4) |
| Popliteal | 4 (28.6) |
| Arteries for flow, n (%) | |
| 1 | 11 (78.6) |
| 2 | 2 (14.3) |
| 3 | 1 (7.1) |
TASC: Trans-Atlantic Inter-Society Consensus II (TASC – II).7
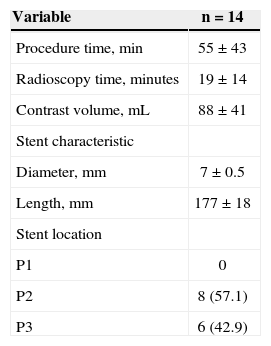
It was possible to achieve the target lesion revascularization in all cases with the use of one stent, obtaining technical success in 100%. The average extent of lesion coverage was 177 ± 18mm (120–200mm). Ten stents (71.4%) with a diameter of 6mm and four stents (28.6%) with a diameter of 5mm were used. There were no cases of intraoperative dissection or embolization. The areas of more frequent stent landing were the middle segment of popliteal artery (P2) in eight cases (57.1%) and the distal segment (P3) of the artery, crossing the joint knee, in six cases (42.9%). No implants occurred in the proximal segment (P1). Mean procedure times and of radioscopy were, respectively, 55 ± 43 minutes (range 20–240 min) and 19 ± 14 minutes (range 5–66 min). The mean volume of iodinated contrast used was 88 ± 41mL. In one case, a distal retrograde access by the dorsalis pedis artery was performed, thanks to the impossibility of crossing the target lesion by the anterograde technique. No complications with respect to the puncture site (Table 3) were observed.
Patient follow-upThe mean follow-up was 6.4 ± 2.1 months (range 3.2 to 8.4 months). There were no intraoperative or procedure-related deaths. Ninety days post-procedure, one elderly patient died due to cardiac complications.
The limb salvage rate was 100%. There was no major amputation during the follow-up. In three patients (21.4%), there was a development of their trophic lesions; two of these lesions were caused by in-stent stenoses in the 60th and 90th day of follow-up, and were treated by balloon dilation. The third injury occurred due to infectious complications, which resulted in a minor amputation. There was an increase of ABI, from 0.4 ± 0.15 preoperatively to 0.8 ± 0.13 at the time of hospital discharge.
The primary patency rate was 85.7% at 6 months. In two cases, it was necessary to perform a new balloon angioplasty for treatment of in-stent restenosis, with therapeutic success in only one case. This resulted in an assisted primary patency rate of 92.8% at follow-up. There were no stent fractures documented by radiographs of the knee joint.
DISCUSSIONThe management of atherosclerotic lesions in the segments of the popliteal artery near the knee joint represents a difficult endovascular approach, because of the biomechanical stresses occurring in this region. Complex rotational, tensile, compressive, and stretching forces act simultaneously on a short arterial segment and on the stent.8,9 For many years, these lesions were treated by surgical grafting using autologous vein, with rates of primary and secondary patency after 5 years of 63% to 75% and 80% to 83%, respectively, and with a perioperative mortality of 1% to 3%.10–12 However, these high patency and low mortality rates are accompanied by a considerable perioperative morbidity, as are the subsequent multiple surgical procedures and hospital readmissions.13
Currently, with the development and improvement of endovascular materials, the number of minimally invasive procedures for the treatment of popliteal lesions has increased. Generally, balloon angioplasty, or mechanical or laser arterectomy, are the preferred choices for the treatment of arterial lesions behind the knee, due to the lack of metallic devices capable of withstanding the forces exerted on this arterial segment.14,15 However, the efficacy of these techniques is limited.15
The first large study comparing treatment with balloon angioplasty versus stenting in the femoropopliteal segment was RESILENT2 (Randomized Study Comparing the Edwards Self-ExpandIng Lifestent versus Angioplasty Alone In LEsions INvolving The SFA and/or Proximal Popliteal Artery). During the first phase of this study, patients with intermittent claudication because of femoropopliteal occlusive lesions, with length < 15cm and diameter of the target vessel between 4 to 6.5 mm, were included. The results showed the superiority of the LifeStent® (Bard Peripheral Vascular, Tempe, United States) over balloon angioplasty in the femoropopliteal segment. In its second phase, 206 patients were included, when the treatment of more than one lesion was allowed, provided they did not exceed the length of 15cm. Its primary endpoint was the revascularization of the target vessel within 12 months. The result was a primary patency of 80% vs. 38% for the LifeStent® vs. balloon angioplasty, respectively.3
The choice of the stent depends on the anatomic characteristics of the lesion, such as its location and the extent of calcification, as well as the characteristics of the stent – its diameter, length, profile, flexibility, long-term durability, and resistance to fracture. The limitations to stent implant in the popliteal artery include insufficient radial force to maintain the patency of the vessel, and the possibility of folding and fractures of the device. Stent fracture is associated with high incidence of restenoses and occlusions. Scheinert et al.16 detected radiographically 64 fractures in 261 stents (24.5%) used in the treatment of femoropopliteal lesions. The primary patency rate obtained in the 12 months’ follow-up was significantly lower in patients with fracture (41.1% vs. 84.3%, p < 0.0001). In the present study, stent fractures detected by the same method were not observed.
Regarding the rate of primary patency, the results of several studies in the literature considered heterogeneous populations, also differing in the location of the segments treated. Chan et al.4 reported primary patency rates of the femoropopliteal stent implanted in the segment after six and 12 months of 83.5% and 78.6%, respectively, in 82 limbs treated with Supera® stent (IDEV Technologies Inc., Webster, United States). In the Durability-200 study, Bosiers et al.17 analyzed 100 patients, 71% of whom were treated for intermittent claudication and 29% treated for critical ischemia, with their injuries classified as TASC C and D, and used the devices in the femoropopliteal segment. These authors obtained a primary patency of 85.4% at 6 months and of 64.8% at 12 months. As for stents implanted in the popliteal segment, Kickuth et al.18 studied 35 patients with intermittent claudication and critical limb ischemia, in which auto-expandable nitinol stents were implanted in the popliteal artery. In 22 cases, stents were implanted in the distal portion of the popliteal artery, and in the other cases, in the tibiofibular trunk, with a primary patency rate of 82% and a limb salvage rate of 100%. In the present study, most stents were implanted in the middle segment, and in only six cases (42.9%), stents were implanted in the distal segment, crossing the joint line. A primary patency and an assisted primary patency of 85.7% and 92.8% were obtained, respectively, at the six-month follow-up, in a population consisting of patients with critical ischemia of Rutherford classes 5 and 6, and in arteriographic lesions classified as TASC B and C, with a similar rate of limb salvage.
During the clinical follow-up, there was improvement in ABI, from 0.4 ± 0.15 preoperatively to 0.8 ± 0.13 at the time of hospital discharge, as well as an improvement of trophic lesions in 78.6% of cases. The measurement of ABI may have been overestimated, due to the high prevalence of diabetes in our population (64.3%), considering that the predominance of arterial calcifications in the distal portions of leg arteries of diabetic people overestimates the mensuration of this index.
Study limitationsThe small number of cases, the heterogeneous group of segments treated in the popliteal artery, the short follow-up period, and the absence of an established algorithm for clinical follow-up may have influenced the results of this study. Finally, the accuracy of the results may have been affected by the retrospective data analysis.
CONCLUSIONSIn this study, it was demonstrated that angioplasty with use of a superflexible nitinol stent is a safe and effective procedure in the treatment of atherosclerotic lesions in popliteal arteries. The patency rates obtained in various segments of the popliteal artery treated demonstrate the need for a close clinical follow-up of these patients in the medium and long term.
CONFLICTS OF INTERESTThe authors declare no conflicts of interest.
FUNDING SOURCENone.