


Radial access is the object of increasing interest for interventional cardiologists, providing several advantages, including a reduction of bleeding and major adverse cardiovascular event (MACE) rates. However, even though elderly patients have a greater risk of access site bleedings, the use of the radial approach is controversial, due to the greater anatomical complexity of these patients.
MethodsRetrospective study including patients undergoing percutaneous coronary intervention (PCIs) using the radial access divided into an elderly (> 65 years) and a non-elderly (< 65 years) group. Clinical, angiographic and procedural characteristics as well as early and late follow-up outcomes were analyzed.
ResultsThe elderly group included 131 patients (145 PCIs) and the non-elderly group, 149 patients (176 PCIs). The elderly group presented lower body mass index and fewer smokers and higher rates of chronic renal failure, peripheral arterial disease, stable coronary artery disease, multivessel disease and calcified lesions. There was no difference in the rate of access-site crossover (4.8% vs. 3.4%), fluoroscopy time (15.3±10.3minutes vs. 16.1±10.3minutes), procedure time (40.6±26.4minutes vs 46.4±53.6minutes), angiographic (96.3% vs 97.5%) and clinical (94.5% vs 95.4%) success, MACE (3.4% vs 3.4%) and bleedings (0.21% vs 0.6%) during hospitalization. In the late follow-up there was no difference in the MACE rates (9.6% vs 11%).
ConclusionsDespite the greater clinical and angiographic complexity, PCI using the radial access is safe and effective, with a high procedural success rate and low in-hospital and late follow-up complication rates.
Intervenção Coronária Percutânea por Acesso Transradial em Pacientes Idosos vs. Não-Idosos
IntroduçãoA via radial é objeto de interesse crescente de cardiologistas intervencionistas, por oferecer diversas vantagens, entre elas a redução da taxa de sangramento e eventos cardíacos adversos maiores (ECAM). Entretanto, apesar de os idosos apresentarem maior risco de sangramento da via de acesso, a utilização da via radial é motivo de controvérsias, pela maior complexidade anatômica desses pacientes.
MétodosEstudo retrospectivo, que incluiu pacientes submetidos a intervenção coronária percutânea (ICP) por via radial, divididos nos grupos idoso (≥65 anos) e não-idoso (< 65 anos). Foram analisados os perfis clínico, angiográfico e do procedimento, além da evolução tanto inicial como tardia.
ResultadosNo grupo idoso foram incluídos 131 pacientes (145 ICPs) e no grupo não-idoso, 149 pacientes (176 ICPs). O grupo idoso apresentou mais frequentemente menor índice de massa corporal e de tabagistas, e maiores taxas de insuficiência renal crônica, doença arterial periférica, quadros clínicos estáveis, doença multiarterial e lesões calcificadas. Não houve diferença nas taxas de troca de via de acesso (4,8% vs. 3,4%), tempo de fluoroscopia (15,3±10,3 minutos vs. 16,1±10,3 minutos), tempo do procedimento (40,6±26,4 minutos vs. 46,4±53,6 minutos), sucesso tanto angiográfico (96,3% vs. 97,5%) como clínico (94,5% vs. 95,4%), ECAM (3,4% vs. 3,4%) e sangramentos (0,21% vs. 0,6%) na fase hospitalar. No seguimento tardio também não houve diferença nas taxas de ECAM (9,6% vs. 11%).
ConclusõesApesar da maior complexidade tanto clínica como angiográfica, a realização de ICP por via radial em idosos é segura e eficaz, com elevado índice de sucesso do procedimento e baixa taxa de complicações hospitalares e tardias.
The radial access approach has been the subject of increasing interest for diagnostic and therapeutic procedures worldwide and also in Brazil, since it has several advantages, such more convenience for the patient in the immediate post-procedure, with earlier return to activities, decreased hospitalisation time, with consequent reduction in hospital costs, and a low complication rate at the puncture site when compared with the femoral approach, reducing the rate of major bleeding, which, in turn, is associated with increased risk of death and ischemic events.1-4
This access is particularly important in scenarios associated with high risk of bleeding, such as acute coronary syndromes, in which the use of antiplatelet and antithrombotic therapies is more aggressive, in female patients, and in the elderly.5,6 However, radial access in the elderly may be a more difficult approach due to tortuosity and arterial stenosis.
This study aimed to evaluate the clinical, angiographic, and procedural profiles, as well as the initial and late evolution of elderly patients, when compared to non-elderly patients submitted to percutaneous coronary intervention (PCI) through radial access, in an unselected population representative of daily clinical practice.
METHODSThis was a retrospective study, which included all consecutive patients submitted to PCI through radial access from June of 2011 to December of 2012, divided into two groups: elderly (≥65years) and non-elderly (≤65years). Patients with chronic renal failure submitted to dialysis with fistula in the right upper limb and those in cardiogenic shock were excluded.
The radial artery puncture was performed with the patient with the right arm extended to the side and hand in the supine position, under local anaesthesia with 2 to 3mL of 2% lidocaine. A Jelco 20 catheter was used to puncture the artery; after puncture, 5F to 7F arterial sheaths were inserted, which were specific for the radial artery, with 11cm of length. After the procedure, the arterial sheath was removed in the operating room without heparin reversal, and a compression dressing was applied, which was usually removed two hours after the procedure.
All patients received a loading dose of 300mg acetylsalicylic acid and 600mg of clopidogrel, followed by a maintenance dose of 100mg and 75mg per day, respectively, as well as intravenous unfractionated heparin during the procedure, at a dose of 70 to 100 U/kg.
Patients were followed after hospital discharge, and follow-up occurred at one month, three months, six months, and one year through medical consultation or telephone contact. Bleeding was defined according to the criteria of the Thrombolysis in Myocardial Infarction study7 (TIMI; minimum: any clinical sign of bleeding associated with decrease in hemoglobin < 3g/dL; minor: any clinical signs of bleeding associated with a decrease in hemoglobin of 3g/dL to 5g/dL; and major: intracranial hemorrhage, sign of clinically significant bleeding associated with decrease in hemoglobin > 5g/dL, or fatal bleeding) and according to the criteria of the Bleeding Academic Research Consortium8 (BARC; type 0: no bleeding; type 1: minor bleeding not requiring medical attention or hospitalisation; type 2: any sign of bleeding that does not fit types 3, 4, or 5, but has at least one of the following criteria: non-surgical medical intervention, need for hospitalisation or increased level of care, requiring clinical assessment; type 3A: bleeding associated with a decrease in hemoglobin of 3g/dL to 5g/dL or bleeding requiring blood transfusion; type 3B: bleeding associated with a decrease in hemoglobin > 5g/dL, cardiac tamponade, bleeding requiring surgical treatment for control except dental/ nasal/skin/hemorrhoids or bleeding requiring the use of vasoactive drugs; type 3C: intracranial bleeding, except micro-bleeding or hemorrhagic transformation, different subcategories of bleeding confirmed by autopsy, imaging assessment or peritoneal lavage or intraocular bleeding that compromises vision; type 4: bleeding related to CABG; and type 5: fatal bleeding).
Major adverse cardiac events were defined as a combination of cardiac death, non-fatal acute myocardial infarction, or need for target-vessel revascularisation. The criterion of reinfarction after the procedure adopted was the TIMI,7 which considers that, for patients within 48 hours of the index procedure, three conditions must be present: documentation that creatine kinase MB fraction (CK-MB) was decreased (or total creatine phosphokinase [CPK] if CK-MB is not available), CK-MB obtained at least four hours after the procedure > three times the upper limit of normal (or total CPK, when CK-MB is not available), and increase in CK-MB of at least 50% of the previous value.
Angiographic success was defined as percentage of stenosis diameter < 30% with final TIMI 3 flow. Stent thrombosis was classified as acute, sub-acute, late, and very late, according to the criteria of the Academic Research Consortium (ARC).9
Statistical analysisContinuous variables were expressed as means and standard deviations and compared using Student’s t-test for independent samples. Qualitative variables were expressed as numbers and percentages and compared using the chi-squared or Fisher’s exact test, as appropriate. SPSS for Windows, version 12.0, was used for the statistical analyses, and a p-value < 0.05 was considered significant.
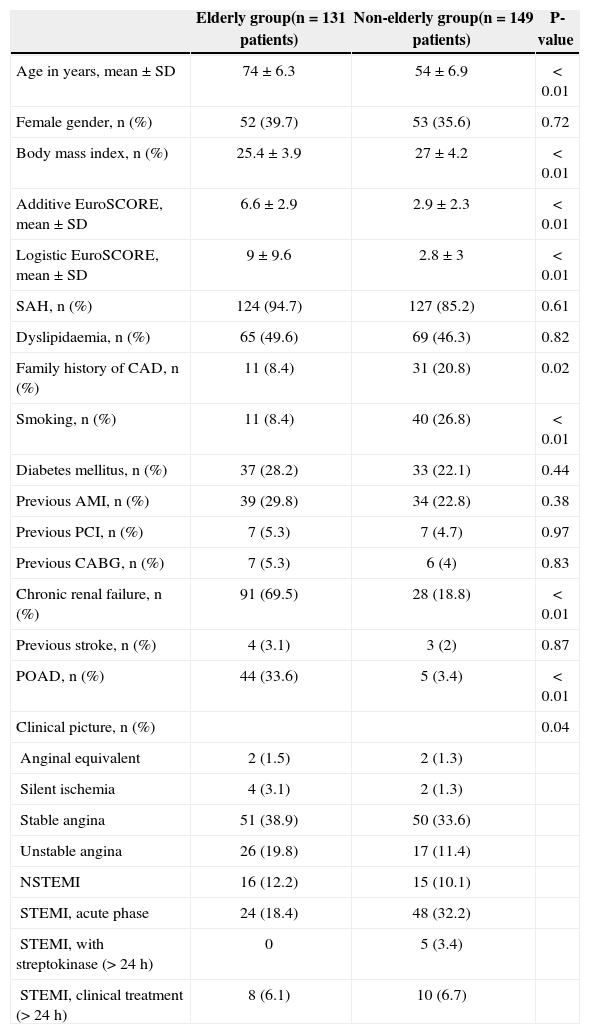
RESULTSFrom June of 2011 to December of 2012, 280 patients underwent 321 PCIs by radial access; 131 patients (145 PCIs) were categorized as elderly and 149 patients (176 PCIs) as non-elderly. The mean ages in the elderly and non-elderly groups were 74±6.3years and 54±6.9years, respectively. The elderly group had lower body mass index, fewer smokers, higher additive and logistic EuroSCORE, and higher incidence of chronic renal failure and peripheral artery disease (Table 1).
Clinical characteristics
| Elderly group(n=131 patients) | Non-elderly group(n=149 patients) | P-value | |
|---|---|---|---|
| Age in years, mean±SD | 74±6.3 | 54±6.9 | < 0.01 |
| Female gender, n (%) | 52 (39.7) | 53 (35.6) | 0.72 |
| Body mass index, n (%) | 25.4±3.9 | 27±4.2 | < 0.01 |
| Additive EuroSCORE, mean±SD | 6.6±2.9 | 2.9±2.3 | < 0.01 |
| Logistic EuroSCORE, mean±SD | 9±9.6 | 2.8±3 | < 0.01 |
| SAH, n (%) | 124 (94.7) | 127 (85.2) | 0.61 |
| Dyslipidaemia, n (%) | 65 (49.6) | 69 (46.3) | 0.82 |
| Family history of CAD, n (%) | 11 (8.4) | 31 (20.8) | 0.02 |
| Smoking, n (%) | 11 (8.4) | 40 (26.8) | < 0.01 |
| Diabetes mellitus, n (%) | 37 (28.2) | 33 (22.1) | 0.44 |
| Previous AMI, n (%) | 39 (29.8) | 34 (22.8) | 0.38 |
| Previous PCI, n (%) | 7 (5.3) | 7 (4.7) | 0.97 |
| Previous CABG, n (%) | 7 (5.3) | 6 (4) | 0.83 |
| Chronic renal failure, n (%) | 91 (69.5) | 28 (18.8) | < 0.01 |
| Previous stroke, n (%) | 4 (3.1) | 3 (2) | 0.87 |
| POAD, n (%) | 44 (33.6) | 5 (3.4) | < 0.01 |
| Clinical picture, n (%) | 0.04 | ||
| Anginal equivalent | 2 (1.5) | 2 (1.3) | |
| Silent ischemia | 4 (3.1) | 2 (1.3) | |
| Stable angina | 51 (38.9) | 50 (33.6) | |
| Unstable angina | 26 (19.8) | 17 (11.4) | |
| NSTEMI | 16 (12.2) | 15 (10.1) | |
| STEMI, acute phase | 24 (18.4) | 48 (32.2) | |
| STEMI, with streptokinase (> 24h) | 0 | 5 (3.4) | |
| STEMI, clinical treatment (> 24h) | 8 (6.1) | 10 (6.7) |
SAH, systemic arterial hypertension; CAD, coronary artery disease; AMI, acute myocardial infarction; PCI, percutaneous coronary intervention; CABG, coronary artery bypass grafting; POAD, peripheral obstructive artery disease; NSTEMI, non-ST segment elevation myocardial infarction; STEMI, ST-segment elevation myocardial infarction.
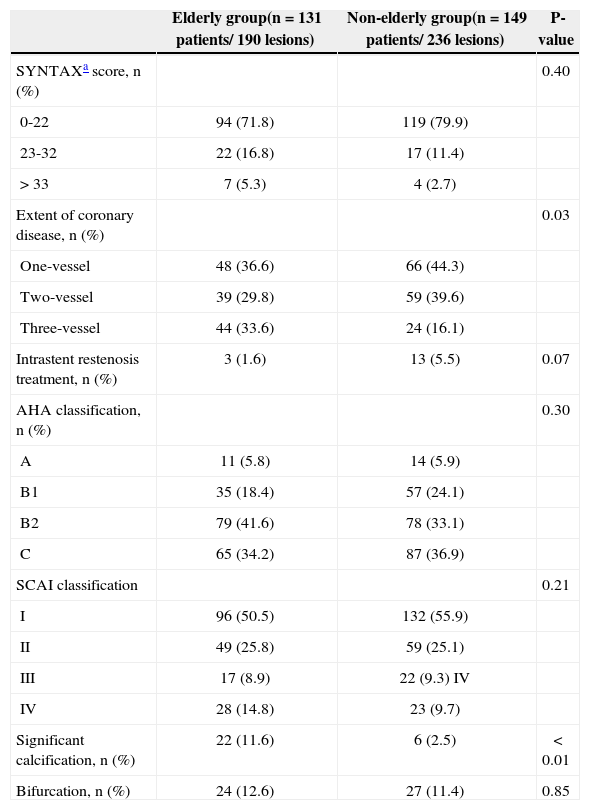
Regarding the angiographic characteristics, the only differences were the extent of coronary disease, most often three-vessel disease (33.6% vs. 16.1%), and severe coronary calcification (11.6% vs. 2.5%; P < 0.01) in the elderly group (Table 2).
Angiographic characteristics
| Elderly group(n=131 patients/ 190 lesions) | Non-elderly group(n=149 patients/ 236 lesions) | P-value | |
|---|---|---|---|
| SYNTAXa score, n (%) | 0.40 | ||
| 0-22 | 94 (71.8) | 119 (79.9) | |
| 23-32 | 22 (16.8) | 17 (11.4) | |
| > 33 | 7 (5.3) | 4 (2.7) | |
| Extent of coronary disease, n (%) | 0.03 | ||
| One-vessel | 48 (36.6) | 66 (44.3) | |
| Two-vessel | 39 (29.8) | 59 (39.6) | |
| Three-vessel | 44 (33.6) | 24 (16.1) | |
| Intrastent restenosis treatment, n (%) | 3 (1.6) | 13 (5.5) | 0.07 |
| AHA classification, n (%) | 0.30 | ||
| A | 11 (5.8) | 14 (5.9) | |
| B1 | 35 (18.4) | 57 (24.1) | |
| B2 | 79 (41.6) | 78 (33.1) | |
| C | 65 (34.2) | 87 (36.9) | |
| SCAI classification | 0.21 | ||
| I | 96 (50.5) | 132 (55.9) | |
| II | 49 (25.8) | 59 (25.1) | |
| III | 17 (8.9) | 22 (9.3) IV | |
| IV | 28 (14.8) | 23 (9.7) | |
| Significant calcification, n (%) | 22 (11.6) | 6 (2.5) | < 0.01 |
| Bifurcation, n (%) | 24 (12.6) | 27 (11.4) | 0.85 |
SYNTAX, [SALTO]; AHA, American Heart Association; SCAI, Society for Cardiac Angiography and Interventions.
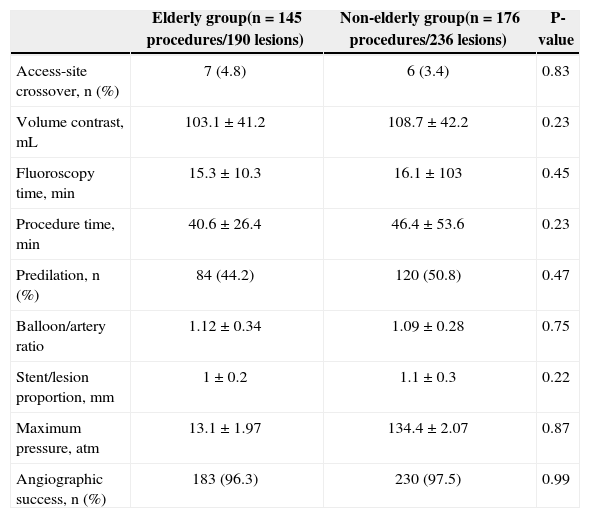
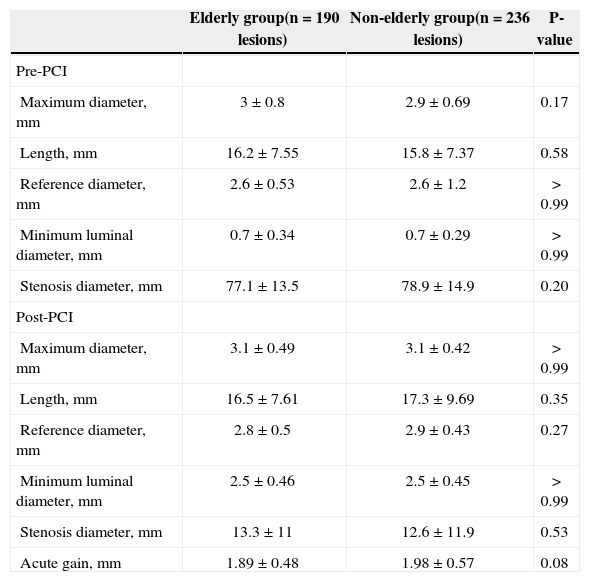
There was no difference in the rates of access-site crossover (4.8% vs. 3.4%; P=0.83), contrast volume (103.1±41.2mL vs. 108.7±42.2mL; P=0.23), fluoroscopy time (15.3±10.3min vs. 16.1±10.3minutes; P=0.45), procedure time (40.6±26 4 minutes vs. 46.4±53.6minutes; P=0.23), and angiographic success (96.3% vs. 97.5%; P=0.99) (Table 3). All stents used were bare-metal stents. Variables obtained in the quantitative coronary angiography are shown in Table 4.
Procedural characteristics
| Elderly group(n=145 procedures/190 lesions) | Non-elderly group(n=176 procedures/236 lesions) | P-value | |
|---|---|---|---|
| Access-site crossover, n (%) | 7 (4.8) | 6 (3.4) | 0.83 |
| Volume contrast, mL | 103.1±41.2 | 108.7±42.2 | 0.23 |
| Fluoroscopy time, min | 15.3±10.3 | 16.1±103 | 0.45 |
| Procedure time, min | 40.6±26.4 | 46.4±53.6 | 0.23 |
| Predilation, n (%) | 84 (44.2) | 120 (50.8) | 0.47 |
| Balloon/artery ratio | 1.12±0.34 | 1.09±0.28 | 0.75 |
| Stent/lesion proportion, mm | 1±0.2 | 1.1±0.3 | 0.22 |
| Maximum pressure, atm | 13.1±1.97 | 134.4±2.07 | 0.87 |
| Angiographic success, n (%) | 183 (96.3) | 230 (97.5) | 0.99 |
Quantitative coronary angiography
| Elderly group(n=190 lesions) | Non-elderly group(n=236 lesions) | P-value | |
|---|---|---|---|
| Pre-PCI | |||
| Maximum diameter, mm | 3±0.8 | 2.9±0.69 | 0.17 |
| Length, mm | 16.2±7.55 | 15.8±7.37 | 0.58 |
| Reference diameter, mm | 2.6±0.53 | 2.6±1.2 | > 0.99 |
| Minimum luminal diameter, mm | 0.7±0.34 | 0.7±0.29 | > 0.99 |
| Stenosis diameter, mm | 77.1±13.5 | 78.9±14.9 | 0.20 |
| Post-PCI | |||
| Maximum diameter, mm | 3.1±0.49 | 3.1±0.42 | > 0.99 |
| Length, mm | 16.5±7.61 | 17.3±9.69 | 0.35 |
| Reference diameter, mm | 2.8±0.5 | 2.9±0.43 | 0.27 |
| Minimum luminal diameter, mm | 2.5±0.46 | 2.5±0.45 | > 0.99 |
| Stenosis diameter, mm | 13.3±11 | 12.6±11.9 | 0.53 |
| Acute gain, mm | 1.89±0.48 | 1.98±0.57 | 0.08 |
PCI, percutaneous coronary intervention.
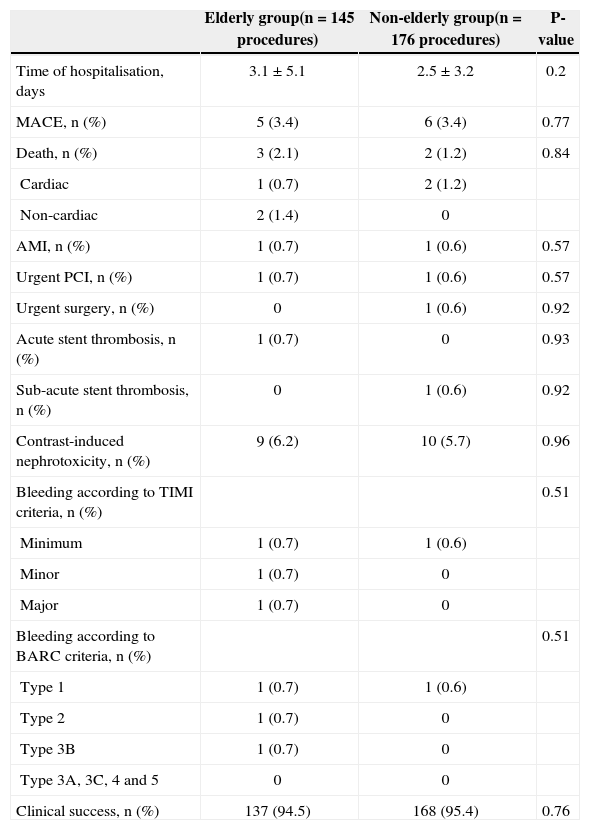
When analysing the in-hospital outcome (Table 5), there was one case of acute stent thrombosis in the elderly group (0.7%) and one case of sub-acute thrombosis in the non-elderly group (0.6%), with myocardial infarction without ST-segment elevation (NSTEMI) and consequent urgent percutaneous reintervention in each group. There was one case of emergency surgery in the non-elderly group, corresponding to a patient with acute myocardial infarction with ST-segment elevation (STEMI) in the inferior wall, with a ten-hour interval between symptom onset and the seeking of care. Although primary PCI was performed in the right coronary artery with angiographic success, the patient had ventricular septal rupture and, despite the surgery, eventually died. Regarding other deaths, there were three deaths in the elderly group: one cardiac death, one due to septic shock from pneumonia associated with mechanical ventilation, and another from sepsis in a patient with peripheral artery disease (diabetic foot), all in the post-STEMI phase. In the non-elderly group, there was another death, in addition to the previously reported, from cardiogenic shock in the evolution phase of STEMI. There was only one case of severe bleeding in the elderly group (major and type 3B by TIMI and BARC criteria, respectively), which occurred in one of the patients who had access-site crossover to the femoral artery, requiring vascular surgery.
In-hospital clinical events
| Elderly group(n=145 procedures) | Non-elderly group(n=176 procedures) | P-value | |
|---|---|---|---|
| Time of hospitalisation, days | 3.1±5.1 | 2.5±3.2 | 0.2 |
| MACE, n (%) | 5 (3.4) | 6 (3.4) | 0.77 |
| Death, n (%) | 3 (2.1) | 2 (1.2) | 0.84 |
| Cardiac | 1 (0.7) | 2 (1.2) | |
| Non-cardiac | 2 (1.4) | 0 | |
| AMI, n (%) | 1 (0.7) | 1 (0.6) | 0.57 |
| Urgent PCI, n (%) | 1 (0.7) | 1 (0.6) | 0.57 |
| Urgent surgery, n (%) | 0 | 1 (0.6) | 0.92 |
| Acute stent thrombosis, n (%) | 1 (0.7) | 0 | 0.93 |
| Sub-acute stent thrombosis, n (%) | 0 | 1 (0.6) | 0.92 |
| Contrast-induced nephrotoxicity, n (%) | 9 (6.2) | 10 (5.7) | 0.96 |
| Bleeding according to TIMI criteria, n (%) | 0.51 | ||
| Minimum | 1 (0.7) | 1 (0.6) | |
| Minor | 1 (0.7) | 0 | |
| Major | 1 (0.7) | 0 | |
| Bleeding according to BARC criteria, n (%) | 0.51 | ||
| Type 1 | 1 (0.7) | 1 (0.6) | |
| Type 2 | 1 (0.7) | 0 | |
| Type 3B | 1 (0.7) | 0 | |
| Type 3A, 3C, 4 and 5 | 0 | 0 | |
| Clinical success, n (%) | 137 (94.5) | 168 (95.4) | 0.76 |
MACE, major adverse cardiac events; AMI, acute myocardial infarction; PCI, percutaneous coronary intervention; TIMI, Thrombolysis in Myocardial Infarction; BARC, Bleeding Academic Research Consortium.
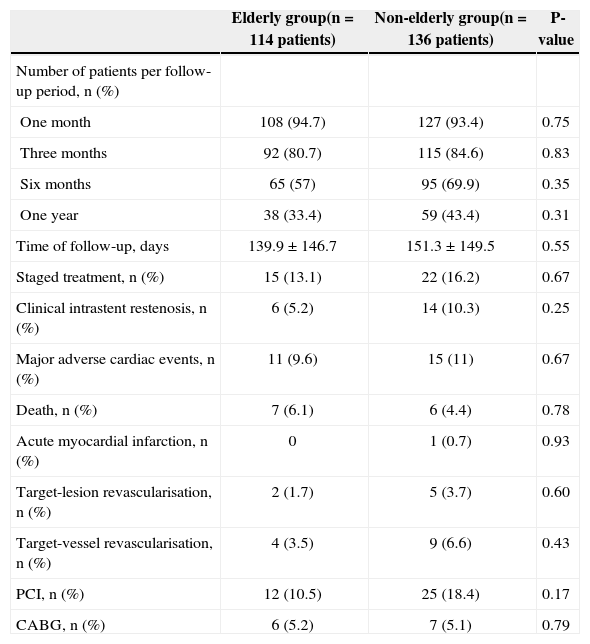
At the late follow-up (139.9±146.7days vs. 151.3±149.5days; P=0.55), there was no difference in the rate of major adverse cardiac events (9.6% vs. 11%; P=0.67), death (6.1% vs. 4.4%; P=0.78), myocardial infarction (0 vs. 0.7%; P=0.93), target-vessel revascularization (3.5% vs. 6.6%; P=0.43), or target-lesion revascularization (1.7% vs. 3.7%; P=0.60) (Table 6). There were no late or very late stent thromboses in this period.
Late clinical events
| Elderly group(n=114 patients) | Non-elderly group(n=136 patients) | P-value | |
|---|---|---|---|
| Number of patients per follow-up period, n (%) | |||
| One month | 108 (94.7) | 127 (93.4) | 0.75 |
| Three months | 92 (80.7) | 115 (84.6) | 0.83 |
| Six months | 65 (57) | 95 (69.9) | 0.35 |
| One year | 38 (33.4) | 59 (43.4) | 0.31 |
| Time of follow-up, days | 139.9±146.7 | 151.3±149.5 | 0.55 |
| Staged treatment, n (%) | 15 (13.1) | 22 (16.2) | 0.67 |
| Clinical intrastent restenosis, n (%) | 6 (5.2) | 14 (10.3) | 0.25 |
| Major adverse cardiac events, n (%) | 11 (9.6) | 15 (11) | 0.67 |
| Death, n (%) | 7 (6.1) | 6 (4.4) | 0.78 |
| Acute myocardial infarction, n (%) | 0 | 1 (0.7) | 0.93 |
| Target-lesion revascularisation, n (%) | 2 (1.7) | 5 (3.7) | 0.60 |
| Target-vessel revascularisation, n (%) | 4 (3.5) | 9 (6.6) | 0.43 |
| PCI, n (%) | 12 (10.5) | 25 (18.4) | 0.17 |
| CABG, n (%) | 6 (5.2) | 7 (5.1) | 0.79 |
PCI, percutaneous coronary intervention; CABG, coronary artery bypass grafting.
In the authors’ experience, PCI through radial access has shown to be as effective in elderly patients as in younger patients, with high technical success rate, low rate of crossover, and very good safety, as puncture site bleeding and complications very rarely occurred in the assessed sample. Transradial PCI can be safely performed in elderly patients.
In the present sample, chronic renal failure was more common in the elderly, as was multivessel disease. The fluoroscopy and procedure time, as well as rates of vascular complications, cardiac death, and procedural success did not differ between groups in the present study. These results are consistent with those reported by Cao et al.10
In the study by Andrade et al.,11 despite the mean age of 70 years and the prevalence of procedures in the presence of acute coronary syndrome, including 22% primary PCI, a high success rate and low prevalence of angiographic complications were attained, requiring access-site crossover in less than 3% of cases, with no need for excess time for its performance or increased use of materials.
Studies have demonstrated that PCI through femoral access in elderly patients has a higher incidence of vascular complications when compared to younger patients.12-14 In the “Prevention of Ischemic Complications (EPIC)” study,15 older age was an independent risk factor for vascular complications and bleeding related to the puncture site after femoral approach. Although the use of arterial closure devices may reduce the incidence of problems after the femoral approach, elderly patients still have a higher rate of vascular complications.16,17
Although older patients have more radial artery tortuosity in the brachiocephalic trunk and subclavian artery, this had no impact on the procedural success rate. These findings suggest that technical failure due to anatomical characteristics is rare and non-significant in transradial procedures in the elderly.
Study limitationsThe present study has the inherent limitations of retrospective and observational studies. An important limitation is its performance in a single center with a relatively small number of patients, in whom the radial access is predominant for both diagnostic and therapeutic coronary procedures.
CONCLUSIONSDespite the greater clinical and angiographic complexity, PCI through the radial access is safe and effective, with a high procedural success rate and low in-hospital and late follow-up complication rates.
CONFLICT OF INTERESTThe authors declare no conflicts of interest.
The authors would like to thank Ettóre Campo Dall’Orto for his invaluable help in designing, handling, and maintaining this study’s database.