


Hepatopulmonary syndrome (HPS) is a serious, progressive disease. Its pathophysiology resides in a hypoxic intrapulmonary shunt and severe clinical deterioration. Liver transplantation (LT) is the only effective treatment in appropriately selected patients.
ObjectiveTo acknowledge the importance of early diagnosis of HPS.
Patients and methodsObservational, descriptive, retrospective trial including 8 patients with HPS that received LT between April 2006 and August 2014. The clinical data prior to transplantation and follow-up after the procedure were reviewed.
A multivariate analysis (stepwise forward logistic regression analysis) was used to identify the variable that could potentially increase the risk of death.
ResultsOf the 8 patients, death could only be significantly predicted based on the pre-LT arterial blood partial oxygen pressure (PaO2) (p=0.002).
The average pre-LT PaO2 of the patients that died was 51.5±2.49 SD, with a statistically significant difference (p=0.002).
None of the variables was statistically significant for HPS reversibility.
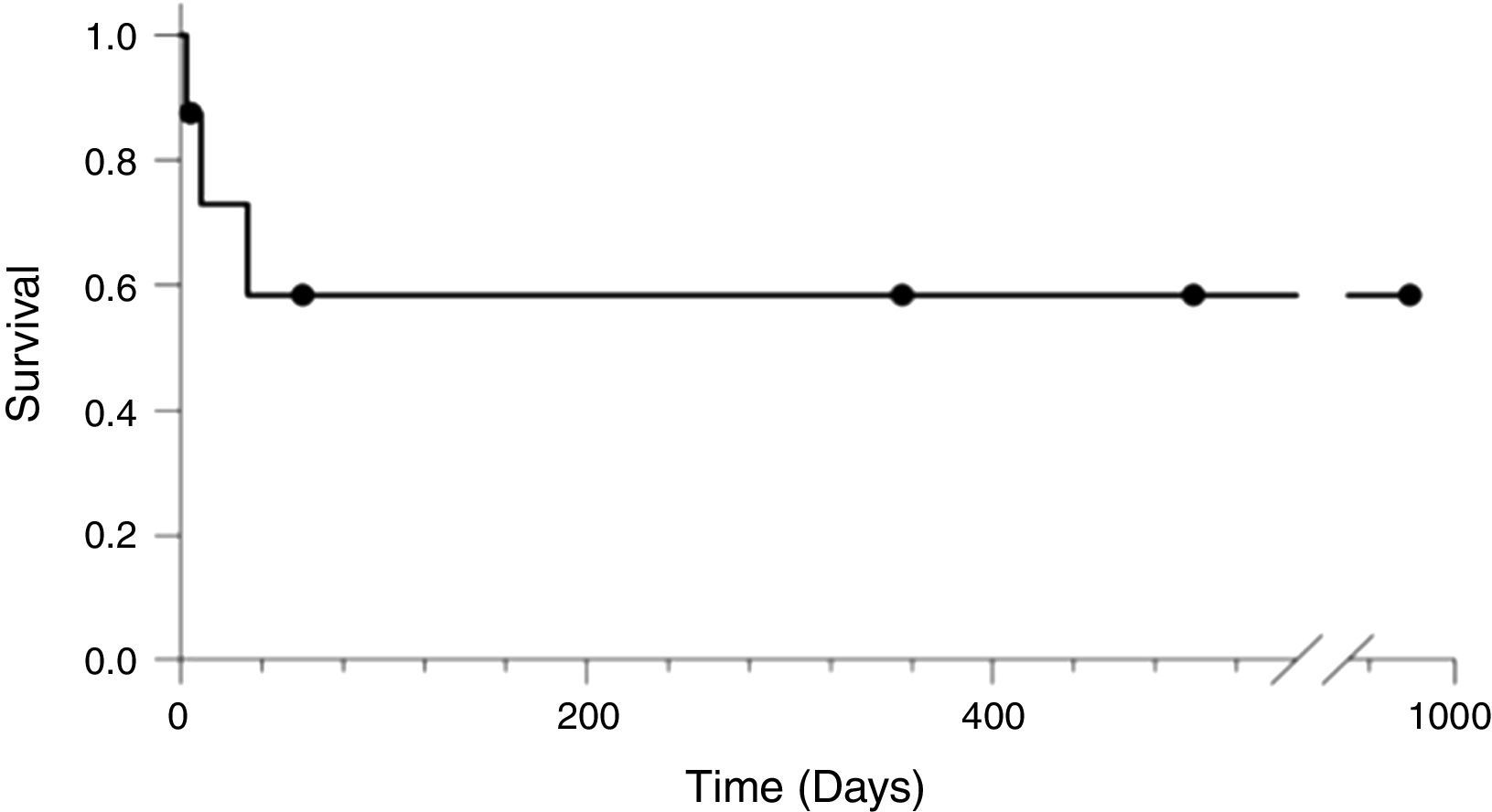
The survival rate of patients diagnosed with HPS following the LT was 62.5%.
ConclusionsThe level of pre-LT hypoxemia is an important predictor for immediate postoperative mortality. Early detection of the condition is critical to reduce the post LT morbidity and mortality so that the indication for transplant is made at the right time, regardless of the stage of liver disease. The most efficient clinical strategy could be the use of appropriate early detection protocols for HPS through screening of hypoxemia in patients with portal hypertension.
El síndrome hepatopulmonar (SHP) es una enfermedad grave y progresiva cuya fisiopatología reside en un shunt intrapulmonar con hipoxia y deterioro clínico severo. Como único tratamiento efectivo se ha postulado el trasplante hepático (TH), en pacientes adecuadamente seleccionados.
ObjetivoReconocer la importancia del diagnostico temprano del SHP.
Pacientes y métodosMediante un estudio observacional, descriptivo, con carácter retrospectivo de 8 pacientes con SHP, a los que se les realizó TH en el período entre Abril 2006-Agosto 2014. Se han revisado los datos clínicos previos al trasplante y el seguimiento tras este.
Se empleó un estudio multivariante (stepwise forward logistic regression analisis), para determinar cual variable podría incrementar el riesgo de muerte.
ResultadosDe los 8 pacientes, el resultado de muerte sólo pudo ser predicho significativamente por el factor presión parcial de oxígeno en sangre arterial (PaO2) pre-TH (p=0,002).
La PaO2 pre-TH promedio de los pacientes que fallecieron era de 51,5 +/- 2,49 DS, siendo la diferencia estadísticamente significativa (p=0,002).
Ninguna variable resultó estadísticamente significativa para reversibilidad del SHP.
La supervivencia de los pacientes con criterio de SHP posterior al TH fue de 62,5%.
ConclusionesEl grado de hipoxemia pre-TH es un factor predictor importante de mortalidad en el postoperatorio inmediato. La precocidad en la detección de la entidad es fundamental tanto para disminuir la morbimortalidad post TH como para indicar éste en el momento óptimo independientemente del estadío de la enfermedad hepática. Protocolos adecuados de detección precoz del SHP mediante screening de hipoxemias en pacientes con hipertensión portal, puede ser la estrategia clínica más eficiente.
The first publication evidencing the association between liver and pulmonary disorders was in 1884 by Fluckieger; however, it was not until 1977 that Kennedy and Knudson coined the term hepatopulmonary syndrome (HPS).1 It was initially thought that this was a reversible condition and hence LT was contraindicated. The observation that HPS could be resolved after LT and that this was the only effective treatment to revert the condition was only made early in the 90s.
HPS is a low prevalence condition but with high morbidity and morality that may severely compromise the functional status of patients with advanced liver disease and/or portal hypertension.2 HPS results from impaired liver clearance of various vascular mediators leading to an imbalance between vasodilators and vasoconstrictors that causes abnormal intrapulmonary vasodilation and intrapulmonary shunt. The resulting disruption in arterial oxygenation not always improves with supplemental O2, with a clinical presentation of platypnea (dyspnea induced by upright posture) and orthodeoxia (>5% desaturation or >4mmHg PaO2 drop when moving from decubitus to an upright posture). These PaO2 alterations are mainly the result of a ventilation/perfusion imbalance, with pulmonary shunt in addition to an impaired oxygen diffusion capacity due to the increased capillary diameter and reduced transit time of the erythrocytes through the capillaries as a consequence of the elevated cardiac output characteristic of HPS.3
The echocardiographic finding of an extracardiac and intrapulmonary shunt confirms the diagnosis.4 To differentiate whether the shunt is intra or extra cardiac the observation of whether the passage of microbubbles following an intravenous injection o cold stirred serum from both right and left cavities is early (<3 cardiac cycles), which will indicate intracardiac shunting, or late (>3 cardiac cycles) which will be diagnostic for intrapulmonary shunting. The diagnostic criteria for HPS are: “Partial oxygen pressure<80mmHg or oxygen alveolar–arterial gradient≥15mmHg while breathing room air, positive findings in the contrast, portal hypertension (more common) with or without cirrhosis. With an alveolar–arterial oxygen gradient≥15mmHg the severity grade depends on the partial oxygen pressure, where mild severity is PO2>80mmHg, moderate severity is PO2>60 to <80mmHg, severe is PO2>50 to <60mmHg and extremly severe is PO2<50mmHg”.5
Up until now, the only effective treatment is liver transplantation in properly selected cases and when the procedure is indicated at a particular time moment of the pulmonary disease.6
Patients and methodsWe have completed an observational descriptive trial with retrospective data collection from patients who received a LT between April 2006 and August 2014. From a total of 815 transplants performed during that period, there were 8 patients (1%) diagnosed with HPS, 7 of which were males (87.5%) and 1 (12.5%) was a female. The age range was 32–60 years at the time of the LT. All patients had been diagnosed with HPS through pulmonary scan or echocardiography. Additionally, the patients presented with altered oxygenation in the arterial gases. The trial was approved by the institutional ethics committee under code 2016/0125.
The clinical data collected included age, gender, MELD and Child–Pugh, etiology of the liver pathology, last gasometry immediately before transplantation, preoperative home oxygen requirements, postoperative mechanical ventilation (MV) time, length of stay in resuscitation and causes of death.
For the qualitative variable distribution, the absolute frequencies of each category were used and Fisher's test was administered. The dependent variable was survival and the independent variables were: pre-LT home O2 requirements, signs of reperfusion syndrome during LT, post-extubation non-invasive mechanical ventilation (NIMV) requirements, and whether the patient has a long postoperative resuscitation unit stay with 48h being the estimated normal length of stay.
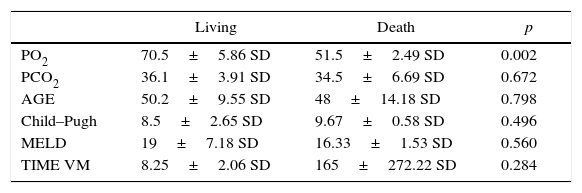
The statistical analysis of quantitative variables used the mean and standard deviation of living and death patients (Table 1). Likewise, a multivariable study–stepwise forward logistic regression analysis–was performed to determine which variable could significantly predict the risk of death. The statistical significance value was set at 0.05.
Demographic and clinical characteristics and hepatic functional status.
| Living | Death | p | |
|---|---|---|---|
| PO2 | 70.5±5.86 SD | 51.5±2.49 SD | 0.002 |
| PCO2 | 36.1±3.91 SD | 34.5±6.69 SD | 0.672 |
| AGE | 50.2±9.55 SD | 48±14.18 SD | 0.798 |
| Child–Pugh | 8.5±2.65 SD | 9.67±0.58 SD | 0.496 |
| MELD | 19±7.18 SD | 16.33±1.53 SD | 0.560 |
| TIME VM | 8.25±2.06 SD | 165±272.22 SD | 0.284 |
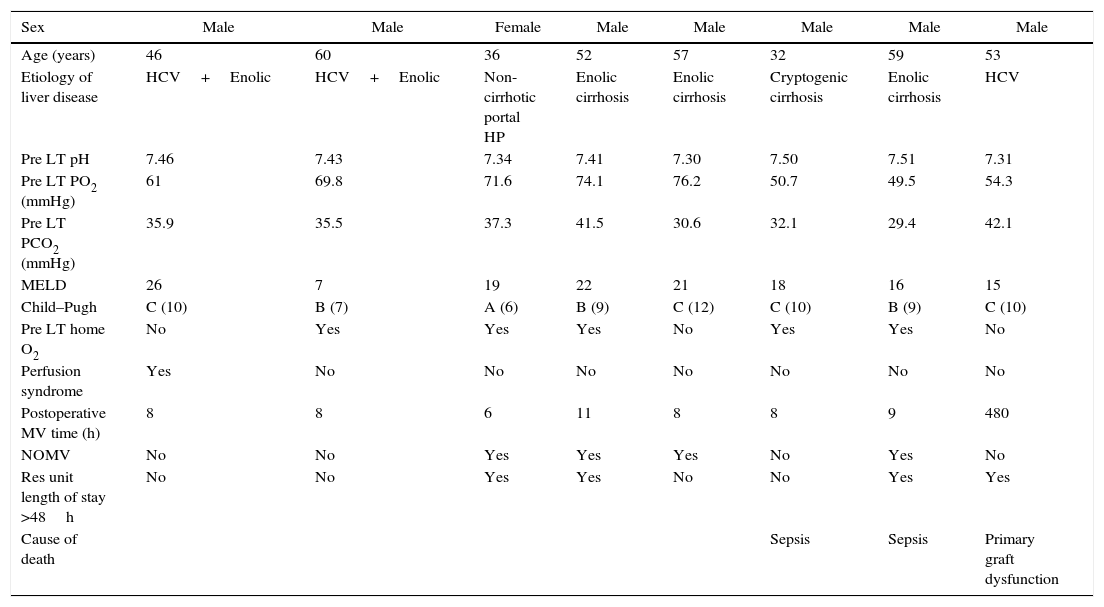
The baseline characteristics of the 8 patients transplanted with HPS during the trial period are presented in Table 2 and refer to the typology and the severity of the liver disease, as well as the data used to evaluate the pre and post-operative pulmonary status. The etiology of liver failure was defined as: enolic cirrhosis, hepatitis C virus (HCV), cryptogenic cirrhosis, and 1 case of HPS due to non-cirrhotic portal hypertension of presinusoidal prehepatic origin. The Child–Pugh status distribution of the sample was 1 patient in Stage A, 3 in stage B, and the other 4 in stage C.
Clinical aspects.
| Sex | Male | Male | Female | Male | Male | Male | Male | Male |
|---|---|---|---|---|---|---|---|---|
| Age (years) | 46 | 60 | 36 | 52 | 57 | 32 | 59 | 53 |
| Etiology of liver disease | HCV+Enolic | HCV+Enolic | Non-cirrhotic portal HP | Enolic cirrhosis | Enolic cirrhosis | Cryptogenic cirrhosis | Enolic cirrhosis | HCV |
| Pre LT pH | 7.46 | 7.43 | 7.34 | 7.41 | 7.30 | 7.50 | 7.51 | 7.31 |
| Pre LT PO2 (mmHg) | 61 | 69.8 | 71.6 | 74.1 | 76.2 | 50.7 | 49.5 | 54.3 |
| Pre LT PCO2 (mmHg) | 35.9 | 35.5 | 37.3 | 41.5 | 30.6 | 32.1 | 29.4 | 42.1 |
| MELD | 26 | 7 | 19 | 22 | 21 | 18 | 16 | 15 |
| Child–Pugh | C (10) | B (7) | A (6) | B (9) | C (12) | C (10) | B (9) | C (10) |
| Pre LT home O2 | No | Yes | Yes | Yes | No | Yes | Yes | No |
| Perfusion syndrome | Yes | No | No | No | No | No | No | No |
| Postoperative MV time (h) | 8 | 8 | 6 | 11 | 8 | 8 | 9 | 480 |
| NOMV | No | No | Yes | Yes | Yes | No | Yes | No |
| Res unit length of stay >48h | No | No | Yes | Yes | No | No | Yes | Yes |
| Cause of death | Sepsis | Sepsis | Primary graft dysfunction |
NIMV, non-invasive mechanical ventilation; MV, mechanical ventilation; LT, liver transplant; Res, resuscitation.
All of them had variable levels of altered oxygenation according to the arterial gases.
According to our statistical analysis, the fatality outcome could only have been significantly predicted based on PaO2 (p=0.002). The other variables were not significant predictors of the risk of death: age (p=0.798), PCO2 (p=0.672), Child–Pugh (p=0.496), MELD (p=0.560), and MV time (p=0.284).
The average pre-LT PaO2 of the patients that died was 51.5±2.49 SD, and the average of patients that survived was 70.54±5.86 SD, with a statistically significant difference (p=0.002).
Of the total number of patients studied, 3 (37.5%) died during the postop, between days 3 and 33. The causes of death were: 2 patients died from sepsis and the third one due to multiple organ failure in the context of global respiratory failure. It should be highlighted that the most frequent cause of mortality is the same as in non HPS transplanted patients.
The patients that survived had a follow-up period ranging from 5 to 979 days until the trial was closed (Fig. 1).
. Source: authors.")
Similarly, there was a attempt to establish possibility for the studied variables to predict reversibility of the HPS, considering total reversibility as improvement in hypoxemia (PaO2) and partial reversibility as a reduction in the home O2 requirements. Keeping in mind the same test and the same variables, none of them was statistically significant (p≥0.05); of the 5 patients that were alive, 3 had total HPS reversal, 2 at hospital discharge and 1 6 months after the LT. 2 patients presented a partial HPS reversal with reduced home O2 requirements versus the pre-transplantation requirements.
DiscussionThe LT due to HPS represent 1% of the liver transplants performed in our center during the period described, with an approximate post-LT survival of 62.5%, as compared to the series in other transplant centers that report a variable prevalence of 4–30%.7 This reflects on the one hand a potential over-diagnosis of the institution in certain series, and on the other an underestimation in our own series. The reason is the difficulty to identify the condition until advanced stages of the disease when dyspnea is already present and the overall condition of the patients, particularly the respiratory status, could have excluded them from being candidates for transplantation. It seems that during the study period some cases where LT could have been the first line treatment would have been excluded in our center because they were missed. This leads us to reflect on the need to do routine pulmonary screening beyond the functional respiratory tests (FRT) that are normal in many patients with HPS.8,9
Liver transplantation controls HPS by correcting the intrapulmonary shunt and improving arterial circulation. Consequently, LT should be a priority in this patients in the light of the significant survival in properly selected cases that are identified at a stage in which the LT is still feasible, with a postoperative morbidity similar to non-HPS LTs, with the sale level of pre-LT liver disease.10 According to the current information, the worsening of hypoxemia is progressive and refractory to medical treatment.11 Several trials have shown a mortality increase in patients with HPS-associated cirrhosis and consequently, LT is suggested as the only effective treatment for this rare but lethal condition.12
Neither the etiology nor the severity of the liver disease affects the development of the syndrome. This contributes to the hypothesis of a genetic predisposition as the cause of HPS in patients with liver disease. However, a significant association with portal hypertension has been identified, as is the case in Budd–Chiari syndrome or in liver fibrosis.13,14 Consequently, maybe the way to approach a HPS screening program could be in patients diagnosed with portal hypertension with cirrhosis and/or syndromes associated with the occurrence of cirrhosis, despite a normal liver function, but that additionally present with non-specific respiratory problems such as dyspnea, that could represent a warning sign for some level of clinical suspicion. In this setting, the accuracy and usefulness of pulse oximetry becomes relevant. Numerous studies have shown that an O2 peripheral saturation (SpO2) equal to or less than 94% identifies any subject with a PaO2≤60mmHg.15 This cost-effectiveness analyses conclude that it is a simple and low-cost technique, in addition to being non-invasive, precise, reliable and applicable at the time of the hepatology visit for regular follow-up.16 It should be noted however, that after the initial screening, the dyspnea and/or hypoxia of the patients identified could be the result of cardiac causes of usual pulmonary diseases that coexist in up to one third of liver disease patients,17 more specific tests such as contrast echocardiography, pulmonary angiography, and comprehensive pulmonary function tests shall be indicated.
The fact that pre-LT PaO2 is suggested as a significant post-LT predictor of mortality, and is considered to be the primary tool for decision-making regarding the timeliness for LT, it becomes necessary to establish a range of PO2 for which LT should be prioritized to optimize the success of therapy. Other groups with large series of LTs with HPS set PO2 levels between 50–60mmHg as the appropriate range for LT indication. In general, patients with PaO2 values under 50mmHg are excluded from the procedure and a PO2<30mmHg is considered by some groups as contraindicated for the procedure.18 However, here are some cases with successful post LT outcomes with a higher survival than non-transplanted cases within the same gasometry range with pre-LT PaO2 below 50mmHg. This means that some cases of HPS with severe hypoxemia shall be comprehensively evaluated and the liver transplant shall be indicated regardless of the severity of hypoxemia.19
The finding that PO2 is the only predictor of mortality may be explained on the basis the pulmonary shunt present if HPS individuals, due to the disrupted oxygen diffusion capacity as a consequence of capillary vasodilation, in addition to a shortened erythrocyte transit time through the capillaries and an elevated cardiac output. This alteration tends to be relatively permanent if not corrected promptly. Therefore, patients with a not excessively low PO2 are excellent candidates for priority liver transplant; on the contrary, patients with low PO2 have a poor prognosis and poor ventilator response, even before transplantation.
The rest of our study variables do not significantly predict the risk of death or reversibility, meaning that they cannot be related since probably these results are limited by the size of the sample. It will be necessary to work on larger samples to assess those variables.
Moreover, keep in mind that in terms of the level of liver disease, MELD is not prognostic in liver cancer-associated HPS patients, neither in metabolic diseases, portal hypertension syndromes, and any other clinical condition not directly associated to the extent of cirrhosis. In this cases, the prioritization for LT indication shall be done based on progression of the disease and patients should be closely monitored for a level of hypoxemia that may question the indication of liver transplantation on account of the high postoperative morbidity and mortality.20
It should be highlighted however that in terms of the patients that died during the immediate postoperative period, the primary cause of death was unrelated to respiratory failure but rather is mostly associated with primary graft dysfunction, biliary complications, perioperative bleeding, sepsis, and other usual morbimortality causes in non-HPS LT, as demonstrated by the Toronto group paper in 2010, involving a large series of cases in two transplantation centers for 6 years.21
All patients that survived the LT had improved arterial oxygenation, although the systematic literature reviews of large series of cases show more variable results in terms of the reversibility of post LT hypoxemia.22 Notwithstanding the fact there was some level of persistent hypoxemia in 2 patients, the condition improved gradually in the course of further control visits, with reduced home O2 requirements (partial HPS reversibility). This ratifies the significance of liver dysfunction in the HPS pathogenesis.
In conclusion, according to our series, despite the low prevalence of HPS among the patients who are candidates for LT, a considerable morbimortality exists with the current medical treatment modalities.23 PO2 has been identified as a statistically significant predictor of postoperative mortality and must be taken into consideration when prioritizing patients in the waiting list for LT. PO2 should be the key tool for screening programs to identify concomitant and potentially reversible lung disease. Although the other variables studied fail to significantly predict the risk of death or reversibility, additional studies with larger samples are needed.
Conflict of interestThe authors have no conflicts of interest to declare.
FundingThe authors did not receive sponsorship to carry out this article.
Please cite this article as: Orozco-Delgado M, López-Cantero M, Zampella V, Vicente R, Galán J. Factores predictores de mortalidad y estrategias de detección precoz de sindrome hepatopulmonar en pacientes trasplantados hepáticos. Rev Colomb Anestesiol. 2016;44:311–316.