



The purpose of this study is to analyse the publication rate of studies presented as podium presentations in the Spanish Society of Shoulder and Elbow Surgery (SECHC) congresses.
MethodsOne hundred and twenty-two abstracts presented at the SECHC congresses held in 2007, 2009 and 2011 were included for the purpose of the study. The oral communications were categorised by study type, sample included and follow-up. In June 2017, possible publications of these studies were searched in PubMed. Type of study, delay in publication, journal and impact factor obtained were recorded. The concordance between the information presented at the congress and their subsequent full-text publications was analysed.
ResultsThe publication rate was 17.21% (21 of the 122 abstracts studied) after 6 years, with a mean time spent for publications of 36.71 months, and a mean impact factor of 1.51. There were no differences between results initially presented at the congresses and those subsequently published (p>0.05).
DiscussionThe majority of papers presented at SECHC congresses do not end up with a publication. The papers that are published do not usually contain significant differences compared to the content delivered at the congress.
El propósito de este estudio es analizar la tasa de publicación de los estudios presentados como comunicaciones orales en los congresos de la Sociedad Española de Cirugía de Hombro y Codo (SECHC).
MétodosSe incluyeron 122 resúmenes presentados en los congresos SECHC celebrados en 2007, 2009 y 2011. Se categorizaron las comunicaciones orales por tipo de estudio, muestra incluida y seguimiento. En junio de 2017 se buscaron posibles publicaciones de estos trabajos en PubMed. El tiempo para la publicación, revista y factor de impacto fueron registrados. Se analizó la concordancia entre la información presentada en el congreso y las publicaciones posteriores.
ResultadosVeintiuno de los 122 resúmenes analizados (17,21%) fueron publicados después de 6 años de seguimiento mínimo, con un tiempo medio empleado para las publicaciones de 36,71 meses y con un factor de impacto medio de 1,51. No se observaron diferencias significativas entre los datos expuestos inicialmente en el congreso y los posteriormente publicados (p>0,05).
ConclusionesLa mayoría de los trabajos presentados en congresos SECHC no acaban siendo publicados. Aquellos trabajos que logran publicarse no suelen presentar diferencias significativas respecto a lo que se expuso previamente en el congreso.
Presenting an investigative work as a scientific communication at a congress does not necessarily lead to its subsequent publication, since the process of publication requires effort and involvement by the authors. Lack of time on the authors’ part for preparing the article appears to be the principal barrier to publishing a scientific communication in a journal.1 Despite this, publication in indexed journals is still essentially the standard method of spreading information through the scientific community, since it leads to greater dissemination of the work undertaken and recognition for the authors.
The rate of publications of oral communications in specialised journals and the factor of impact obtained are a reflection of the scientific quality of congresses.2 For this reason, some Spanish medical associations have published their publication rates, with highly variable results.3–8 These publications rates range from between 17% and 51% for podium presentations and from between 20% and 50% for those studies which include scientific posters and podium presentations in their analysis. In recent years there has been an increasingly greater presence of Spanish authors, in international reference data bases, which has been calculated as a 600% rise between 1980 and 2003.9
Bibliometric information on congresses in the speciality or sub-specialty of orthopaedic surgery or traumatology celebrated in the Spanish language is unknown. Different international orthopaedic and trauma associations have published publication rates of their congress,10–32 because interest in the rate of publications has increased. The publication rate varied from between 48% and 73%n depending on the congress analysed and the year of its celebration. With regard to the sub-speciality of shoulder and elbow, only the publication rate of the shoulder and elbow sessions of the specialty congress of the American Academy of Orthopaedic Surgery (AAOS)12 is known, and is set at 58%. In this article, the changes in the order and number of authors, in the study sample or in the title do not usually have an impact on the conclusions of publication.
What is the probability of publication of an abstract that has been accepted in the congress of the Spanish Society of Shoulder and Elbow Surgery (SECHC)? Is any factor influential in the publication rate? Our study proposes to offer the publication rate of the congress of the SECHC, analysing the factors which could affect whether a research study is published afterwards. Concordance of content between published studies and their corresponding podium presentations previously presented in the congress was also analysed.
Material and methodsThe abstracts of the oral communications presented in 3 consecutive congresses of the SECHC in 2007, 2009 and 2011 were obtained through the society's website (www.sechc.es) and included in this study. Communications were classified in accordance with the type of study (treatment, diagnosis, prognosis or basic sciences) and the level of scientific study (I–V). The studies were classified according to subject matter: elbow injuries, proximal humerus fractures, rotator cuff injury, degenerative disease of the shoulder/joint replacements, glenohumerus instability, collarbone injury/acromioclavicular articulation, basic or miscellaneous sciences.
A minimum period of 6 years was fixed to evaluate the survival of the review processes and publication of the articles, although the majority of communications which are published manage to be published within 4 years after the celebration of the congress.11,14,16,17,23,32
All the abstracts obtained through the SECHC web site were investigated using the PubMed data in the month of June 2017, which aimed at identifying those abstracts which were published afterwards. The search was undertaken with the name of the main author, and the key words that appeared in the title of the abstract. In the cases where no publications were found with the before-mentioned criteria, a search was made through the remaining authors prior to declaring a work as not published. The criteria used to declare a abstract as published was based on previously described criteria.3,27
A total of 122 oral presentation abstracts were included in the SECHC website and were classified according to a combination of characteristics in order to determine the probabilities of obtaining publication in indexed journals. The indexed journal where the works were published and the impacting factor at the time of publication were recorded for those abstracts which passed the review process of the indexed journal, using CiteFactor.33
In statistical analysis, the Wilcoxon rank-sum non parametric test was used for comparing groups, and the Spearman correlation test for assessing associations of continuous variables which followed a non-normal distribution. The chi-square test or the exact Fisher test was used to assess the association between dichotomous variables. 95% confidence intervals were calculated over the estimators. The R version 3.4.0 for Windows was the statistical package used to treat data and for analysis.
ResultsOut of a total of 122 abstracts examined, 28 corresponded to elbow injury, 27 to proximal humerus fractures, 24 to rotator cuff injury, 19 to basic sciences or miscellaneous, 13 to glenohumeral instability, 7 to degenerative disease of the shoulder and 4 to collarbone or acromioclavicular injury. During the congress celebrated in 2007 30 oral communications were presented, 43 in the 2009 congress, and 49 in the 2011 congress.
With regard to the type of works presented at the SECHC congress, 87 abstracts corresponded to treatment assessment presentations (intervention); 15 to assessment of prognostic factors; 11 to assessment of diagnostic methods; 8 to basic sciences, whilst only one presentation consisted of a review of the literature. With regard to the level of scientific evidence, we found one presentation of level I, 9 of level II, 17 of level III, 85 of level IV, 2 of level V,whilst it was not possible to classify 8 by level of evidence. The mean sample of communications presented was of 59.66 patients per presentation (4–912), with mean follow-up of 27.06 (1–240) months.
Twenty one of the 122 oral communications assessed by the SECHC (17.21%) presented in the congresses were published in indexed journals, in accordance with the applied criteria.34–54 The 21 articles were published in 12 difference journals, with a mean impact factor of 1.51 (0.09–3.29). The mean time which elapsed between the presentation of the oral communication and subsequent publication was 36.71 months (4–92 months). 4 communications out of 30 oral communications (13.6%) were published in reference to the 2007 congress, 6 out of 43 communications (13.95%) in reference to the 2009 congress, whilst of the 49 communications presented in 2011, 11 of them successfully had a publication in an indexed journal (22.45%). The tendency to growing publication between congresses did not obtain any statistical significance (p=0.29).
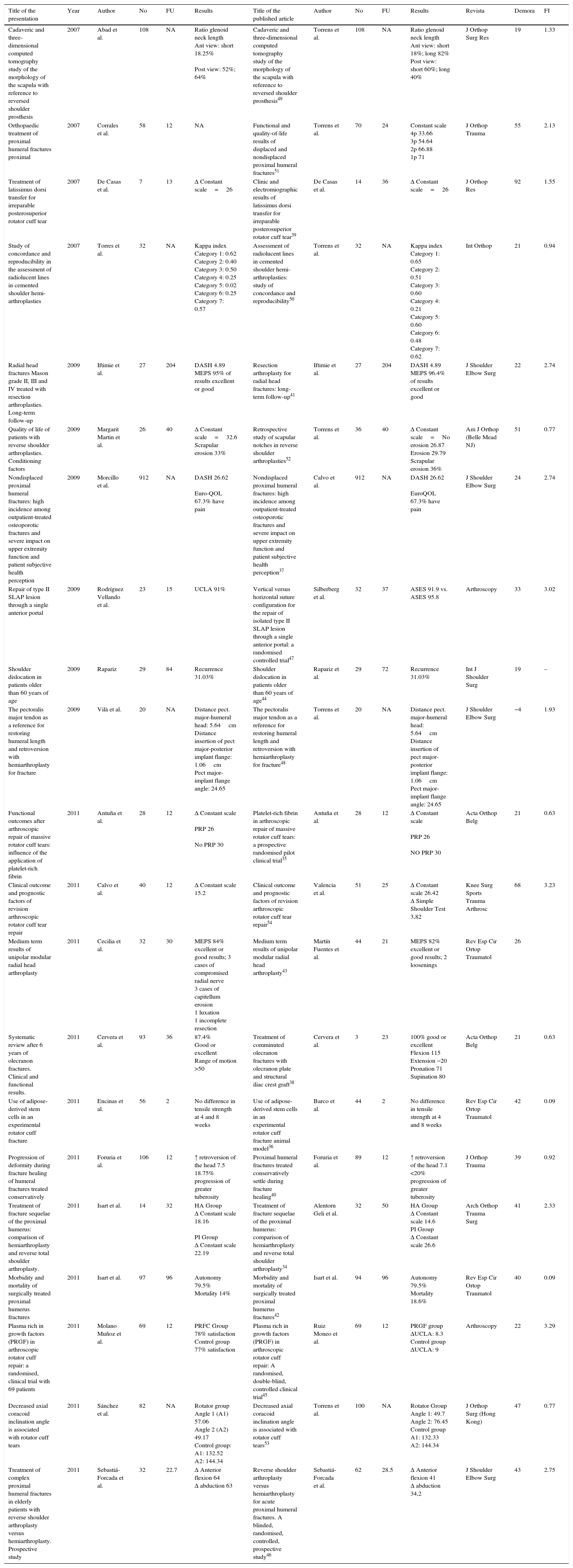
Fifteen of the 21 articles published showed differences in the sample size (4 of the 15 reported lower samples, whilst higher samples were reported in 11 of the 15 samples included in the final presentation). With regards to follow-up, 3 of the 21 studies published lower follow-ups whilst 4 of the published presentations reported a higher follow-up than that presented at the SECHC congress. Nine of the 21 studies reported the same follow-up whilst 5 did not apply follow-up due to the study design. In 8 out of the 21 works published the results were the same as those previously expressed in the SECHC congress, whilst in 12 works the results were different. In one single work they could not obtain results from the oral communication in the SECHC (Table 1) website. Despite this, only one out of the 21 works published modified the conclusions. In this study,47 the focus of the published work differed from the podium presentation. The changes in the sample, follow-up and results were not statistically significant (p=0.26; p=0.17 and p=0.36, respectively).
Comparison of podium presentations with articles published afterwards, for those presentations which obtained indexed publications.
| Title of the presentation | Year | Author | No | FU | Results | Title of the published article | Author | No | FU | Results | Revista | Demora | FI |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cadaveric and three-dimensional computed tomography study of the morphology of the scapula with reference to reversed shoulder prosthesis | 2007 | Abad et al. | 108 | NA | Ratio glenoid neck length Ant view: short 18.25% Post view: 52%; 64% | Cadaveric and three-dimensional computed tomography study of the morphology of the scapula with reference to reversed shoulder prosthesis49 | Torrens et al. | 108 | NA | Ratio glenoid neck length Ant view: short 18%; long 82% Post view: short 60%; long 40% | J Orthop Surg Res | 19 | 1.33 |
| Orthopaedic treatment of proximal humeral fractures proximal | 2007 | Corrales et al. | 58 | 12 | NA | Functional and quality-of-life results of displaced and nondisplaced proximal humeral fractures51 | Torrens et al. | 70 | 24 | Constant scale 4p 33.66 3p 54.64 2p 66.88 1p 71 | J Orthop Trauma | 55 | 2.13 |
| Treatment of latissimus dorsi transfer for irreparable posterosuperior rotator cuff tear | 2007 | De Casas et al. | 7 | 13 | Δ Constant scale=26 | Clinic and electromiographic results of latissimus dorsi transfer for irreparable posterosuperior rotator cuff tear39 | De Casas et al. | 14 | 36 | Δ Constant scale=26 | J Orthop Res | 92 | 1.55 |
| Study of concordance and reproducibility in the assessment of radiolucent lines in cemented shoulder hemi-arthroplasties | 2007 | Torres et al. | 32 | NA | Kappa index Category 1: 0.62 Category 2: 0.40 Category 3: 0.50 Category 4: 0.25 Category 5: 0.02 Category 6: 0.25 Category 7: 0.57 | Assessment of radiolucent lines in cemented shoulder hemi-arthroplasties: study of concordance and reproducibility50 | Torrens et al. | 32 | NA | Kappa index Category 1: 0.65 Category 2: 0.51 Category 3: 0.60 Category 4: 0.21 Category 5: 0.60 Category 6: 0.48 Category 7: 0.62 | Int Orthop | 21 | 0.94 |
| Radial head fractures Mason grade II, III and IV treated with resection arthroplasties. Long-term follow-up | 2009 | Iftimie et al. | 27 | 204 | DASH 4.89 MEPS 95% of results excellent or good | Resection arthroplasty for radial head fractures: long-term follow-up41 | Iftimie et al. | 27 | 204 | DASH 4.89 MEPS 96.4% of results excellent or good | J Shoulder Elbow Surg | 22 | 2.74 |
| Quality of life of patients with reverse shoulder arthroplasties. Conditioning factors | 2009 | Margarit Martin et al. | 26 | 40 | Δ Constant scale=32.6 Scrapular erosion 33% | Retrospective study of scapular notches in reverse shoulder arthroplasties52 | Torrens et al. | 36 | 40 | Δ Constant scale=No erosion 26.87 Erosion 29.79 Scrapular erosion 36% | Am J Orthop (Belle Mead NJ) | 51 | 0.77 |
| Nondisplaced proximal humeral fractures: high incidence among outpatient-treated osteoporotic fractures and severe impact on upper extremity function and patient subjective health perception | 2009 | Morcillo et al. | 912 | NA | DASH 26.62 Euro-QOL 67.3% have pain | Nondisplaced proximal humeral fractures: high incidence among outpatient-treated osteoporotic fractures and severe impact on upper extremity function and patient subjective health perception37 | Calvo et al. | 912 | NA | DASH 26.62 EuroQOL 67.3% have pain | J Shoulder Elbow Surg | 24 | 2.74 |
| Repair of type II SLAP lesion through a single anterior portal | 2009 | Rodríguez Vellando et al. | 23 | 15 | UCLA 91% | Vertical versus horizontal suture configuration for the repair of isolated type II SLAP lesion through a single anterior portal: a randomised controlled trial47 | Silberberg et al. | 32 | 37 | ASES 91.9 vs. ASES 95.8 | Arthroscopy | 33 | 3.02 |
| Shoulder dislocation in patients older than 60 years of age | 2009 | Rapariz | 29 | 84 | Recurrence 31.03% | Shoulder dislocation in patients older than 60 years of age44 | Rapariz et al. | 29 | 72 | Recurrence 31.03% | Int J Shoulder Surg | 19 | – |
| The pectoralis major tendon as a reference for restoring humeral length and retroversion with hemiarthroplasty for fracture | 2009 | Vilà et al. | 20 | NA | Distance pect. major-humeral head: 5.64cm Distance insertion of pect major-posterior implant flange: 1.06cm Pect major-implant flange angle: 24.65 | The pectoralis major tendon as a reference for restoring humeral length and retroversion with hemiarthroplasty for fracture48 | Torrens et al. | 20 | NA | Distance pect. major-humeral head: 5.64cm Distance insertion of pect major-posterior implant flange: 1.06cm Pect major-implant flange angle: 24.65 | J Shoulder Elbow Surg | −4 | 1.93 |
| Functional outcomes after arthroscopic repair of massive rotator cuff tears: influence of the application of platelet-rich fibrin | 2011 | Antuña et al. | 28 | 12 | Δ Constant scale PRP 26 No PRP 30 | Platelet-rich fibrin in arthroscopic repair of massive rotator cuff tears: a prospective randomised pilot clinical trial35 | Antuña et al. | 28 | 12 | Δ Constant scale PRP 26 NO PRP 30 | Acta Orthop Belg | 21 | 0.63 |
| Clinical outcome and prognostic factors of revision arthroscopic rotator cuff tear repair | 2011 | Calvo et al. | 40 | 12 | Δ Constant scale 15.2 | Clinical outcome and prognostic factors of revision arthroscopic rotator cuff tear repair54 | Valencia et al. | 51 | 25 | Δ Constant scale 26.42 Δ Simple Shoulder Test 3,82 | Knee Surg Sports Trauma Arthrosc | 68 | 3.23 |
| Medium term results of unipolar modular radial head arthroplasty | 2011 | Cecilia et al. | 32 | 30 | MEPS 84% excellent or good results; 3 cases of compromised radial nerve 3 cases of capitellum erosion 1 luxation 1 incomplete resection | Medium term results of unipolar modular radial head arthroplasty43 | Martín Fuentes et al. | 44 | 21 | MEPS 82% excellent or good results; 2 loosenings | Rev Esp Cir Ortop Traumatol | 26 | |
| Systematic review after 6 years of olecranon fractures. Clinical and functional results. | 2011 | Cervera et al. | 93 | 36 | 87.4% Good or excellent Range of motion >50 | Treatment of comminuted olecranon fractures with olecranon plate and structural iliac crest graft38 | Cervera et al. | 3 | 23 | 100% good or excellent Flexion 115 Extension −20 Pronation 71 Supination 80 | Acta Orthop Belg | 21 | 0.63 |
| Use of adipose-derived stem cells in an experimental rotator cuff fracture | 2011 | Encinas et al. | 56 | 2 | No difference in tensile strength at 4 and 8 weeks | Use of adipose-derived stem cells in an experimental rotator cuff fracture animal model36 | Barco et al. | 44 | 2 | No difference in tensile strength at 4 and 8 weeks | Rev Esp Cir Ortop Traumatol | 42 | 0.09 |
| Progression of deformity during fracture healing of humeral fractures treated conservatively | 2011 | Foruria et al. | 106 | 12 | ↑ retroversion of the head 7.5 18.75% progression of greater tuberosity | Proximal humeral fractures treated conservatively settle during fracture healing40 | Foruria et al. | 89 | 12 | ↑ retroversion of the head 7.1 <20% progression of greater tuberosity | J Orthop Trauma | 39 | 0.92 |
| Treatment of fracture sequelae of the proximal humerus: comparison of hemiarthroplasty and reverse total shoulder arthroplasty. | 2011 | Isart et al. | 14 | 32 | HA Group Δ Constant scale 18.16 PI Group Δ Constant scale 22.19 | Treatment of fracture sequelae of the proximal humerus: comparison of hemiarthroplasty and reverse total shoulder arthroplasty34 | Alentorn Geli et al. | 32 | 50 | HA Group Δ Constant scale 14.6 PI Group Δ Constant scale 26.6 | Arch Orthop Trauma Surg | 41 | 2.33 |
| Morbidity and mortality of surgically treated proximal humerus fractures | 2011 | Isart et al. | 97 | 96 | Autonomy 79.5% Mortality 14% | Morbidity and mortality of surgically treated proximal humerus fractures42 | Isart et al. | 94 | 96 | Autonomy 79.5% Mortality 18.6% | Rev Esp Cir Ortop Traumatol | 40 | 0.09 |
| Plasma rich in growth factors (PRGF) in arthroscopic rotator cuff repair: a randomised, clinical trial with 69 patients | 2011 | Molano Muñoz et al. | 69 | 12 | PRFC Group 78% satisfaction Control group 77% satisfaction | Plasma rich in growth factors (PRGF) in arthroscopic rotator cuff repair: A randomised, double-blind, controlled clinical trial45 | Ruiz Moneo et al. | 69 | 12 | PRGF group ΔUCLA: 8.3 Control group ΔUCLA: 9 | Arthroscopy | 22 | 3.29 |
| Decreased axial coracoid inclination angle is associated with rotator cuff tears | 2011 | Sánchez et al. | 82 | NA | Rotator group Angle 1 (A1) 57.06 Angle 2 (A2) 49.17 Control group: A1: 132.52 A2: 144.34 | Decreased axial coracoid inclination angle is associated with rotator cuff tears53 | Torrens et al. | 100 | NA | Rotator Group Angle 1: 49.7 Angle 2: 76.45 Control group A1: 132.33 A2: 144.34 | J Orthop Surg (Hong Kong) | 47 | 0.77 |
| Treatment of complex proximal humeral fractures in elderly patients with reverse shoulder arthroplasty versus hemiarthroplasty. Prospective study | 2011 | Sebastiá-Forcada et al. | 32 | 22.7 | Δ Anterior flexion 64 Δ abduction 63 | Reverse shoulder arthroplasty versus hemiarthroplasty for acute proximal humeral fractures. A blinded, randomised, controlled, prospective study46 | Sebastiá-Forcada et al. | 62 | 28.5 | Δ Anterior flexion 41 Δ abduction 34,2 | J Shoulder Elbow Surg | 43 | 2.75 |
IF, impact factor of the journal; FU, follow-up in months; No, sample size, NA, not applicable; NA, not available Δ, pre and postoperative differences.
The publication rate was not significantly related to the study subject matter (p=0.30), neither were the type of study, level of evidence, sample included or follow-up of podium presentations determining factors of the probability of publication (p=0.35; p=0.96; p=0.19 and p=0.17, respectively). Lastly, delay in publication did not affect the impact factor which was obtained with regards to the indexed journal (p=0.92).
DiscussionThe SECHC congress is celebrated biannually and is the benchmark state congress in Spain in shoulder and elbow disorders. This paper shows that at least 20% of the podium presentations are published in indexed journals.
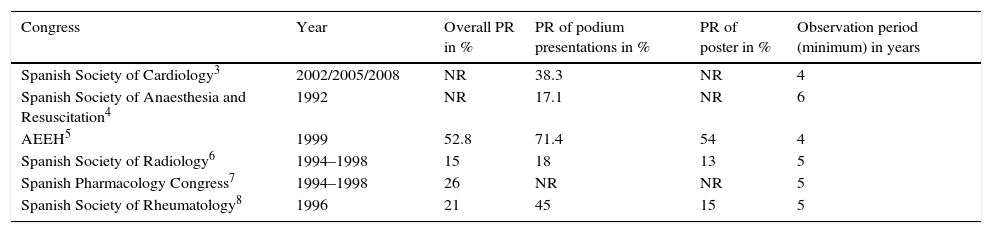
The publication rate of different medical congresses celebrated in Spain3–8 is very varied (Table 2), and the majority are based on congresses celebrated during the last century (1992–1999). The Spanish Association for the Study of the Liver achieved the best publication rate of a Spanish Medical congress,5 with 71.4% of its podium presentations and 54% of its posters published in journals four years after the congress (1999). Only the Spanish Society of Cardiology3 has published results from congresses celebrated between 2002 and 2008, and has reported 38.4% as its publication rate of podium presentations at 4 years. In the sub-speciality of shoulder and elbow we only have knowledge of the publication rates of podium presentations in congress sessions of the AAOS, as being 66% after a minimum follow-up of 3 years.12
Publication rate of Spanish congresses.
| Congress | Year | Overall PR in % | PR of podium presentations in % | PR of poster in % | Observation period (minimum) in years |
|---|---|---|---|---|---|
| Spanish Society of Cardiology3 | 2002/2005/2008 | NR | 38.3 | NR | 4 |
| Spanish Society of Anaesthesia and Resuscitation4 | 1992 | NR | 17.1 | NR | 6 |
| AEEH5 | 1999 | 52.8 | 71.4 | 54 | 4 |
| Spanish Society of Radiology6 | 1994–1998 | 15 | 18 | 13 | 5 |
| Spanish Pharmacology Congress7 | 1994–1998 | 26 | NR | NR | 5 |
| Spanish Society of Rheumatology8 | 1996 | 21 | 45 | 15 | 5 |
NR, not reported; PR, publication rate.
The reasons for the low SECHC publication rate found may differ. The fact that the SECHC congress is a sub-specialty of orthopaedic surgery and trauma (specialty) could explain the differences with regard to the publications rates mentioned for Spanish congresses. Different publications have proposed reasons for explaining the non publication of podium presentations. Sprague et al.1 studied the reasons for non publications of abstracts presented at the AAOS congress. Out of the 306 works for which no publication was found, 199 authors responded to the survey. Out of the 199 authors, 72 (36.2%) declared that the work had been published whilst 71 authors (35.7%) had never sent off their presentations. The major obstacles stated by the authors for not sending off their scientific studies was lack of time1 and lack of interest in publishing. Fear of rejection was another reason stated for not sending off a podium presentation for publication.55
The majority of studies presented at the SECHC congress which were later published suffered from changes over the publication process. In our study, half of the works published result in a higher sample, whilst almost 25% reduce the sample in later publication (Table 1). The works by De Casas39 and Sebastiá-Forcada46 are the ones with a larger sample, with the patient numbers increasing by 100%. Bhandari et al.10 reported an almost 10% reduction of the sample in the works published compared to the abstract given at the AAOS congress, whilst Preston et al.55 observed almost a 20% reduction in the sample of the studies previously expressed in the congress of the Orthopaedic Trauma Association. With regard to follow-up, all the studies except 338,43,45 maintained the same follow-up time or increased it considerably. As an example, the work published by Torrens et al.51 changed from a 12 month follow-up recorded in the congress abstract to a 24 month follow-up in subsequent publication. De Casas39 practically tripled follow-up from podium presentation to publication. With regard to the conclusions, only the work of Silberberg47 showed different conclusions between podium presentation and publication. In this case, the podium presentation expressed the results of a surgical technique (SLAP injury repair through anterior portal vein), whilst the subsequent publication extended the study with a comparative work between 2 specific techniques. These findings appear to be in keeping with other publications which study the consistency between abstracts and posterior publications. The work of Preston et al.55 delves into the differences between the podium presentations from the congress of the Orthopaedic Trauma Association between the years of 1994 and 1997. The authors of this study found that there was a 93.4% coincidence rate in the conclusions between congress abstracts and later publications. 56.3% of the works which were published used the same sample as in the previous podium presentation whilst 25.5% increased it. The reasons stated for changing the presented data were diverse. Often podium presentations were the preliminary results of an investigation with regards to follow-up and sample size. Only 10% of the studies which contained changes to the content of the work offer an explanation, according to Preston et al.55 Among them, the loss of follow-up of the patients included in the study was the main reason for change. Bandhari et al.,10 in contrast, identified the delay in publication as the only predisposing factor between the oral communication at a congress and subsequent publication.
The study topic was not related to the probability of gaining a posterior publication in our analysis. Schulte et al.27 found differences in the publication rate according to the work design (prospective vs retrospective) and the level of scientific evidence (I–II vs III–IV) in the study of the German orthopaedics congress, but there were no differences in the study topic. Schulte et al.27 and Kleine-Konig et al.22 found that the abstracts corresponding to works with a significant main outcome were more likely to be published than those with clearly non significant outcomes. Furthermore, multicentre studies and biomechanical studies27 obtained higher publication rates. Cifuentes et al.5 identified the type of presentation (oral or poster) as the only determining factor for final publication of an abstract presented at a meeting of the Spanish Association of the Study of Liver Diseases.
Scientific meetings in Spain, such as the Electrophysiology, Arrhythmias and cardiac stimulation meeting have strictly limited the time for oral presentations. Only those presentations which are deserving of awards due to their originality or level of scientific evidence are presented at the congress. This focus could help to improve the number of studies published which are presented previously in SECHC congresses. Another measure which would help to improve the rate of publication of the SECHC would be that or promoting the study of high levels of evidence: prospective randomised studies, multicentre or biomechanical studies, as has been determined by other authors.27 Consolidation of the rising trend in the SECHC publication rate is expected, like that observed in this study in the 2007–2011 period due to the scientific development of society itself. Publications in Spain in the Science Citation Index Expanded data base increased by over 600% between 1980 and 2003, a far higher rise than the total increase of the data bases (100%).9 Despite the research internationalisation process and the drop in publications in the Spanish language,9 the indexation of the spanish journal of orthopaedic surgery and traumatologyin Medline/Pubmed from 2013 will help Spanish authors to familiarise themselves with a publication in their own language. The Spanish Society of Cardiology has identified3 the “Revista Española de Cardiología” as the main publication for authors of works presented at their congresses. 37.1% of the works published from the congress were present in this journal.
This study has several limitations. Firstly, the reasons for non publication of communications have not been analysed nor is the number of studies which initiated some type of review process in indexed journals available. Secondly, the search for posterior publications through PubMed may lead to an underestimation of the analysed publication rate.
ConclusionsThe majority of oral communications presented in the SECHC congresses are not published in indexed journals. The differences between the published communications and their previous oral presentations do not appear to be significant.
Level of evidenceLevel of evidence IV (systematic review).
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments have been performed on humans or animals in this research.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Miquel J, Fernández-Muñoz S, Romero A, Pelfort X, Torrens C. ¿Publicamos lo que predicamos? Tasa de publicación de los congresos de la Sociedad Española de Cirugía de Hombro y Codo. Rev Esp Cir Ortop Traumatol. 2018;62:35–46.
