





The objective of this study was to compare the clinical outcomes of surgical treatment using tension band with needles and preformed plates in type II olecranon fractures according to the Mayo classification in patients older than 65 years.
Materials and methodA descriptive, retrospective study of 49 patients with a mean age of 75.1 years who underwent surgery olecranon fracture using 2 different fixing systems. The Mayo classification was used to define them, excluding type I and III, and the VAS to assess postoperative pain. Patients were assessed functionally by the questionnaire Quick DASH. All measurement was performed with goniometer and joint balance serial radiographs at one month, 3, 6 and 12 months. Minimum follow-up was one year.
ResultsIn 26 patients the tension band was used and the preformed plates in 23. There were no statistically significant differences in functional outcomes, joint balance or postoperative VAS between the 2 groups. There were a greater proportion of patients who had to be operated because of problems related to osteosynthesis material in those in which preformed plates were used.
ConclusionTreatment of olecranon fractures with tension band with needles and cerclage remains the surgery of choice in patients older than 65 years.
El objeto de este estudio fue comparar los resultados clínicos del tratamiento quirúrgico mediante banda a tensión con agujas y las placas preconformadas en las fracturas de olécranon tipo ii de Mayo en pacientes mayores de 65 años.
Material y métodoEstudio descriptivo, restrospectivo, de 49 pacientes con una edad media de 75,1 años, intervenidos quirúrgicamente de fractura de olécranon mediante 2 sistemas distintos de fijación. Se empleó la clasificación de Mayo para definirlas, excluyendo los tipos i y iii, y la EVA para valorar el dolor postoperatorio. Los pacientes fueron evaluados funcionalmente mediante el cuestionario Quick DASH. A todos se les realizó medición del balance articular con goniómetro y radiografías seriadas al mes, 3, 6 y 12 meses. El seguimiento mínimo fue de un año.
ResultadosEn 26 pacientes se empleó la banda a tensión y en 23, las placas preformadas. No hubo diferencias estadísticamente significativas en los resultados funcionales, el balance articular ni la EVA postoperatoria entre los 2 grupos. Sí destaca una mayor proporción de pacientes a los que hubo que intervenir por problemas relacionados con el material de osteosíntesis en aquellos en los que se emplearon placas preformadas.
ConclusionesEl tratamiento quirúrgico de las fracturas de olécranon tipo ii en pacientes mayores de 65 años mediante el uso de placas preformadas no aportó mejores resultados que los obtenidos mediante la fijación con banda a tensión.
Olecranon fractures comprise at least 20% of all proximal fractures of the forearm.1 Because these are intraarticular fractures they require anatomic reduction and restoration of articular congruence to obtain a good clinical outcome and prevent the development of osteoarthritis.2 Stable fixation is also necessary to enable early mobilisation to prevent stiffness of the elbow. Several fixation systems are used, including tension bands, fixation plates and intramedullary nails.3 However, there is some controversy regarding the outcomes and complications of surgery to these fractures in elderly patients, specifically precarious osteosynthesis, due to poor bone quality and problems with the surgical wound.4,5 Excision of the fractured proximal fragment and advancement of the triceps for its reinsertion have been suggested as alternatives for these patients, although problems have been raised regarding weakness of elbow extension.6 There are few papers on the conservative management of displaced fractures of the olecranon in elderly patients. However, there are some that show acceptable outcomes in those at more surgical risk.7,8
The aim of our study was to assess the long-term outcomes of surgical treatment by open reduction and osteosynthesis of olecranon fractures in patients aged over 65 years, and to compare clinical outcomes between the use of tension bands with cerclage wires and needles with fixation plates.
Materials and methodAn observational, descriptive and retrospective study was undertaken of patients over the age of 65 years operated in our hospital for isolated unstable olecranon fracture between January 2005 and December 2014, with a minimum follow-up of one year.
Out of a total of 66 patients, 17 were not included in the study as they had not completed minimum follow-up (change of hospital, death or lack of data), which reduced the number patients in the series to 49.
We used the Mayo classification of olecranon fractures as described by Morrey9 based on different factors such as displacement, conminution and elbow stability. Only patients who presented type II (A and B) fractures were included in the study.
Mean follow-up was 14.8 months, during which time X-rays were taken at 1, 3, 6 and 12 months after surgery. Anteroposterior and lateral views were used in all cases.
Postoperative pain was assessed using the VAS scale and articular movement using a goniometer. The QuickDASH questionnaire in Spanish was used for functional evaluation.
The non-parametric Mann–Whitney U test was used to establish statistically significant differences (p<0.05) in functional outcomes.
A posterior elbow approach was used in all cases. Kirschner needles of 1.6–1.8mm in diameter and 1–1.2mm wire was used for fixation with tension bands. Synthesis was achieved leaving the intramedullary needles or nailing them to the anterior cortex of the ulna, making a figure-of-eight wire loop, which was manually tightened in the proximal part after passing through the distal orifice in the ulna (Fig. 1).

The plates used had a profile of 3.1mm, with proximal locking screws of 2.7mm and distal screws of 3.5mm, which could be either locking or compression (Fig. 2).
Results
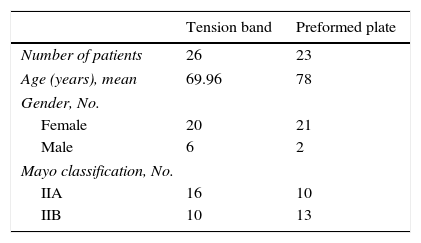
The mean age was 75.1 years (65–89). The sample comprised 41 females and 8 males. In 22 cases the left elbow was affected and in 27 the right. The distribution according to fracture type was 26 cases type IIA and 23 type IIB. Of the total number of patients, 26 were operated using a tension band with cerclage wires and Kirschner needles (16 IIA cases, 10 IIB cases), compared to 23 in whom a fixation plate and screws were used (10 IIA cases, 13 IIB cases) (Table 1).
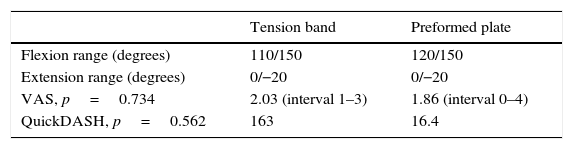
The mean articular movement was 143° flexion and −3.2° extension deficit for the patients operated using cerclage wires and needles compared to 146° flexion and extension deficit −4.3° for those in whom fixation plates were used. There were no statistically significant differences between either group (p=0.278).
Both groups had very similar outcomes in terms of postoperative pain assessed using the VAS scale. The patients operated using needles and cerclage wires presented a mean of 2.03 compared to 1.86 for those in whom plates and screws were used. There was no statistically significant relationship (p=0.734) (Table 2).
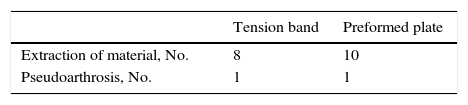
In our series, 18 patients had to undergo a second operation to remove the osteosynthesis material due to discomfort or problems with the surgical wound. Eight patients had been operated using needles and cerclage wires (comprising 30.7% of those operated using tension bands) compared to 10 patients who underwent removal of the plate and screws (43.4% of the patients in whom this system was used).
In terms of complications, one patient presented early postoperative infection and 2 patients presented pseudoarthrosis. All of these patients required a further operation. The 2 patients with pseudoarthrosis had a type IIB fracture, one was treated with cerclage wires and needles and the other with preformed plate and screws (Table 3).
The mean QuickDASH score was 16.3 points for the patients operated using a tension band compared to 16.4 for those who underwent osteosynthesis with plate and screws. This difference was not statistically significant (p=0.562).
DiscussionThere are few research studies that compare clinical outcomes after osteosynthesis using plate and screws and tension band with needles and wires in olecranon fractures. There are none that focus on the male or female elderly population, although there are articles that highlight an increased incidence of olecranon fractures due to low energy trauma from the seventh decade of life.1,10
In our study, as in those that compare both fixation systems, we found no statistically significant differences with regard to functional outcomes and postoperative pain, although these outcomes were slightly better in the patients operated using plate and screws.
One thing makes the result of this study different to that of others1,11: the amount of reoperations to remove the osteosynthesis material due to discomfort or surgical wound closure problems was rather higher than in most previous studies. The differentiating element was that more patients were reoperated in whom a preformed plate rather than a tension band was used. This might have been due to the poor quality of the tissue of the patients studied due to the greater age range, meaning that a subcutaneous plate was less well tolerated. A second hypothesis is that the material used was slightly thicker than the latest low profile plates. A third and more remote hypothesis is that the surgical technique needs to be refined to ensure that the osteosynthesis material adapts further to the bone. However we doubt that this is the problem.
Unlike some previous studies, no nerve injury was observed in the patients operated using tension bands.12
We can conclude from our study that using preformed plates and screws did not provide better functional outcomes for olecranon fracture patients aged over 65 years. Therefore, from a cost-benefit perspective, we consider that the tension band system with needles and cerclage wires is more appropriate for these cases. Furthermore, the number of operations to extract the osteosynthesis material was higher in our study in the patients operated with plate and screws. This involves greater expenditure and a second operation for the patient.
Level of evidenceLevel of evidence IV.
Ethical disclosuresProtection of humans and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their centre of work regarding the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflict of interestsThe authors have no conflicts of interests to declare.
Please cite this article as: Liñán-Padilla A, Cáceres-Sánchez L. Fracturas de olécranon tipo ii en mayores de 65 años. ¿Banda a tensión o placa preformada? Análisis y resultados. Rev Esp Cir Ortop Traumatol. 2017;61:339–342.
