




Calcific myonecrosis is a rare post-traumatic sequela almost exclusively located in the lower extremity, which can be mistaken for an aggressive primary neoplasm. This lesion, initially described by Gallei and Thompson in 1960, is characterized by the formation of a calcified mass that appears decades after trauma. The pathophysiologic mechanism is not fully understood, although the lesion most likely results from post-traumatic ischaemia and it may be associated with a common peroneal nerve injury. The typical radiographic image is a fusiform soft tissue mass with linear calcifications. The treatment of choice is conservative in asymptomatic patients because the surgical treatment has a high complication rate.
We report four cases of calcific myonecrosis treated surgically in our hospital. Three of the cases had an infection as a complication that required subsequent debridement and special therapies to achieve the resolution of the cases.
La mionecrosis calcificante es una rara secuela postraumática que se localiza casi exclusivamente en la extremidad inferior, y que puede ser confundida con una neoplasia primaria agresiva. Esta lesión, descrita inicialmente por Gallei y Thompson en 1960, se caracteriza por la formación de una masa calcificada que aparece varias décadas después de un traumatismo. El mecanismo fisiopatológico no es conocido, sin embargo la lesión parece que es debida a una isquemia postraumática y puede asociarse con una lesión del ciático poplíteo externo. La imagen radiográfica típica es una masa de partes blandas fusiforme con calcificaciones lineales. El tratamiento de elección es conservador en los casos asintomáticos ya que el tratamiento quirúrgico tiene un alto porcentaje de complicaciones.
Presentamos 4 casos de mionecrosis calcificante tratados quirúrgicamente en nuestro hospital. Tres de los casos se infectaron por lo que precisaron sendos desbridamientos y terapias especiales para su resolución definitiva.
Calcific myonecrosis is a rare complication that has been described as a chronic sequela of a trauma in the lower limb. It is associated in the majority of cases to a nervous and/or vascular lesion with or without clear evidence of compartment syndrome.
The patients indicate a history of a fracture of the femur or tibia that evolved with vascular and/or nervous complications. After many years they note the presence of a painless tumour in the soft tissues, located in the antero-external part of the leg. Physical examination shows that a large soft tissue mass is located in the anterior compartment of the leg, which is fluctuant, painless and sometimes under tension. Its typical radiographic appearance is of a large fusiform soft tissue mass with linear calcifications inside with well defined borders.
These radiographic findings should allow differential diagnosis against other causes of soft tissue masses such as abscesses, myositis ossificans or soft tissue sarcomas, the latter being a reason that patients are sent to tumour pathology units.
The aim of our work was to present 4 cases of calcific myonecrosis of the leg treated in our hospital over the last few years and carry out a review of the literature of this rare disease that can cause diagnostic problems. Three of our patients were sent to the Tumour Unit with the tentative diagnosis of soft tissue sarcoma and the fourth went to the emergency department with a suspected acute soft tissue infection in the lower limb.
Clinical casesCase 1The first case was a 55-year-old male, with a history of a supracondylar femur fracture that was treated with osteosynthesis, 34 years before he was sent to our tumour unit. In the anamnesis, the patient referred to having presented repeated haematoma on the leg after the operation, which required successive debridement. As a result he was left with a lesion in the sciatic nerve that required a tendon transposition to correct the residual equinus. He later presented symptoms of swelling in the limb, which would clear up of their own accord, until nearly 4 years ago when he went to the hospital with a persistent tumour mass that did not disappear as previously: the diagnosis was of a synovial cyst. Due to the progressive growth of the tumour and increased pain, they performed a magnetic resonance imaging (MRI) that reported a soft tissue sarcoma, which was the reason he was sent to the tumour unit. On examination he presented good general health, with no toxic syndrome; what stood out was the presence of a soft tissue mass of about 20cm, which was hard, well defined and under tension, and took up the entire anterolateral compartment of the leg. The radiographic images showed a fusiform tumour with calcifications inside and with erosion at tibial cortical level (Fig. 1A). In the computerized tomography (CT), we could see a soft tissue mass in close contact with the anterior cortex and lateral cortex of the tibia, with multiple irregular central and peripheral calcifications (Fig. 1B). In the MRI (Fig. 1C), the lesion had hypointense areas that eroded the tibial cortical bone by disrupting it. We could see images suggestive of calcifications and irregular and hypointense margins, which indicated haemosiderin secondary to intralesional haemorrhage. Despite the fact that the clinical history and additional tests did not suggest a sarcoma, we carried out a biopsy that eliminated the presence of tumour cells. Later extensive debridement of the soft tissue mass revealed a coffee-coloured liquid, multiple elongated calcifications, degenerate mucoid tissue with muscle necrosis and remains of organized haematoma. We were able to extract nearly all of the mass and the cultures taken were negative. The histopathological study showed muscular necrosis and calcified bone matter, which suggested a diagnosis of calcific myonecrosis. The evolution was satisfactory, with correct healing of the wound, and the patient improved clinically. Seven years later there was no evidence of a recurrence.
 AP and profile X-rays of the left leg showing a large soft tissue lesion with irregular linear calcifications. (B) Consecutive CT slices with contrast showing the anterior position of the soft tissue mass, with linear, central irregular and irregular calcifications, of complex cystic content. We can also see the ossification of the interosseous membrane. (C) MRI axial T1-weighted sequences (right) and T2 (left), which show that the soft tissue mass has a heterogeneous appearance, corresponding to a complex liquid collection, while the calcifications have a very low signal in both sequences.")
(A) AP and profile X-rays of the left leg showing a large soft tissue lesion with irregular linear calcifications. (B) Consecutive CT slices with contrast showing the anterior position of the soft tissue mass, with linear, central irregular and irregular calcifications, of complex cystic content. We can also see the ossification of the interosseous membrane. (C) MRI axial T1-weighted sequences (right) and T2 (left), which show that the soft tissue mass has a heterogeneous appearance, corresponding to a complex liquid collection, while the calcifications have a very low signal in both sequences.
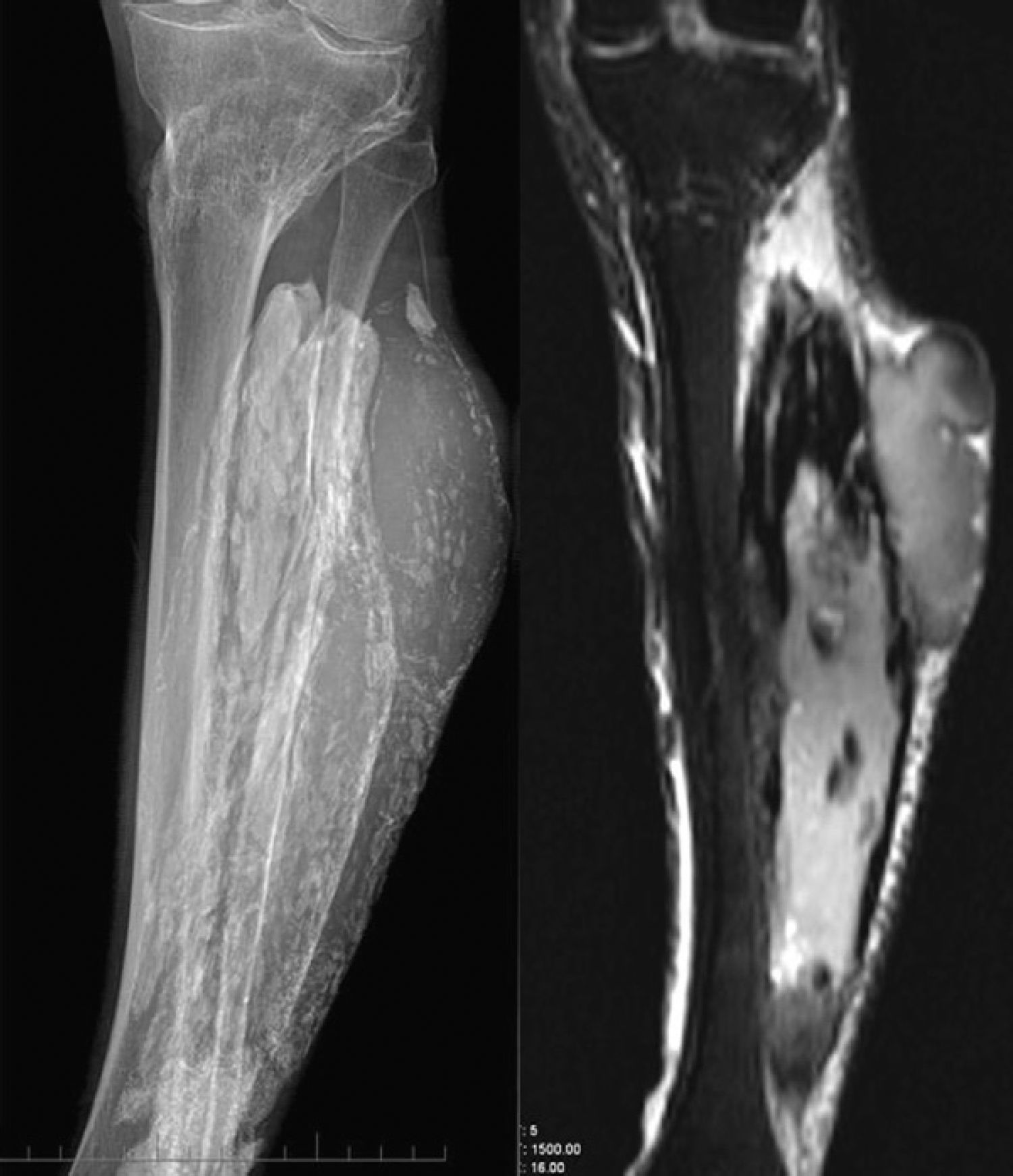
A 64-year-old patient with a history of a tibia fracture 12 years before, which was treated with a long-leg plaster. In the anamnesis carried out, the patient remembered the presence of repeated haematomas on the leg, which required repeated punctures to clear. As a consequence of the whole process, there was a residual equinus, which required a plasty of the posterior tibia. A few years before coming to our surgery, he noticed a painless hard tumour, which was progressively growing. Due to its size, he was sent to our centre with a suspected malignant tumour or myositis ossificans. After a radiographic study, the MRI established the diagnosis of calcific myonecrosis (Fig. 2). Given that he was asymptomatic and because of the possible complications from surgical treatment, we decided that, with the patient's consent, we should monitor his progress. Three years later, a small trauma produced a wound through which haematic and slough drained. It was operated on with a surgical debridement of the lesion and haematic material, necrotic muscle and multiple calcifications were removed. The wound was finally closed with drains. Two weeks later there was a dehiscence of the surgical wound with the release of a purulent liquid that gave positive cultures to Staphylococcus aureus and enterobacter, forcing new debridement and specific antibiotic treatment. The wound later needed new debridement, applying growth factors and VAC therapy so that it could close. Despite all the treatments performed, there is still a chronic fistula, which is well tolerated by the patient.
 and MRI coronal slices in T1-weighted sequences (central) and T2 (left), identifying typical calcifications, together with the soft tissue component (which can be better seen in the MRI) and which has a complex cystic appearance. We can also see the consolidated fracture of the proximal tibial metaphysis.")
AP X-ray of the leg (right) and MRI coronal slices in T1-weighted sequences (central) and T2 (left), identifying typical calcifications, together with the soft tissue component (which can be better seen in the MRI) and which has a complex cystic appearance. We can also see the consolidated fracture of the proximal tibial metaphysis.
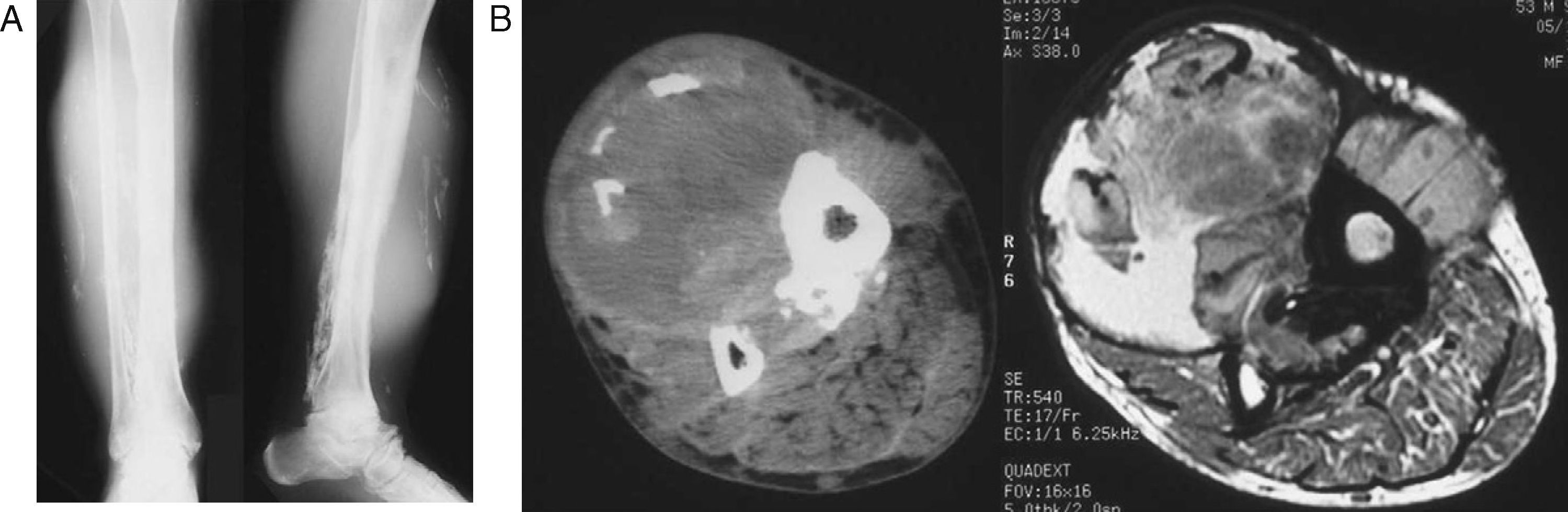
A 54-year-old male with a history of idiopathic thrombocytopenic purpura (ITP) and fracture of the tibia and fibula treated with plaster when he was 34 years old, who was sent to our tumour unit having been diagnosed with soft tissue sarcoma. In the anamnesis, the patient explained that on the days after the trauma the plaster was removed several times due to intense pain and the examination showed a haematoma on the leg that was attributed to his underlying disease. The fracture healed with no problems but as a consequence he was left with a residual equinus that required tendon transposition. He later had repeated haematomas on the leg that were attributed to the disease and which improved with rest. A few months before coming to the surgery, the patient presented new symptoms of swelling on the leg and the appearance of a painful soft tissue mass, which is why he had an MRI that suggested soft tissue sarcoma. On examination we could see a soft tissue mass of about 15cm, which was purplish, under tension, mobile and poorly defined. The X-ray (Fig. 3A) showed a soft tissue mass with linear calcification, eroding the cortex of the tibia and fibula. In the CT and MRI (Fig. 3B), we could see an intramuscular mass with a central hemorrhagic area and calcifications inside. After the corresponding haematological study for the underlying disease, we performed a surgical debridement, obtaining necrotic muscle tissue, haematoma remains and many calcifications. The posterior evolution was towards infection, which needed specific antibiotic treatment and multiple debridements; these left a residual fistula, which closed up 5 years after the intervention. In the years of follow-up, there were no signs of recurrence.
 AP X-rays and profile of the right leg showing a soft tissue mass, with irregular calcifications in a peripheral location. (B) CT axial slices (right) and T2 weighted MRI sequences (left): we can see the anterior location, in close contact with the tibial cortical of the lesion, which has a heterogeneous appearance, partially cystic in both the CT and MRI. We can also see ossification of the interosseous membrane.")
(A) AP X-rays and profile of the right leg showing a soft tissue mass, with irregular calcifications in a peripheral location. (B) CT axial slices (right) and T2 weighted MRI sequences (left): we can see the anterior location, in close contact with the tibial cortical of the lesion, which has a heterogeneous appearance, partially cystic in both the CT and MRI. We can also see ossification of the interosseous membrane.
The fourth case was a 77-year-old patient with a history of type 2 diabetes mellitus and a fracture of the tibia and fibula 30 years previously. The patient went to the emergency department with fever symptoms of a urinary aetiology, which is why antibiotic treatment was started. Three days later he returned with a temperature of 39°C and pain and swelling in the left leg. On examination we saw a swollen, erythematous calf area of stony consistency and areas of fluctuation. The X-ray showed linear calcifications all along the leg. With the initial diagnosis of pyomyositis, we carried out extensive debridement of the affected area, obtaining purulent material, necrotic muscle and elongated calcifications; we closed the wound partially and put drains in place. The patient explained that after the fracture he had presented a compartment syndrome that meant he had to have repeated drains and was admitted to another hospital for 4 months, but he had had no complications since then. Having assessed the patient's history, the X-rays and the surgical findings, we established the diagnosis of calcific myonecrosis. The cultures were positive for E. coli and we set up specific antibiotic treatment for 3 months. The patient required debridement several times and VAC therapy before complete closure of the wounds. After a year there was no recurrence of the process.
DiscussionCalcific myonecrosis was first described by Gallie and Thompson1 in 1960. Its most common location is the anterior and external compartments of the leg, although cases have been described in the foot and upper limb.2,3
These patients consult because of a soft tissue mass that appears in the anterior and external compartment of the leg, which has evolved over several months or years and has suddenly increased in size. On undertaking an anamnesis, the history is similar in all cases; they refer to a previous trauma to the leg several years before (10–64 years), associated or not to tibia and fibula fractures, and they explain that they had complications that they cannot specify (repeated haematoma that meant they had to have debridement, neurological lesion, etc.) but that point to a possible compartment syndrome.
It is accepted that calcific myonecrosis is a rare sequela of compartment syndrome but its pathophysiological mechanism is unknown. The most commonly accepted hypothesis is that after the trauma there is a compartment syndrome that causes a decrease in blood supply to a limited area, which leads to a cystic degeneration, muscle necrosis and fibrosis; over the years, new haemorrhagic episodes cause the mass to increase and calcify.1,4
From a clinical point of view, we can see a large soft tissue mass that occupies nearly the entire anterior and external compartment of the leg, which can be painful or painless when touched and sometimes under tension. The X-ray shows a soft tissue mass located in these leg compartments, which is fusiform and has linear calcifications with trabecular bone formation and peripheral calcification. This can be accompanied by erosion and minimal periosteal reaction of the neighbouring bones.
The CT allows the location and the typical shape of the calcifications to be seen better. It is useful when establishing a differential diagnosis with bone tumours and soft tissue sarcomas.
The typical X-ray picture, together with the anamnesis (which emphasises there was a trauma on the limb several years earlier, together with a vascular and/nervous peripheral lesion), can be enough to diagnose calcific myonecrosis.
Differential diagnosis must be considered with tumours and inflammatory diseases that can lead to soft tissue calcification sarcomas (synovial sarcoma, epithelioid sarcoma or soft tissue osteosarcoma), or afflictions such as myositis ossificans, dermatomyositis, polymyositis, tumoral calcinosis, diabetic myonecrosis or calcific tenosynovitis, among others.2,5–7 An abscess in the soft tissue should also be taken into account in the differential diagnosis,2 although it is rare because it is generally produced in cases where patients have been diagnosed and treated.
The MRI is useful in establishing the extension of the lesion, but its interpretation without X-rays can lead to diagnostic errors, given that the calcifications (a characteristic feature) are not seen in MRI images. The non-calcified part has a signal similar to that of a liquid or that of a haemorrhagic effusion, with an intermediate, relatively homogeneous signal in T1 weighted sequences and a variable heterogeneous signal in T2 weighted sequences, with areas that appear solid, with an intermediate signal in both sequences.
The use of an intravenous contrast allows for better definition of the areas of complex cysts, but its systematic use does not provide additional information.2
However, if there is diagnostic doubt we can carry out a puncture biopsy that will eliminate a malignant process, as occurred in our first case.
Conservative treatment with periodic monitoring of the patient is recommended by several authors,3,8,9 given that infectious complications are common when surgical treatment is chosen. However, there are authors who support extensive debridement with primary or second intention closure.2
We think that the conservative option can always be valid as long as there is periodic monitoring of the patient. If the mass becomes painful or grows, surgical treatment may have to be undertaken; this will consist of excision of the maximum amount of haematoma, necrotic muscle and calcifications, primary closure and drain placement. The most common complication is infection,3,6,9 which would require new debridement and specific antibiotic treatment. In many cases a residual fistula remains for many years until it closes on its own, although a recurrence cannot be ruled out. Three of our cases developed an infection; however, one of them initially presented, without surgical intervention, an abscess in the leg with positive cultures of staphylococcus and pseudomonas. It was when additional tests were carried out that the diagnosis and origin of the abscess was suspected.
To conclude, calcific myonecrosis is a rare, not very well known disease that can lead to a misdiagnosis, especially of soft tissue sarcomas, which is why many of these patients are sent to the Tumour Pathology Unit. A simple X-ray is fundamental to guide the diagnosis. The most widely accepted treatment is conservative with periodic controls, because surgical treatment is a source of complications, especially of infection, as occurred in 3 out of 4 of our cases.
Evidence levelEvidence level IV.
Conflict of interestsThe authors have no conflict of interests to declare.
Ethical DisclosuresProtection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of Data. The authors declare that no patient data appears in this article.
Right to privacy and informed consent. The authors declare that no patient data appears in this article.
Please cite this article as: Portabella F, et al. Mionecrosis calcificante de la pierna. Rev esp cir ortop traumatol. 2012;56(1):46-50.
