



Distal radius fractures (DRF) are being a bigger burden for health resources as changes continue to happen in our population demography and in management strategies, so a precise epidemiologic comprehension is mandatory. We present a DRF epidemiology study and we compared it with other sanitary areas of the Iberian Peninsula and Europe.
MethodEvery DRF in our sanitary area registered between 2017 and 2018 in patients older than 18 years old were observational and retrospectively recorded and classified using AO-OTA classification. Age, sex, season of the year, mechanism of injury, presence of associated injuries and type of treatment were analysed.
Results1121 DRF in 1108 patients, 903 women (81.5%) and 205 men (18.5%), were registered. Left side was affected in 612 cases (54.6%) and right side in 509 cases (45.4%). The average age of our sample was 65.9 years old (CI95%: 65–67.9 years old). The incidence rate of DRF in our population was 158.5 fractures per 100,000 people-year; 49.2% were classified as type A of AO-OTA classification and 19% were treated surgically.
ConclusionIncidence of DRF had a maximum during males and women sixth decade of age. Type A fractures of AO-OTA classification were the most frequent. Most part of the fractures were treated non-surgically. The usual patient treated surgically was a woman, over 50 years old with a distal radius intraarticular complex fracture.
Las fracturas de la extremidad distal de radio (FEDR) representan una carga cada vez mayor para los recursos sanitarios debido a los cambios demográficos de la población y a las estrategias de gestión, por lo que la comprensión precisa de su epidemiología es esencial. Presentamos un estudio epidemiológico de FEDR y lo comparamos con otras áreas de la peninsula y Europa.
MétodoSe recogieron todas las FEDR de nuestra área sanitaria registradas en 2017 y 2018 en pacientes mayores de 18 años de forma retrospectiva y observacional agrupándolos según la clasificación de AO-OTA. Se analizaron las variables de edad, sexo, época del año, mecanismo de fractura, presencia de lesiones asociadas y tratamiento realizado.
ResultadosRegistramos 1.121 FEDR en 1.108 pacientes, 903 mujeres (81,5%) y 205 varones (18,5%). En 612 casos se vio afectado el lado izquierdo (54,6%) y en 509 el lado derecho (45,4%). La edad media de la muestra fue de 65,9 años (IC95%: 65–66,9 años). La tasa de incidencia de FEDR fue de 1585 fracturas por 100.000 habitantes/año. El 49,2% se clasificaron como tipo A de AO-OTA y se intervinieron quirúrgicamente un 19%.
ConclusiónLa incidencia de FEDR alcanza un máximo en la sexta década tanto en hombres como en mujeres. Las fracturas de tipo A de la clasificación AO-OTA son las más frecuentes. La mayoría se trataron de forma conservadora. El patrón de paciente tratado quirúrgicamente con más frecuencia es el de una mujer mayor de 50 años con FEDR articular compleja.
Fractures are an increasing burden on healthcare resources due to changing population demographics and management strategies. Therefore, an accurate understanding of their epidemiology is essential in allocating healthcare resources.1
Distal radius fracture (DRF) is one of the most common trauma injuries encountered in our daily clinical practice.2 It is also of particular interest, as it is known to be a valuable predictor for subsequent fractures in other locations such as the spine or hip, a phenomenon known as fracture cascade.1,3,4
There have been numerous epidemiological studies in various European cities,1,2,5–15 especially in the north of the continent. Studies have also been conducted in Spain,16,17 but there are none from the north-west area (Galicia), which has one of the peninsula’s most aged populations.
The aim of this study was to conduct an epidemiological study of DRF in the health area covered by our hospital complex (EOXI Vigo), and to compare our findings with those of other areas of the Iberian Peninsula and Europe.
Material and methodWe conducted a retrospective observational study, obtaining data on all patients diagnosed and treated for DRF in our hospital (a tertiary care centre covering a population of approximately 470,000 inhabitants, including both urban and rural areas) over a period of 2 years.
We collected initial data on all patients attending the Emergency Department of the Complejo Hospitalario Universitario de Vigo (CHUVI) with upper limb trauma pathology and seen by the centre’s Orthopaedic Surgery and Traumatology Service (OTS), after initial assessment by the emergency department, from 1 January 2017 to 31 December 2018.
All patients with suspected DRF underwent an anteroposterior (AP) and lateral (L) plain X-ray on arrival at the emergency department, which were the projections used for classification in this study. A computed tomography (CT) scan was requested for patients with complex or comminuted joint fractures for their final therapeutic decision.
Inclusion criteriaAll patients of legal age (>18 years) who were diagnosed with DRF (last 3 cm of the forearm bones before the radiocarpal joint), including polytrauma and pathological fractures.
Exclusion criteriaPatients who met the criteria but were not part of our health area were excluded.
Variables collectedAge at the time of the trauma, sex, laterality, mechanism of the trauma (high energy: if it occurred while undertaking recreational activities, in a traffic accident, or a fall from greater than standing height [2 m], or low energy: fall from standing height or less), season of the year in which the fracture occurred, type of fracture according to the Arbeitsgemeinschaft für Osteosynthesefragen -AO-OTA- classification (type A or extra-articular, type B or partial articular, and type C or complex articular),18 whether it was open or closed, presence of associated injuries (associated distal ulnar or ulnar styloid fracture, fractures of bones of the hand or fracture at another level, dislocations or associated ligament injuries, presence of other injuries), and type of treatment (conservative or surgical), specifying the technique used in the latter case.
Age was stratified by decade and five-year period. Due to the influence of osteoporosis in these fractures,1,3,4 and as in other multicentre studies, we made the cut-off point 50 years of age to divide into groups of young and older patients.
We calculated the incidence rate defined as the risk of developing a new condition during a specific time period. In this case, the risk of an individual developing a DRF within 1 year. The incidence rate was calculated as follows19:

The demographic data of the population studied (CHUVI health area) were collected from the 2017 and 2018 annual reports published by the Servicio Galego de Saúde (SERGAS).20
Data collection was performed by 5 resident interns specialising in orthopaedics and traumatology, and data analysis was performed by an independent observer (an orthopaedics and traumatology specialist).
The study was approved by the Hospital Ethics Committee following the guidelines for care quality assessment. The investigators conducted the study according to the principles of the Declaration of Helsinki. The study was conducted in accordance with the protocol and in compliance with the standards of good clinical practice as described in the standards of the International Council for Harmonisation (ICH) for good clinical practice.
Statistical analysisWe used SPSS v25 for the data analysis. Continuous variables were described by mean, standard deviation, and minimum and maximum values. Discrete variables were described by frequency distribution and percentages.
The bivariate analysis used the Student’s t-/Fisher test for continuous variables and the Chi-square test for categorical variables. Pearson's and Spearman’s correlation coefficients were used for the association between variables. Differences with a p < 0.05 were taken as significant.
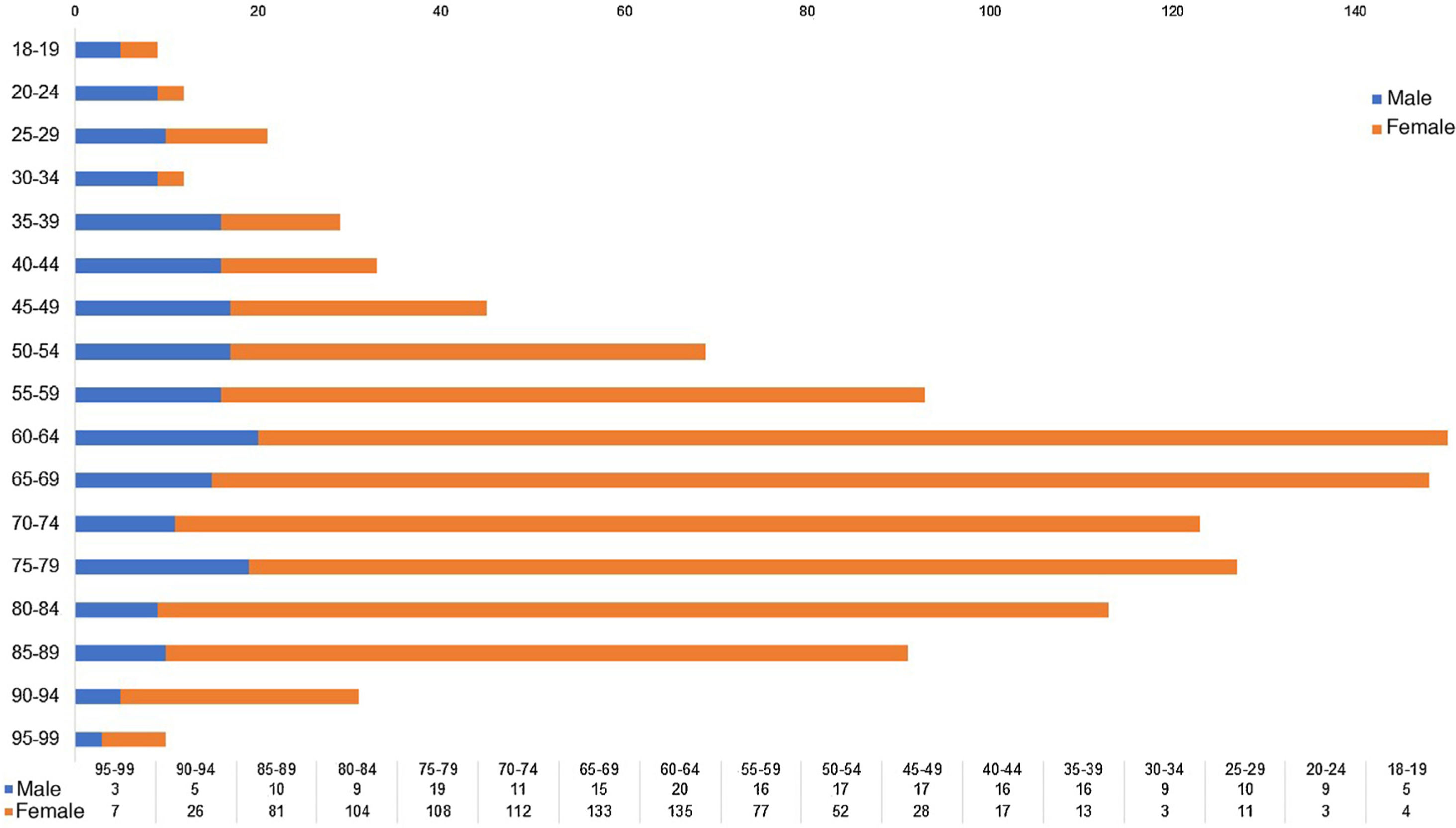
ResultsOur sample consisted of 1121 DRF in 1108 patients, 903 females (81.5%), and 205 males (18.5%). The left side was affected (54.6%) in 612 cases, and the right side in 509 cases (45.4%); these differences were not statistically significant (p = 0.6). The fracture was bilateral in 11 women and 2 men. The mean age of the sample was 65.9 years (95% confidence interval [95%CI]: 65–66.9 years); the minimum age being 18 years and the maximum age 99 years. The mean age was 68.2 years in the women (95% CI: 67.3–69.2 years) and 55.8 in the men (95% CI: 53.1–58.5 years); this difference was significant with a p < 0.00. In those under 50 years the female: male ratio was 1:1; however, in those over 50 years the ratio was 4:1. The distribution of DRF by age and sex is shown in Fig. 1.

Over the period studied, 7698 cases of locomotor system disease were recorded in the Emergency Department of the CHUVI requiring care and follow-up by the upper limb Traumatology Unit, and DRF (1108 patients) accounted for 14% of ED attendances for traumatic pathology of the upper limb, and 26% of fractures of this anatomical area (.9% of all ED attendances for any reason).
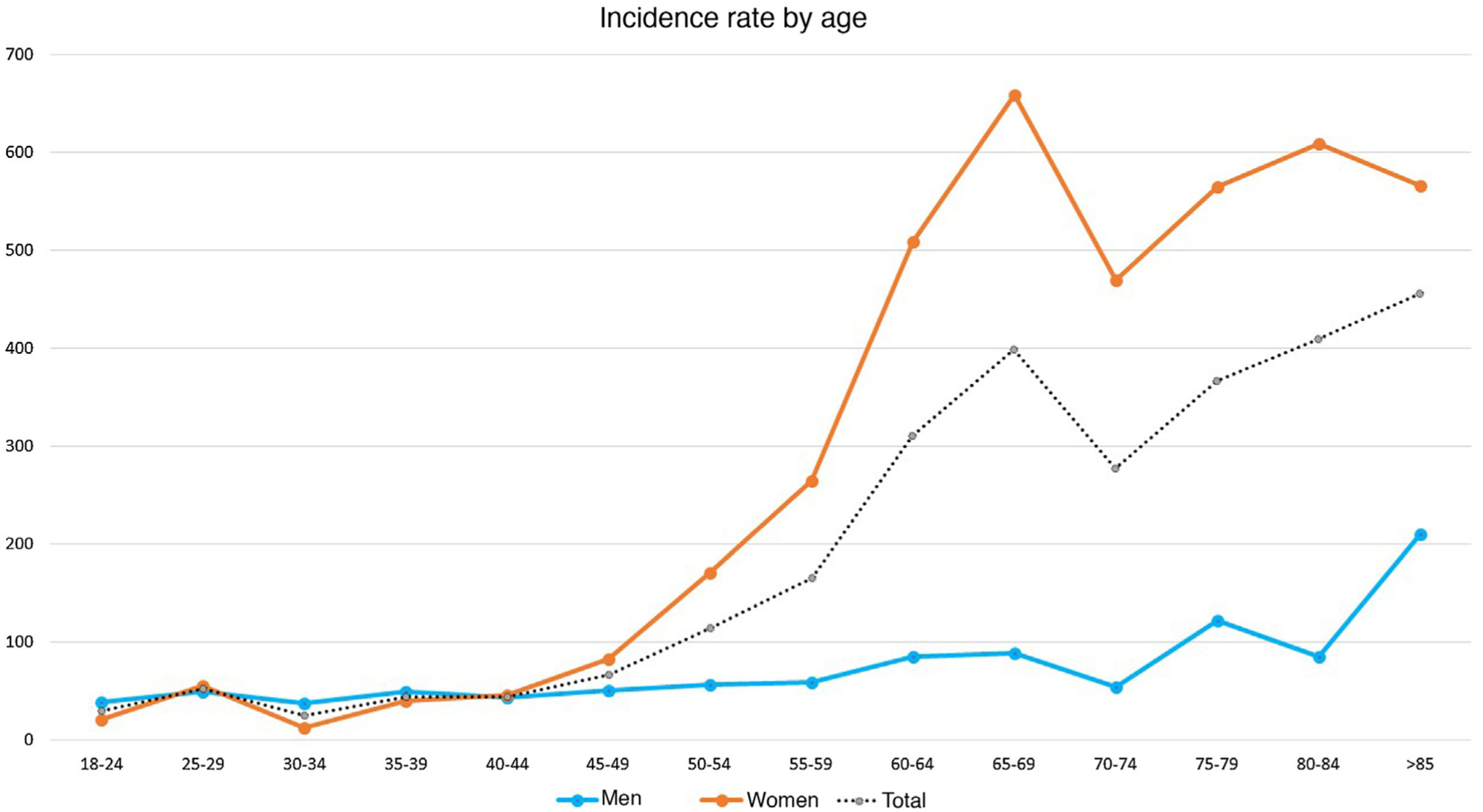
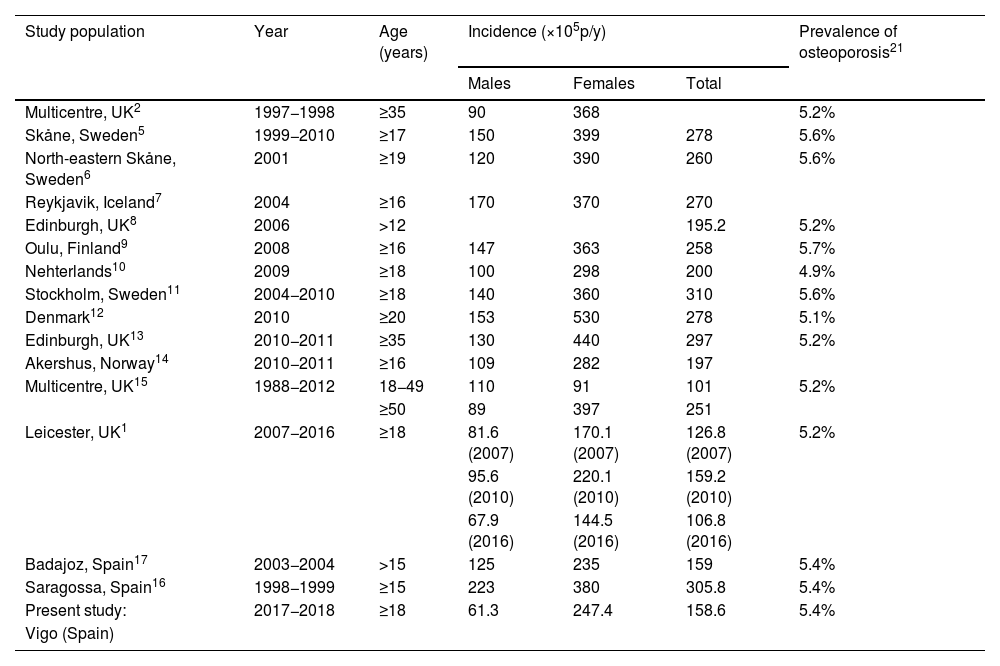
Over the period studied, the incidence rate of DRF was 158.5 fractures per 100,000 people/year (×105p/y). Segmented by sex, we obtained an incidence rate of 247.45 × 105p/y in women and 61.34 × 105p/y in men (Table 1). Fig. 2 shows the age-stratified incidence rate.
Incidence of DRF published in Europe.
| Study population | Year | Age (years) | Incidence (×105p/y) | Prevalence of osteoporosis21 | ||
|---|---|---|---|---|---|---|
| Males | Females | Total | ||||
| Multicentre, UK2 | 1997−1998 | ≥35 | 90 | 368 | 5.2% | |
| Skåne, Sweden5 | 1999−2010 | ≥17 | 150 | 399 | 278 | 5.6% |
| North-eastern Skåne, Sweden6 | 2001 | ≥19 | 120 | 390 | 260 | 5.6% |
| Reykjavik, Iceland7 | 2004 | ≥16 | 170 | 370 | 270 | |
| Edinburgh, UK8 | 2006 | >12 | 195.2 | 5.2% | ||
| Oulu, Finland9 | 2008 | ≥16 | 147 | 363 | 258 | 5.7% |
| Nehterlands10 | 2009 | ≥18 | 100 | 298 | 200 | 4.9% |
| Stockholm, Sweden11 | 2004−2010 | ≥18 | 140 | 360 | 310 | 5.6% |
| Denmark12 | 2010 | ≥20 | 153 | 530 | 278 | 5.1% |
| Edinburgh, UK13 | 2010−2011 | ≥35 | 130 | 440 | 297 | 5.2% |
| Akershus, Norway14 | 2010−2011 | ≥16 | 109 | 282 | 197 | |
| Multicentre, UK15 | 1988−2012 | 18−49 | 110 | 91 | 101 | 5.2% |
| ≥50 | 89 | 397 | 251 | |||
| Leicester, UK1 | 2007−2016 | ≥18 | 81.6 (2007) | 170.1 (2007) | 126.8 (2007) | 5.2% |
| 95.6 (2010) | 220.1 (2010) | 159.2 (2010) | ||||
| 67.9 (2016) | 144.5 (2016) | 106.8 (2016) | ||||
| Badajoz, Spain17 | 2003−2004 | >15 | 125 | 235 | 159 | 5.4% |
| Saragossa, Spain16 | 1998−1999 | ≥15 | 223 | 380 | 305.8 | 5.4% |
| Present study: | 2017−2018 | ≥18 | 61.3 | 247.4 | 158.6 | 5.4% |
| Vigo (Spain) | ||||||
DRF: Distal radius fractures; UK: United Kingdom.
 stratified by age (five years).")
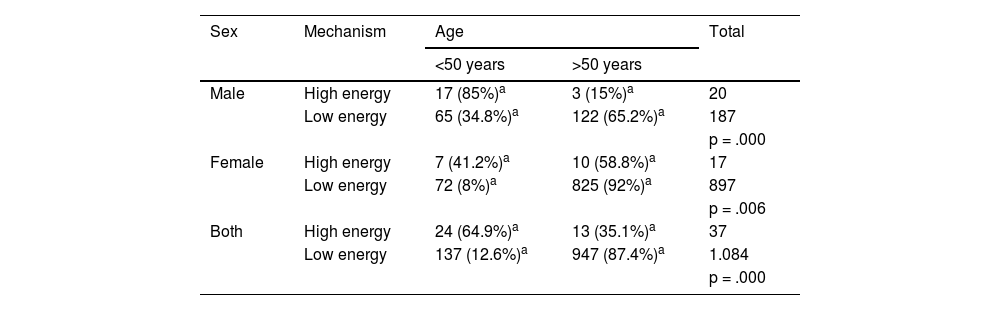
Only 37 DRF caused by a high-energy mechanism (3.3%) were identified, while the remainder were due to a low-energy mechanism (1084 DRF, 96.7%). The relationship between age and the mechanism of the DRF was analysed. Of the high-energy traumas (24), 64.9% occurred in patients younger than 50 years, although this accounted for only 14.9% of the DRF occurring in this age range (Table 2). These results were statistically significant (p < 0.001).
DRF mechanism of injury (high or low energy) divided by age (over or under 50 years of age) and by sex.
| Sex | Mechanism | Age | Total | |
|---|---|---|---|---|
| <50 years | >50 years | |||
| Male | High energy | 17 (85%)a | 3 (15%)a | 20 |
| Low energy | 65 (34.8%)a | 122 (65.2%)a | 187 | |
| p = .000 | ||||
| Female | High energy | 7 (41.2%)a | 10 (58.8%)a | 17 |
| Low energy | 72 (8%)a | 825 (92%)a | 897 | |
| p = .006 | ||||
| Both | High energy | 24 (64.9%)a | 13 (35.1%)a | 37 |
| Low energy | 137 (12.6%)a | 947 (87.4%)a | 1.084 | |
| p = .000 | ||||
DRF: Distal radius fractures.
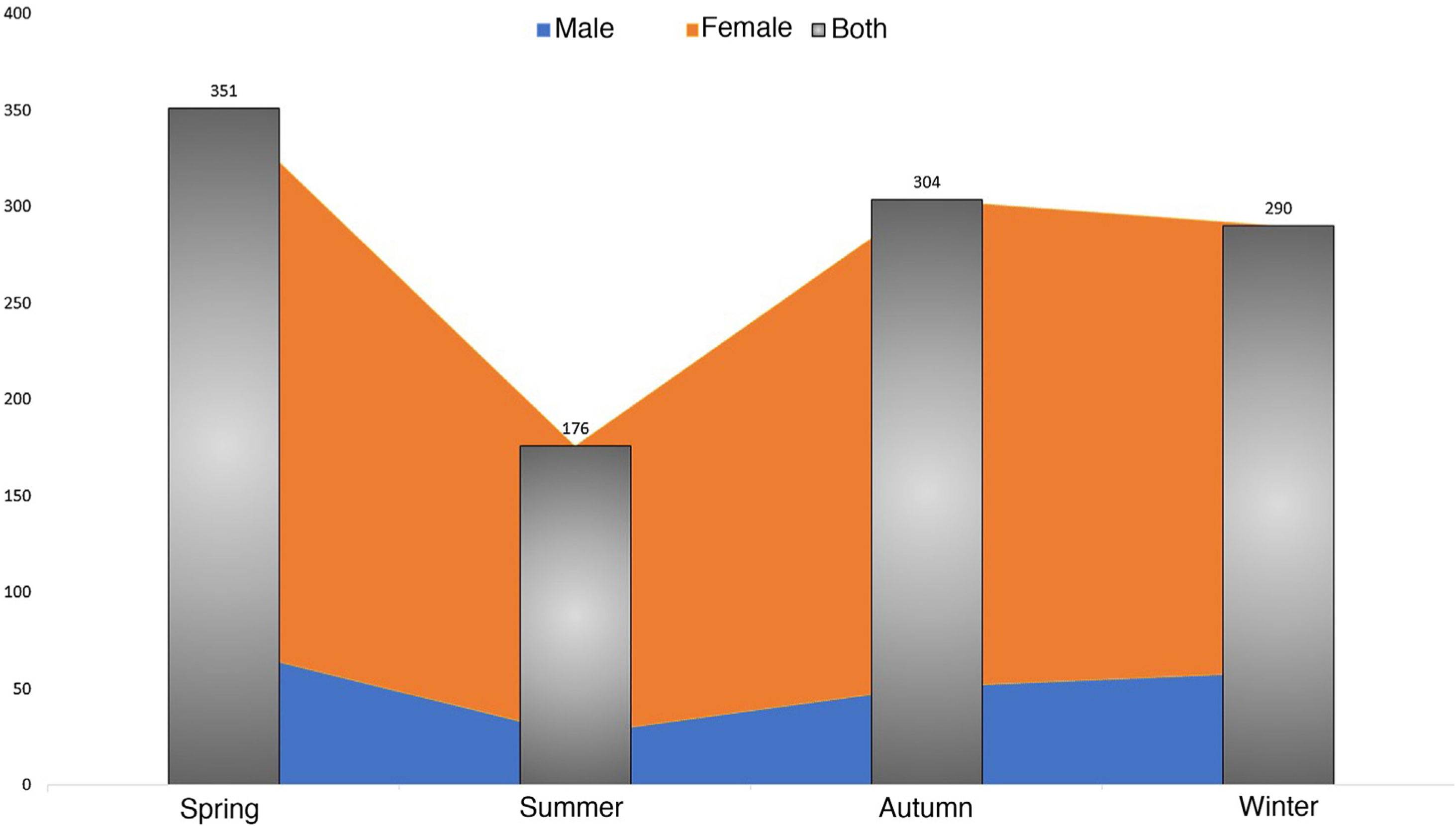
Regarding the relationship between the seasons of the year and the presence of DRF, we recorded 351 fractures in the winter period, 176 in spring, 304 in summer and 289 in autumn; these differences were statistically significant (p < 0.001) (Fig. 3).

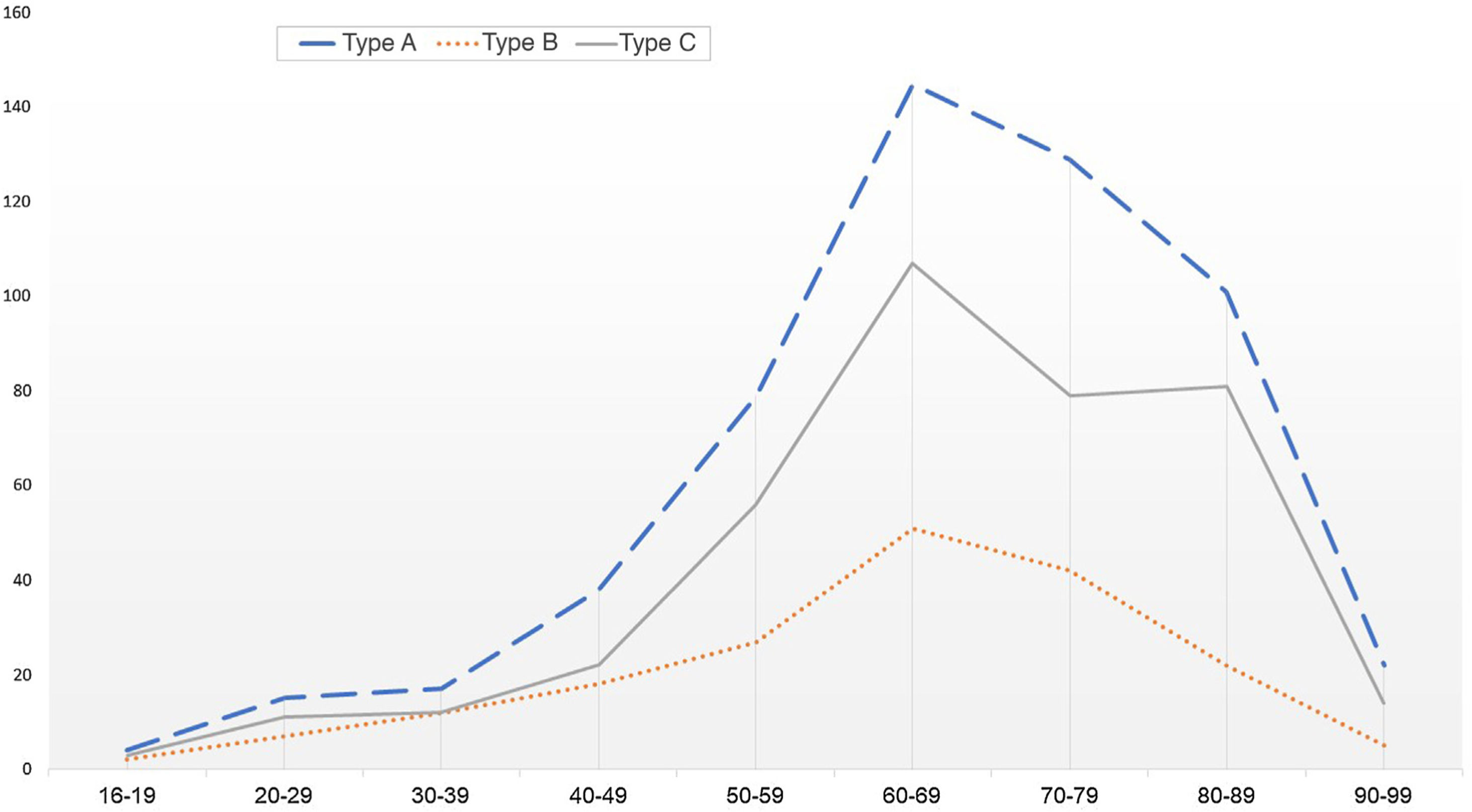
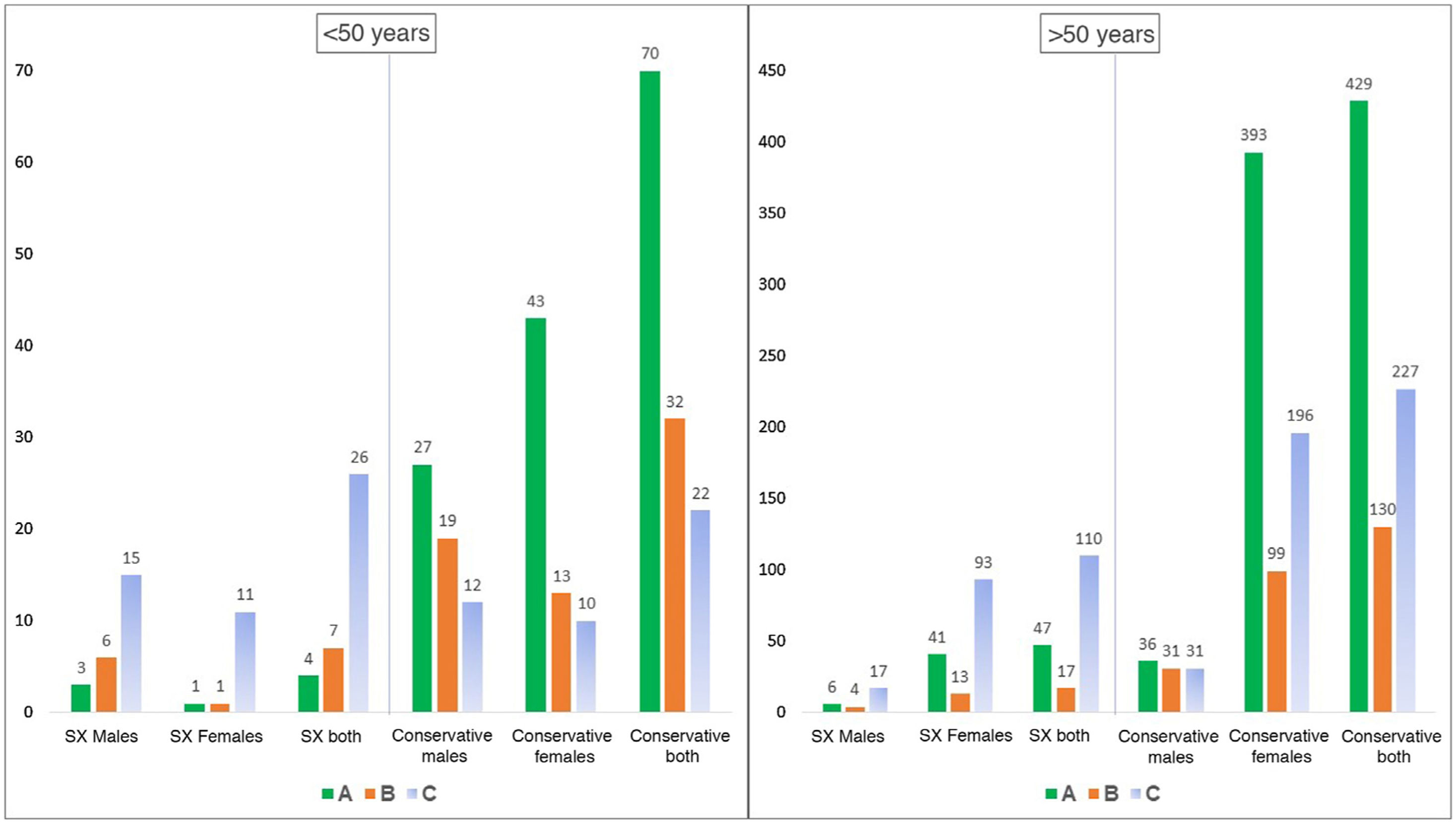
According to the AO-OTA18 classification, we attended 551 DRF classified as type A (49.2%), 185 type B (16.5%), and 384 type C (34.3%) (Fig. 4). In addition, using the age cut-off of 50 years, we obtained statistically significant differences in the groups according to age (p = 0.018). When relating the mechanism of injury to the type of fracture according to the AO-OTA classification,18 we obtained variations in the frequency of DRF. Type A fractures continue to be the most frequent fractures produced by low-energy mechanisms, followed by type C fractures. However, type C fractures were the most frequent (p < 0.05) DRF caused by a high-energy mechanism.
. DRF: distal radius fractures.")
Distribution of DRF according to AO-OTA classification18 stratified by age (decades). DRF: distal radius fractures.
Only 2 open DRF out of 1121 occurred in 2 women over the age of 50 years. Both were by low-energy mechanisms.
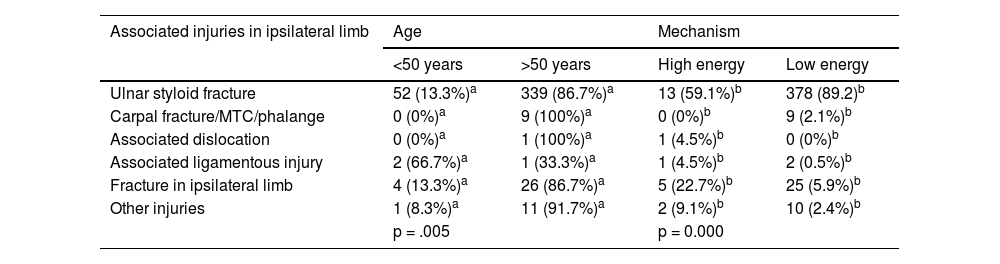
We collected the presence of injuries associated with DRF that occurred in the ipsilateral upper limb. When we analysed whether there was a relationship between the complexity of the fracture and presence of a fracture of the ulnar styloid or distal third of the ulna, we found that, according to the AO-OTA classification,18 33.1% of type A DRF had an associated ulnar fracture, in those of type B 18.3%, and in those of type C 44.8% (p < 0.01). We also looked for a relationship between the presence of associated lesions and age. We found 36.6% of lesions associated with DRF in patients under 50 years of age, whereas this was 40.6% in those over 50 years. These differences were not statistically significant (p = 0.1). Regarding the fracture mechanism and the presence of associated injuries, we found that 54% of cases of DRF with associated injuries were produced by a high-energy mechanism, while in low-energy cases there were 34.1% associated injuries. These results were statistically significant (p < 0.001) (Table 3).
Presence of associated injuries stratified by age and mechanism of injury.
| Associated injuries in ipsilateral limb | Age | Mechanism | ||
|---|---|---|---|---|
| <50 years | >50 years | High energy | Low energy | |
| Ulnar styloid fracture | 52 (13.3%)a | 339 (86.7%)a | 13 (59.1%)b | 378 (89.2)b |
| Carpal fracture/MTC/phalange | 0 (0%)a | 9 (100%)a | 0 (0%)b | 9 (2.1%)b |
| Associated dislocation | 0 (0%)a | 1 (100%)a | 1 (4.5%)b | 0 (0%)b |
| Associated ligamentous injury | 2 (66.7%)a | 1 (33.3%)a | 1 (4.5%)b | 2 (0.5%)b |
| Fracture in ipsilateral limb | 4 (13.3%)a | 26 (86.7%)a | 5 (22.7%)b | 25 (5.9%)b |
| Other injuries | 1 (8.3%)a | 11 (91.7%)a | 2 (9.1%)b | 10 (2.4%)b |
| p = .005 | p = 0.000 | |||
Nineteen per cent of DRF (211 cases) were treated surgically compared to 81% (910 cases) that were treated conservatively with immobilisation in an antebrachial cast. Stratified by age, we observed that patients under 50 years received 5% more surgical treatment than those over 50 years, although these data were not statistically significant (p = 0.02) (Fig. 5).
 and type of DRF according to the AO-OTA classification.18 DRF: distal radius fractures; SX: surgical intervention.")
Type of treatment given, stratified by sex, age (over or under 50 years of age) and type of DRF according to the AO-OTA classification.18 DRF: distal radius fractures; SX: surgical intervention.
We studied whether there was a greater tendency in our population for surgical treatment was associated with patients with associated lesions. We found that 35.2% of conservatively treated DRF patients had an associated lesion (434 cases), while 54% of surgically treated patients had an associated lesion (114 cases). In the surgical group, 78.1% had an associated ulnar styloid fracture (93 cases), 0.8% had another fracture in the hand (1 case), 0.5% had an associated dislocation (1 case), 1.7% a ligamentous injury (2 cases), and 14.4% a fracture at another level in the same extremity (17 cases). These data were statistically significant (p < 0.001).
The most used osteosynthesis material was the variable angle volar plate (87.7% total [185 cases]). No statistically significant association was found between the use of osteosynthesis material and the type of DRF according to the AO-OTA classification (p = 0.2).18
DiscussionIn line with that published in the literature,4 we found that DRF is the most frequent upper limb fracture in our setting. The most significant aspect of this study is that the incidence rate (158.6 × 105p/y) is much lower than that published in other northern European countries1,2,5–15 (Table 1). Although DRF is considered an osteoporotic fracture, these findings could not be explained simply by the higher prevalence of osteoporosis in these areas. According to the report published by Hernlund et al.21 in 2013, the prevalence of osteoporosis in northern Europe varied from 4.9% to 5.6%, while in Spain it was estimated at 5.4%. It is important to note that our health area enjoys an oceanic climate, unlike the Nordic countries, and there is no snowfall or temperatures below 0 °C.
In Spain, we found 2 only epidemiological studies on DRF published since 2000 that include the entire adult population (over 15 years of age).16,17 Our overall incidence rate is also much lower than that published in Saragossa by Cuenca et al.16 (305.8 × 105 p/y) although similar to that published by Luque et al. in Badajoz in 201017 (159 × 105 p/y). In 2006, a Spanish multicentre study was published on non-vertebral fragility fractures in women aged 65 years and over22 in which they reported an incidence rate of 580 distal radius fractures per 100,000 women ≥65 years/year, a figure similar to that obtained in our study if we only include women in that age range who suffered a low energy mechanism (563 × 105 women > 65 years/year). However, we obtained an incidence rate one third lower than that published by Naves et al.23 within the EVO osteoporosis study where DRF were recorded in women aged 50 years and over, although this study was published in 2003.
If we analyse this incidence rate according to age divided by decades, we observe in both sexes a proportional increase with age, which is exponential in women from the fourth decade onwards. This finding is a constant in published epidemiological studies. However, there are studies in which the incidence rate stabilises from the sixth decade onwards,1 while others2,8,11,12 show a continuous increase with age. In our study, the incidence rate stabilises from the sixth decade until the eighth decade, when it again increases. It should be noted that, due to the demographic data available to us, the population over 80 years of age was grouped together and that includes two decades, and therefore this increase may not be real. In the men there was also an increase in the incidence rate with age, although more linear and later than in the women, around the sixth decade (Fig. 2). This reflects the later onset of osteoporosis in men.1,8,12
This fracture has been described as having a bimodal distribution,1,10,24,25 with a peak in young men secondary to high energy trauma, and another in older women with underlying osteoporosis.1 Like Cuenca et al.,16 we did not find this bimodal distribution in our study, but rather a maximum peak in the 60−69 year age group (27%) in both men and women, the most frequent age being 60 years (1.3%); however, we did not include patients under 18 years and this may affect this bimodal distribution.10,24
The distribution by sex in those under 50 years was 1:1 (79 women: 82 men), although in this age group 70% of high-energy trauma occurred in males (Table 2). This ratio increases to 4F:1M in those aged over 50 years, with 74.5% of the sample being women over 50 years, which can be attributed to the impact of osteoporosis.26
As in other studies,1,9,24 we observed variations in the incidence of DRF according to season. In our study more DRF were recorded in the winter period, in contrast to the study by Luque et al.17 where they recorded a greater number of fractures in summer. Reduced levels of light have been published as possible causes of this higher incidence in the winter months, with the consequent increase in the risk for falls in individuals with poor eyesight and reduced synthesis of vitamin D, which can lead to osteoporosis.1,24 In our health area there is a lot of rainfall and high humidity during the winter months, which may explain the greater likelihood of falls on slippery surfaces, especially in the elderly population with poorer balance and reaction speed.
Several authors8,12,16,17,26–28 have used the AO-OTA system to classify the DRF in their epidemiological studies.18 Our findings are similar to these publications, and extra-articular fractures (type A of AO-OTA) are the most frequent in our sample, either analysing the population as a whole or dividing it by decades. As in these studies, among the articular fractures, type C fractures are more frequent than type B fractures. We observe that, as the age range increases, the percentage of complex intra-articular DRF increases (Fig. 4). Women over the age of 50 years accounted for 85.7% of patients with complex joint fractures and women over the age of 70 years accounted for 40%. Clayton et al.29 reported the relationship between osteoporosis and the severity of fractures of the distal radius. In our study, although more than half of the DRF produced by a high-energy mechanism were classified as AO-OTA type C, only 5% of type C fractures were caused by a high-energy mechanism. This, together with the high percentage of these fractures in older women, is in line with that described by Clayton et al.29
We found a very small proportion of open fractures (.18%), much lower than that published recently in the Swedish registry (1.2%).24 This implies that this type of injury is difficult to incur in this anatomical region, probably due to the mechanism of injury (generally indirect trauma through hyperextension and fall from standing height).
As in the paper by Koo et al.,28 we found a low percentage of other associated injuries in the ipsilateral arm (41 fractures at another level, 2 carpometacarpal dislocations, and 3 tendon ruptures). Of the associated injuries, 77% occurred in women over 50 years of age; we found a statistically significant association between the presence of these injuries and female sex (p = 0.03), but not in males (p = 0.1) in this age range. We did not find this relationship in the papers published in the literature that we reviewed; it could be explained by the high prevalence of osteoporosis in this population group after the menopause.
The treatment of DRF has changed over the last few decades, and the number of surgical interventions has increased,30 which does not seem to be related to the relative increase in the incidence of the injury.26 In Sweden, the rate of surgical treatment increased from 16% of fractures in 2005 to 20% in 2010 and 26% in 2020.24 According to Porrino et al.,26 this trend may be related to increased follow-up of these fractures by hand surgeons rather than orthopaedic surgeons, as is the case in our centre. In this study, most DRF were treated conservatively (81%) although, logically, the more complex fractures were more likely to be treated surgically (63.7% of operated fractures). These data coincide with the Spanish multicentre study published in 2013 by Oteo et al.,27 in which they report that 75% of DRF were treated conservatively. It also coincides with that published in the literature, except for the work of Koo et al.,28 where 61% of patients with a DRF were treated surgically. There was a predisposition for conservative treatment in patients over 50 years of age; however, the pattern of surgically treated patients corresponded to that of women over 50 years of age with type C fracture of AO-OTA (44%).
In our study, following the current trend, the most used surgical technique was the fixed-angle volar plate, both in extra-articular fractures and in simple and complex articular fractures. The reason for this type of treatment is primarily down to the organisational system of our hospital, as we usually delay surgery until 7–10 days after the patient's arrival at the Emergency Department.
This study has some limitations. Its retrospective nature is a limitation, as is the fact that the fractures were classified by 5 orthopaedic surgeons in training. Therefore, to minimise this inter-observer variability, only the 3 main types (A, B, C) of DRF were classified.18 The strengths of the study are that it was limited to the registry of a hospital that receives all the emergencies in the health area described, to which the entire population has access, given Spain’s system of comprehensive public health coverage. Logically, DRF may have been lost in patients who suffered an accident at work, as it is possible that they attended a health centre that has an agreement with their employer's health insurance company. Another strength is that we were able to collect all the DRF that occurred in our health area, whether they were treated as inpatients or outpatients, conservatively or surgically. We believe, therefore, that we have selected a sample representative of our region for the epidemiological analysis of this pathology.
We can conclude that DRF in our health area occur in all age groups, reaching a maximum in the sixth decade in both men and women. Type A fractures of the AO-OTA18 classification are the most common, whereas type B fractures are the least common. The mechanism of injury correlates with the AO-OTA classification, and this classification, in turn, is associated with the percentage of fractures fixed surgically. Most are treated conservatively, however, the most common pattern of surgically treated patients are women over the age of 50 with complex joint fractures. Ulnar styloid fractures are common and should be looked for especially in older women.
Level of evidenceLevel of evidence III.
Conflict of interestsThe authors have no conflict of interests to declare.
FundingThe authors declare that they have received no funding for the conduct of the present research, the preparation of the article, or its publication.
Please cite this article as: Zugasti-Marquínez J, García-Reza A, Domínguez-Prado DM, Cela-López M, Oiartzábal-Alberdi I, Castro-Menéndez M. Estudio epidemiológico de las fracturas de la extremidad distal de radio en el área sanitaria de Vigo. Rev Esp Cir Ortop Traumatol. 2022;66:37–45.
