



To evaluate the clinical, radiological and histological factors that can predict local recurrence of fibromatosis.
MethodsA retrospective study was conducted on 51 patients diagnosed with fibromatosis in this hospital from 1983 to 2014. The mean follow-up was 83 months. A study was made of the clinical parameters, location, depth, size, surgical margins, and proliferation index (Ki-67). An evaluation was also made of the risk of recurrence depending on the adjuvant treatment and the relationship between treatment and patient functionality.
ResultsTumour location and depth were identified as risk factors for local recurrence, showing statistically significant differences (P<.001 and P=.003, respectively). There were no statistically significant differences in age, gender, size, surgical margins, or adjuvant treatments, or in the Musculoskeletal Tumour Society Score according to the treatment received. The mean Ki-67 was 1.9% (range 1–4), and its value was not associated with the risk of recurrence.
DiscussionDeep fibromatosis fascia tumours, and those located in extremities are more aggressive than superficial tumours and those located in trunk. The Ki-67 has no predictive value in local recurrence of fibromatosis. Radiotherapy, chemotherapy, or other adjuvant treatments such as tamoxifen have not been effective in local control of the disease. Given the high recurrence rate, even with adequate margins, a wait and see attitude should be considered in asymptomatic patients and/or stable disease.
Valorar los factores clínicos, radiológicos e histológicos que pueden predecir la recidiva local de fibromatosis.
MétodosHemos realizado un estudio retrospectivo de 51 pacientes con diagnóstico de fibromatosis en nuestra institución desde 1983 hasta 2014. La media de seguimiento es de 83 meses. Hemos estudiado parámetros clínicos, localización, profundidad, tamaño, márgenes quirúrgicos e índice de proliferación (Ki-67) del tumor. Asimismo, hemos valorado el riesgo de recidiva en función del tratamiento adyuvante y la relación del tratamiento con la funcionalidad del paciente.
ResultadosHemos observado diferencias estadísticamente significativas en cuanto a la profundidad (p=0,003) y la localización (p<0,001) como factores de riesgo de recidiva local. No existen diferencias estadísticamente significativas en cuanto a edad, sexo, tamaño, márgenes quirúrgicos ni tratamientos adyuvantes, ni en el Musculoskeletal Tumor Society Score en función del tratamiento recibido. El Ki-67 tiene una media de 1,9% (rango 1-4) y su valor no se asocia con el riesgo de recidiva.
DiscusiónLos tumores profundos a la fascia y los localizados en extremidades son más agresivos que los localizados superficialmente y en el tronco. El Ki-67 no tiene valor predictivo en las recidivas de la fibromatosis. La radioterapia, la quimioterapia u otros tratamientos adyuvantes como el tamoxifeno no han sido eficaces en el control local de la enfermedad. La gran cantidad de recidivas, incluso en pacientes con resecciones adecuadas, induce a plantear la posibilidad de una actitud expectante en tumores asintomáticos o en enfermedad estable.
Fibromatosis, or desmoid tumour, is a clonal proliferation tumour deriving from mesenchymal cells seated in the fascia and musculoaponeurotic structures. It constitutes a rare group of soft tissue tumours, with an incidence of 2.4–4.3 new cases per 106 inhabitants/year.1–3
For many years, this tumour was treated by surgery fundamentally, reserving chemotherapy, radiotherapy and other systemic treatments such as tamoxifen or more recently, imatinib or toremifine,2,4 for cases with positive surgical margins to improve local control of the disease.1
It can appear in practically any part of the body5,6 and is locally aggressive, with a high local recurrence rate, despite broad surgical resection, although it lacks the capacity for remote metastasis.2
Conservative management has been proposed recently as an acceptable treatment option, since it is not unusual for the tumour to stop growing spontaneously. This would prevent functional complications and post-radiation effects associated with the conventional, radical management of fibromatosis.1
Because this is a rare entity, the series available in the literature enable us to establish a consensus on some of the factors that influence the natural evolution of the disease. It is our intention to evaluate the data that might predict local recurrence.
MethodsWe undertook a retrospective study identifying 192 patients with an anatomopathological diagnosis of fibromatosis in our institution from 1983 to 2014. Patients with a clinical diagnosis of Dupuytren's, Ledderhose disease or intra-abdominal desmoid tumour were excluded from the study, because their prognosis is more favourable, and patients with an unclear final diagnosis.
The following variables were gathered from the patients included in the study: age at the time of diagnosis, gender, imaging test type used in diagnosis, location, tumour size and depth, relation to the vascular bundle, initial treatment given, primary tumour resection margins, recurrences, time until recurrence, treatment and surgical margins, and finally, follow-up time and the patients’ current condition and functional status according to the Musculoskeletal Tumour Society Score. Due to the wide range of years over which our patients were diagnosed, we also gathered the variations in the type of treatment through that time.
All our cases were identified initially as primary or recurrences as they presented in our centre. However, this difference was not taken into account in the statistical analysis for classifying the primary tumours or recurrences, or the subsequent determination of risk factors.
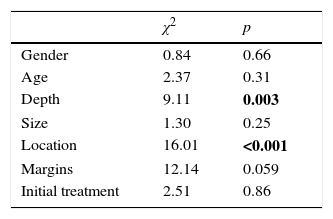
The statistical analysis was then undertaken using the χ2 test to assess the influence of patient gender, age, depth, size, location, surgical margins and initial treatment on local recurrences.
For this analysis, in terms of age, the patients aged ≤30 years were classified as “young” and those aged >30 years as “older”. Tumours that measured <5cm were classified as “small” and those that measured ≥5cm as “large”, in the same way as soft-tissue sarcomas. Finally, the tumour location was divided into 2 large groups: extremities and trunk, the latter included neck, breast, chest wall, abdominal wall and paravertebrals.
The initial treatment of our patients was evaluated. Most underwent surgery as single therapy. Some cases received adjuvant treatment as well as surgery, such as radiotherapy, chemotherapy and tamoxifen.
The resection margins were classified according to Enneking's criteria. In addition, a revision of the histological preparations was made to quantify the Ki-67 of the histological blocks from 1992 onwards.
ResultsOur series includes 51 patients with a clinical and anatomopathological diagnosis of fibromatosis. Twenty-nine of these patients were treated primarily in our centre, and 22 presented as recurrences.
The mean follow-up was 83 months (range 6–240 months).
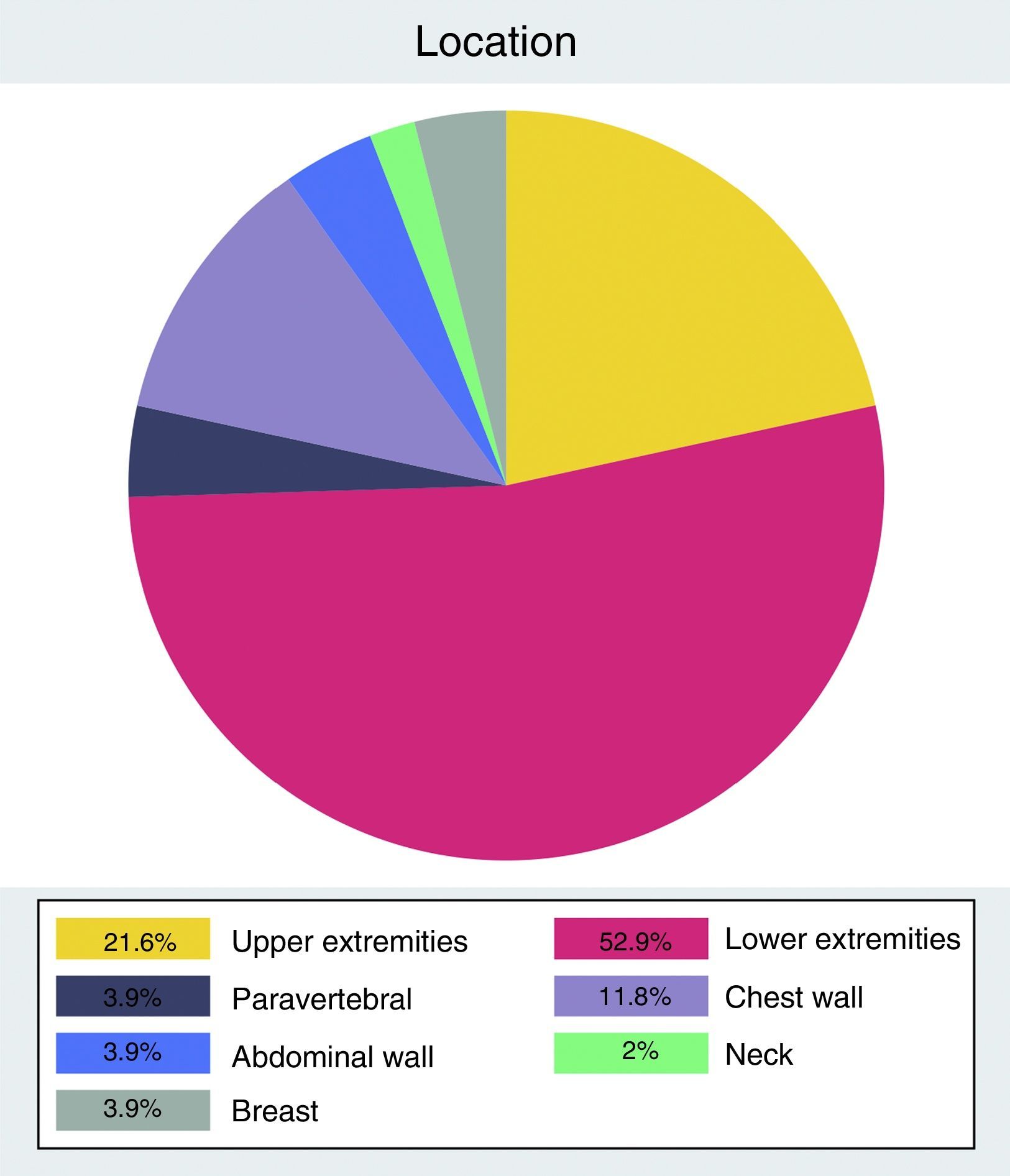
The most common anatomical distribution was tumours located in the extremities (n=38) compared to the trunk (n=13) (Fig. 1).

The mean age at time of diagnosis was 26 years, with a range from 2 to 68 years. Distribution by gender showed a slight male predominance, unlike the other published series.
The mean size, measured as the maximum tumour diameter, was 9.9cm (range 3–31cm). Most of the tumours were found deep in the fascia. The imaging test used to study the tumours was initially ultrasound. From 1990 onwards, diagnosis was made by magnetic resonance.
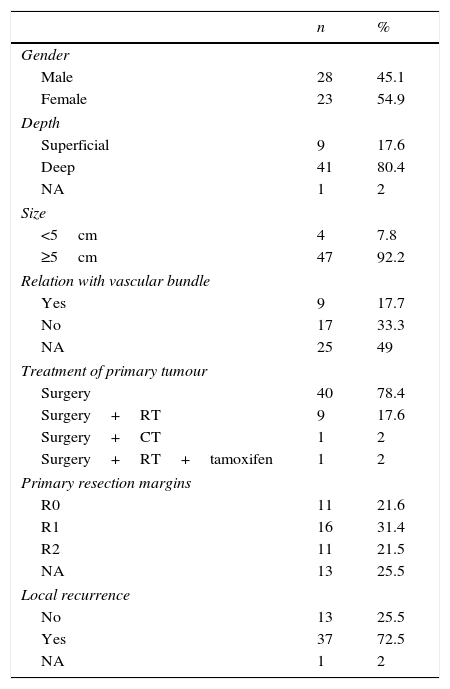
A complete macroscopic and microscopic (R0) resection was achieved in 11 patients. The margins were microscopically positive (R1) in 16 patients, and in 11 cases, the resection was intentionally incomplete on entry (R2) due, principally, to the great morbidity resulting from radical surgery in certain locations such as the popliteal fossa, groin and axilla. We have no information on the outcomes of the resection margins of the primary tumour for 13 patients (Table 1).
Characteristics of the patients with fibromatosis and of the primary tumour.
| n | % | |
|---|---|---|
| Gender | ||
| Male | 28 | 45.1 |
| Female | 23 | 54.9 |
| Depth | ||
| Superficial | 9 | 17.6 |
| Deep | 41 | 80.4 |
| NA | 1 | 2 |
| Size | ||
| <5cm | 4 | 7.8 |
| ≥5cm | 47 | 92.2 |
| Relation with vascular bundle | ||
| Yes | 9 | 17.7 |
| No | 17 | 33.3 |
| NA | 25 | 49 |
| Treatment of primary tumour | ||
| Surgery | 40 | 78.4 |
| Surgery+RT | 9 | 17.6 |
| Surgery+CT | 1 | 2 |
| Surgery+RT+tamoxifen | 1 | 2 |
| Primary resection margins | ||
| R0 | 11 | 21.6 |
| R1 | 16 | 31.4 |
| R2 | 11 | 21.5 |
| NA | 13 | 25.5 |
| Local recurrence | ||
| No | 13 | 25.5 |
| Yes | 37 | 72.5 |
| NA | 1 | 2 |
NA: not available; CT: chemotherapy; RT: radiotherapy.
In our patients, the proliferation rate, quantified using Ki-67, was a mean 1.9% (range 1–4).
The total number of recurrences in our series was 37, including incident cases (n=15) plus those that presented as recurrences in our institution (n=22). Out of these, 22 presented new recurrences (n=7 and n=15, respectively). The incidence of “re-recurrence” was less in the cases treated primarily in our centre (46.7% vs 68.2%), although this difference is not statistically significant (p=0.443). Neither are there statistically significant differences in re-recurrences according to the treatment of the first recurrence (p=0.112).
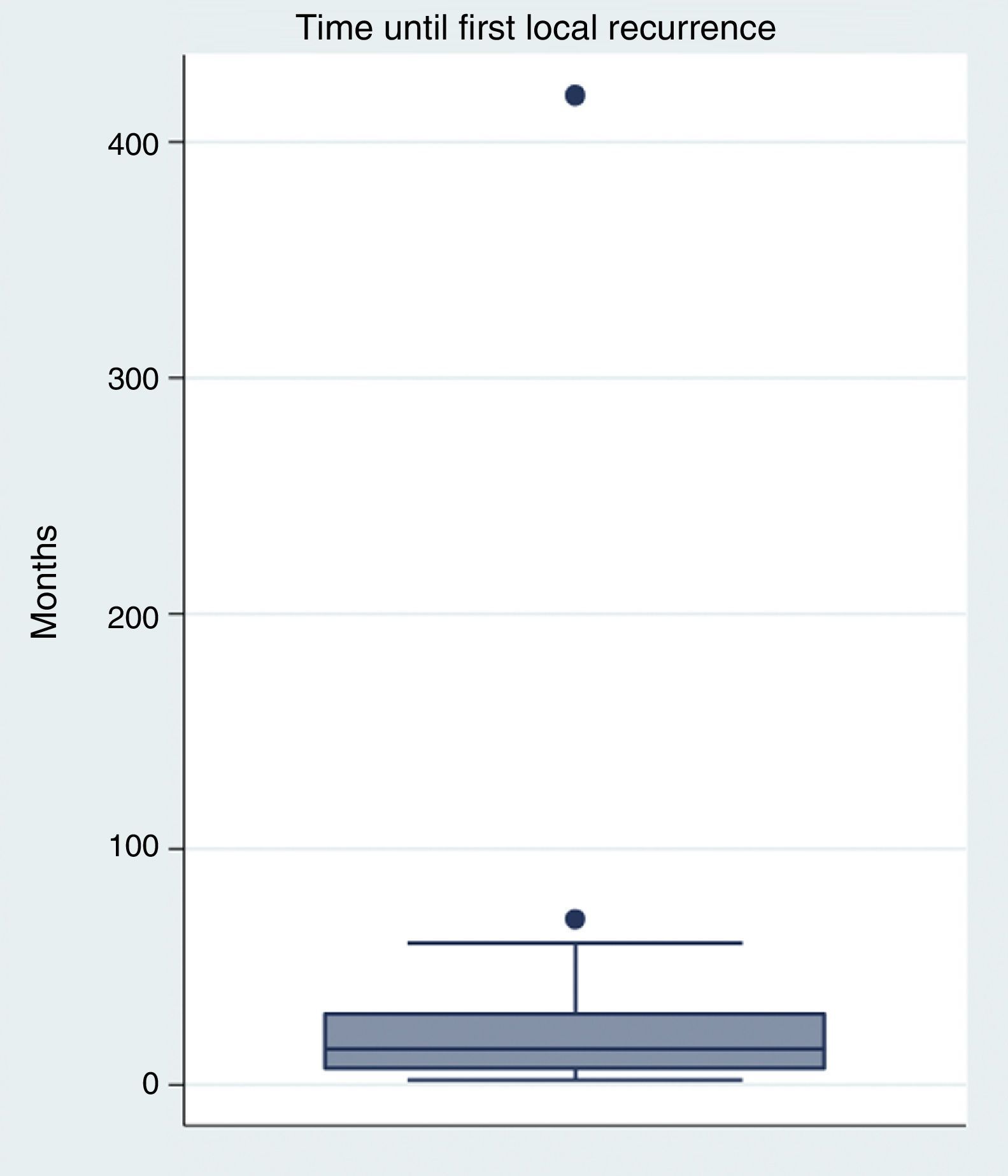
The mean time between the primary resection and the first recurrence was 32 month (range 2–420 months), although recurrence within the first year (Fig. 2) was most frequent. The mean time until repeat recurrence is similar to that of the first (mean 22.56, range 2–42).

Due to the limited number of cases treated with adjuvant therapies, no clear pattern for choosing this treatment was established. However, we did observe a variation over the years in terms of the type of radiotherapy. Up until 1999, patients who underwent radiotherapy received intraoperative radiotherapy complemented later with external radiotherapy, whereas from 1999 onwards brachytherapy plus external radiotherapy was used. In both groups, the mean dose received was 45Gy, and in no case did this exceed 60Gy.
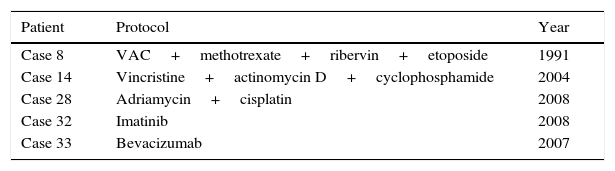
We saw no homogeneity in terms of chemotherapy protocol either (Table 2).
Protocols of chemotherapy administered.
| Patient | Protocol | Year |
|---|---|---|
| Case 8 | VAC+methotrexate+ribervin+etoposide | 1991 |
| Case 14 | Vincristine+actinomycin D+cyclophosphamide | 2004 |
| Case 28 | Adriamycin+cisplatin | 2008 |
| Case 32 | Imatinib | 2008 |
| Case 33 | Bevacizumab | 2007 |
VAC: vincristine+doxorubicin+cyclophosphamide.
Twenty-seven patients are currently disease-free, 8 are in the progression phase, 15 are in stable disease phase, and for one patient we have no information.
We observed no statistically significant differences in our series with regard to gender, age, size, margins or initial treatment as risk factors for local recurrence. By contrast, we did observe a greater risk of local recurrence in patients presenting tumours deep in the fascia (p=0.003) and tumours located in the extremities (p<0.0001) (Table 3).
The Musculoskeletal Tumour Society Score showed no statistically significant differences either (p=0.19) between the patients treated with surgery alone compared to those treated with surgery plus radiotherapy and those who underwent follow-up with periodic monitoring. Other complications after surgery included lymphoedema (n=2) and paralysis of the peroneal nerve (n=1).
DiscussionIn most current studies, positive surgical margins are considered a risk factor of local recurrence; however, there is no universal consensus on the matter.3,6–8 In our case, we found no statistically significant differences in this parameter.
Although there is no unanimity in this regard, the negative effect of incomplete surgery with positive margins (R1, R2) on local recurrence of the disease has a strong biological basis.9 Up to 75% of desmoid tumours present mutations associated with β-catenin. Most are sporadic, although a small percentage is associated with APC gene mutations, in Gardner syndrome.1,10,11
In the initial phase of wound healing, growth factors are released that activate β-catenin. This protein plays an important role in healing, since it stimulates the proliferation of fibroblasts, and therefore is also important in fibroproliferative disorders. Incomplete resection of a tumour involves leaving genetically altered cells in the bed exposed to the healing mechanisms of the tissues. Thus, surgery itself acts as a cancer potentiator in cases where there is a beta-catenin aberration.
Various mutations have been identified in the CTNNB1 gene, responsible for coding β-catenin. The mutations of this gene that are associated with fibromatosis are T41A, S45F and 45P, but S45F is the only one of prognostic value as a predictor of local recurrence.12 These variations in β-catenin mutations can in part explain the differences in the development of recurrences in relation to surgical margins.1,8,12
As we have seen to date, the evolution of this tumour is unpredictable, up to a certain point. In many cases, there is a high tendency for local recurrence despite apparently complete resection. Furthermore, some studies support the fact that adjuvant therapies can be effective in controlling the disease. However, there is no consensus in this regard, since there are desmoid tumours that have been observed to stop growing spontaneously.3,7,13,14 It does appear clear that as we increase therapeutic measures, in addition to increasing monitoring of the disease, we enhance the functional consequences, those of radical surgery and radiotherapy in particular.13,14
We must remember, in our series, that treatment by periodic monitoring only took place in patients who had already developed local recurrence, therefore we do not know what would have happened if we had not operated the primary tumours.
In high grade tumours, when we observe multiple recurrences, the disease-free time between each recurrence progressively shortens. In desmoid tumours, recurrences do not follow this pattern. As we saw in our series, the recurrences, both primary and secondary, occurred most frequently during the first year, without the disease-free time between the first and the second recurrence being significantly shortened.
Due to the lack of evidence in our series on the efficacy of the various treatments on local control of the disease, we cannot actively recommend the use of radiotherapy, chemotherapy or tamoxifen as adjuvant treatment.
It was observed that in selected cases, where the tumour was asymptomatic and did not display aggressive behaviour throughout follow-up, conservative treatment by periodic monitoring achieved local control of the disease at 3 years similar to that of the patients who underwent complete resection (R0).1,3,7
Due to the high rate of local recurrence and the morbidity after multiple surgeries, a wait-and-see approach should be considered for all desmoid tumours, primary or recurrences, which are asymptomatic and have not grown throughout their evolution.
Level of evidenceLevel of evidence III.
Ethical disclosuresProtection of people and animalsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their centre of work regarding the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflict of interestsThe authors have no conflict of interests to declare.
To Dr. Juan Pons de Villanueva and Dr. Dámaso Aquerreta.
Please cite this article as: Machado V, Troncoso S, Mejías L, Idoate MÁ, San-Julián M. Factores de riesgo para la recidiva local de la fibromatosis. Rev Esp Cir Ortop Traumatol. 2017;61:82–87.
