



Suicide and its prevention are a serious public health challenge. As the primary external cause of death in our country, it seems to be beyond our understanding and control in view of the numerous studies and interventions carried out. We conducted a study of suicide at the Valladolid Institute of Legal Medicine from 2018 to 2019.
Material and methodsAll deaths by suicide from 2018 to 2019 were collected and crossed with anonymized data of the Psychiatry Service of the University Clinical Hospital of Valladolid in 2019.
ResultsThe suicide rate was 8.5/100,000 inhabitants, 49 cases in 2018 and 44 in 2019, with a 3:1 male to female ratio, mainly in rural areas. The age group with the highest incidence was 31–70 years. Hanging in rural areas and precipitation in urban areas were the main methods. Affective disorders (F30−39 ICD-10) were the most common identified psychiatric disorders.
ConclusionsSuicide rates are slightly lower, while the risk profile and features of suicide remain constant in our environment more than 20 years later, indicating that preventive efforts carried out have not been completely successful. The effective prevention of suicide must start with better identification, prevention, and treatment of psychiatric disorders, but the contribution of the Institutes of Legal Medicine in the implementation of multilevel population programmes is also essential.
El suicidio y su prevención suponen un reto esencial en salud pública. Como primera causa externa de muerte en nuestro país, parece escapar a nuestra comprensión y control en vista de los numerosos estudios e intervenciones realizadas. Llevamos a cabo un estudio de los suicidios mortales estudiados por el Instituto de Medicina Legal y Ciencias Forenses de Valladolid durante el bienio 2018–2019.
Material y métodosSe recogieron todas las muertes por suicidio durante 2018–2019 y se cruzaron con los datos anonimizados del Servicio de Psiquiatría del Hospital Clínico Universitario de Valladolid en 2019.
ResultadosLa tasa de suicidios fue de 8,5/100.000 habitantes, 49 casos en 2018 y 44 en 2019, con una distribución de 3:1 para varones frente a mujeres, principalmente en el medio rural. La franja de edad con mayor incidencia fue la de 31–70 años. La ahorcadura en el medio rural y la precipitación en el urbano fueron los principales métodos. La comorbilidad psiquiátrica identificada más frecuente fueron los trastornos del estado de ánimo-afectivos (F30−39 CIE-10).
ConclusionesLas tasas de suicidio presentan un ligero descenso, mientras que el perfil de riesgo y las características del suicidio mortal se mantienen constantes en nuestro medio más de 20años después, lo que indica una escasa eficacia de los esfuerzos preventivos realizados hasta ahora. La prevención efectiva del suicidio debe partir de la mejor identificación, prevención y tratamiento de los trastornos psiquiátricos, pudiendo resultar esencial la participación de los Institutos de Medicina Legal y Ciencias Forenses en programas poblacionales multinivel.
Following Durkheim’s classic work at the end of the last century, a great many studies have been undertaken on the epidemiology of suicidal behaviours; nevertheless, this phenomenon still seems to be beyond our understanding and control. This is largely due to the extremely complex nature of this behaviour, as it is influenced by social and cultural factors as well as neurobiological ones.1 It also has major medical, legal, sociological, ethical and philosophical implications. When an individual decides to end their life, they are apparently exercising their free will within their social context; nevertheless, this is not the case for the majority of suicides, as psychological autopsies have repeatedly shown that in approximately 90% of deaths by suicide there are one or more psychiatric disorders,2–4 depression above all.5 Suicide is a severe preventable public health problem,6–8 and although it is the first external cause of death in Spain, with double the number of deaths caused by traffic accidents, the preventive measures taken do not correspond to its importance. Over the past decade a worrying tendency has emerged for suicide rates among younger people to increase, making it one of the main causes of loss of potential years of life.4 According to the latest available data from the National Institute of Statistics (INE), in 2018 suicide was the first absolute cause of death in men aged from 15 to 29 years old, and the second cause for women of the same age group.
It is necessary to know the size of a problem and how it is evolving before implementing any preventive measures in the field of public health. The Legal Medicine and Forensic Science Institutes (IMLCF) in Spain play a fundamental role in this respect. As it is obligatory to perform a judicial autopsy in a uniform manner9 this leads to a series of improvements: a higher rate of autopsies will lead to a higher percentage of correct diagnoses of suicide. As the latter rate rises, so too will the degree of certainty and validity of the statistics on which preventive strategies can be based.10
The Valladolid IMLCF has been developing a provincial suicide epidemiological monitoring system over recent years. It should be remembered that discrepancies exist between the official figures for suicides supplied by the INE and the actual rates. Approximately 10% of suicides have been calculated to be under-reported, and when the data generated in the daily work of the IMLCF are recorded in a rigorous and uniform way, the information on mortality due to suicide is more exhaustive and valid.9,11,12
The core aim of this study is to describe the suicides which occurred in the province of Valladolid during the two year period 2018–2019. It has the secondary purpose of analysing how this has changed in comparison with the biennium 1996–1997, showing how forensic sources can form the basis for future preventive measures.
Material and methodsAfter approval by the IMLCF Teaching and Research Committee, the data corresponding to deaths by suicide in the Valladolid (Spain) region were gathered for analysis. They were contained in the 2018 and 2019 report by the Palencia, Salamanca and Valladolid IMLCF management body for Valladolid.
The area of work covered by this management report corresponds to the province of Valladolid, which according to INE data had a population of 520,716 inhabitants on 1 January 2020.13 For legal purposes the province is divided into 3 administrative areas: Valladolid, including the capital and its suburbs, Medina del Campo and Medina de Rioseco, both of which are rural. This division was used to classify the areas studied in this paper as urban or rural.
After it had been formed and commenced working in 2003, the Pathology Department of the IMLCF in Valladolid has recorded the data on all of the deaths which gave rise to judicial intervention. All of the information collected is included in a database that is used to prepare an annual report.
Based on the working agreement between the IMLCF and the Regional Health Board, and with the aim of performing a rough analysis of clinical characteristics, anonymised data on suicides from the Psychiatric Department of Valladolid Hospital Clínico Universitario were also included. This department coordinates the Mental Health resources of the Eastern Health Region in the province of Valladolid, which has a population of 259,129 individuals according to Management data.
This study is solely descriptive, and data are grouped according to frequency. Total suicide rates are calculated per 100,000 inhabitants. Pearson’s chi-squared test is used as the association measure for nominal variables, while the Student t-test is used for quantitative variables. The level of significance was set at 5%. V24 of the SPSS programme was used for data analysis.
Descriptive statistical analysis was applied to the following variables: 3 categories of age (under 30 years, from 30 to 70 and over 70), sex, seasonality, geographical area (urban or rural, depending on the type of the above-mentioned administrative areas), mechanism used (hanging, firearm, fall from a height, poisoning by medication, drowning, sharp instrument, carbon monoxide poisoning, adverse reaction to drugs) and the presence of psychiatric comorbidity.
Lastly, the results were compared with the data corresponding to a similar period of time in the same area, 22 years earlier.14 This comparison is of interest due to the similarities between both studies: the period observed is also a biennium, the data sources are forensic, and the suicides were analysed according to sex and the mechanism used. These parallels were used to establish a temporal continuity.
ResultsThere were 93 deaths due to suicide in the province of Valladolid in the 2-year period 2018–2019: 49 in 2018 and 44 in 2019. Based on INE data corresponding to the population of Valladolid province in 2019,15 the total rate of mortality due to suicide is estimated to stand at 8.5/100,000 inhabitants. 71% of the total number of suicide victims were men, with 69% in 2018 and 73% in 2019.
The average age of fatal suicides was 58.6 years, with a standard deviation of ±17.9. Grouped according to age band (under 30 years, from 30 to 70 and older than 70), 6 fatalities were under the age of 30 years, 61 were aged from 30 to 70 years and 26 were over 70. 65.6% of fatal suicides therefore occurred in the age band that covers middle age (Table 1).
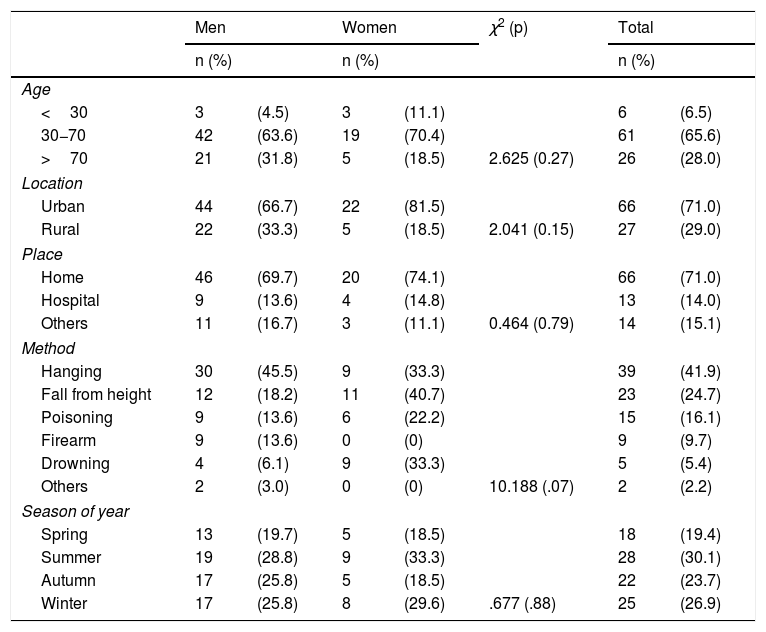
Characteristics of suicides grouped according to sex. Years 2018 and 2019 (n=93).
| Men | Women | χ2 (p) | Total | ||||
|---|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | |||||
| Age | |||||||
| <30 | 3 | (4.5) | 3 | (11.1) | 6 | (6.5) | |
| 30−70 | 42 | (63.6) | 19 | (70.4) | 61 | (65.6) | |
| >70 | 21 | (31.8) | 5 | (18.5) | 2.625 (0.27) | 26 | (28.0) |
| Location | |||||||
| Urban | 44 | (66.7) | 22 | (81.5) | 66 | (71.0) | |
| Rural | 22 | (33.3) | 5 | (18.5) | 2.041 (0.15) | 27 | (29.0) |
| Place | |||||||
| Home | 46 | (69.7) | 20 | (74.1) | 66 | (71.0) | |
| Hospital | 9 | (13.6) | 4 | (14.8) | 13 | (14.0) | |
| Others | 11 | (16.7) | 3 | (11.1) | 0.464 (0.79) | 14 | (15.1) |
| Method | |||||||
| Hanging | 30 | (45.5) | 9 | (33.3) | 39 | (41.9) | |
| Fall from height | 12 | (18.2) | 11 | (40.7) | 23 | (24.7) | |
| Poisoning | 9 | (13.6) | 6 | (22.2) | 15 | (16.1) | |
| Firearm | 9 | (13.6) | 0 | (0) | 9 | (9.7) | |
| Drowning | 4 | (6.1) | 9 | (33.3) | 5 | (5.4) | |
| Others | 2 | (3.0) | 0 | (0) | 10.188 (.07) | 2 | (2.2) |
| Season of year | |||||||
| Spring | 13 | (19.7) | 5 | (18.5) | 18 | (19.4) | |
| Summer | 19 | (28.8) | 9 | (33.3) | 28 | (30.1) | |
| Autumn | 17 | (25.8) | 5 | (18.5) | 22 | (23.7) | |
| Winter | 17 | (25.8) | 8 | (29.6) | .677 (.88) | 25 | (26.9) |
Hanging was the most common mechanism for both sexes and in the rural environment. Falls from a height was the second most commonly used method, above all in an urban context (Table 1). There is a significant association in men (χ2=15.725; P=0.008) between a rural or urban environment and the method used, as 77.3% used hanging in the rural environment as opposed to 29.5% who did so in an urban setting. On the contrary, 25% died due to a fall from a height in an urban setting as opposed to 4.5% who did so in a rural one. The differences between the other methods used are not significant. The preferred location for committing suicide was the victim’s own home (69.7% cases) in urban as well as in rural areas.
The seasonal or annual distribution of suicides was found to be uniform over the 24 months covered by the study, with little variation between months, seasons or one year in comparison with the other. Summer was the season with the highest number of suicides (30.1% of the total) (Table 1). There was a peak in the summer months of 2018, when there were 17 deaths, as opposed to 10 in the summer of 2019.
In the study of the psychiatric clinical histories of those who died corresponding to the Eastern Health Area, 68% of the 22 victims in 2019 analysed were found to have such a history. They were classified according to the CIE-10, and the most prevalent diseases were mood-affective disorders (categories F30-39 CIE-10), with 10 deaths, followed by disorders caused by substance abuse (F10-19 CIE-10). The latter may be broken down into those associated with alcohol (F10), with 3 deaths, disorders due to cocaine consumption (F14), with one death, and disorder caused by opiate consumption (F11), with one death.
Approximate tendencies were analysed by obtaining data on fatal suicides in the two-year period 1996–1997 from the Psychiatric Department. These corresponded to the same geographical area and the same IMLCF, and they were published in a paper with a similar subject to this one.2,3
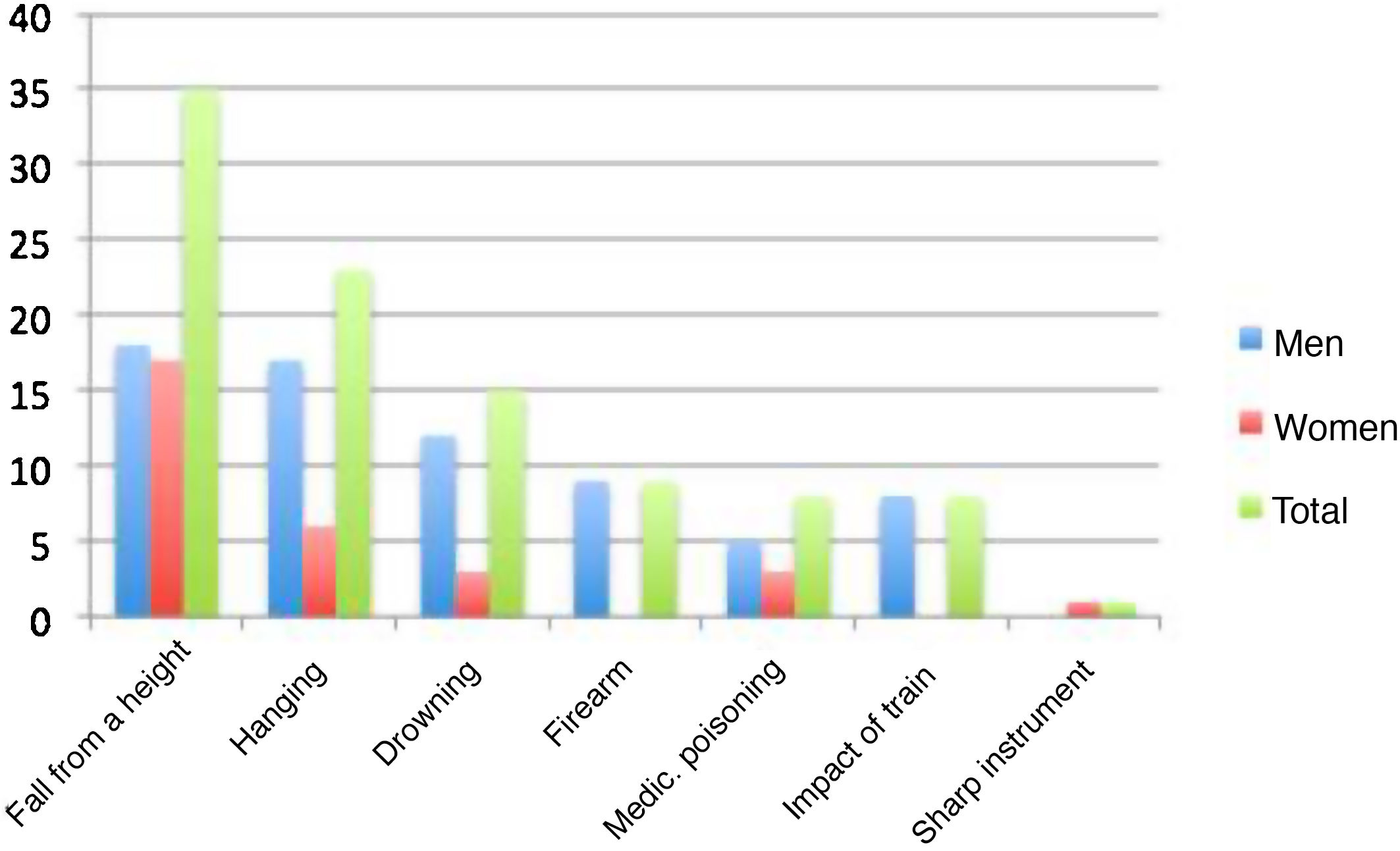
99 deaths occurred in the previous period, as opposed to 93 22 years later. The estimated total mortality rates based on INE data were 8.85 and 9.05 deaths/100,000 inhabitants in 1996 and 1997, respectively. The proportions corresponding to the sexes were 70% men-30% women. The most common mechanism used by both sexes was falling from a height, followed by hanging, and both of these methods accounted for 50% of all deaths (Fig. 1).
Discussion.")
Mortality rates due to suicide in the province of Valladolid in the 2018–2019 biennium seem to be relatively stable in comparison with those found 22 years earlier.2,3 It has to be borne in mind that the limited number of suicides in each province may lead to slight year-on-year variations that hinder the analysis of tendencies, so that longer time periods should therefore be used.
A recent study based on INE data seemed to find a slight decrease in suicides by men as well as women in Castile-Leon, although such tendencies are not uniform among the autonomous communities.16 It should also be remembered that the use of forensic sources in the study of suicide showed that INE data may reflect under-reporting of the same.11 Moreover, these results disagree with those of other studies, such as the one which showed an increase in the suicide rate during the recent financial crisis, in 2007.17
It is important to remember that preventive tools and programmes have been proven to be effective,6–8,18,19 and that if they are implemented and applied with regularity, they may reduce the number of suicides.
As is the case for other series, our study found that the proportion of men who committed suicide was three or four time higher than the number of women.20 Nevertheless, attempted suicides without fatality are far more common among women.21 Although this phenomenon may be explained by the lethality of the methods used by each sex,22 social factors have also been hypothesised to play a role here: gender roles determine different attitudes to the elements that trigger suicidal behaviour and its consequences.23 Men, and most especially in a rural environment, are expected to repress their emotions and be successful. Although a significantly higher proportion on men hang themselves in the countryside, a high percentage of women there also use this method (60% as opposed to 27% in urban environments). A potential line of research and prevention would therefore consist of analysing the differences in emotional terms between rural and urban areas, examining how responsibilities are distributed, and how families, education and society are organised.20
The concentration of fatal suicides from the fifth to the seventh decades of life is visible in the distribution according to age. It proved impossible to calculate the age-adjusted rate, so that it is only possible to speculate on the causes of this. Studies indicate that deaths due to suicide gradually increase with age, although this is most marked after the age of 65 years.24,25 There are hardly any suicides by young people or adolescents in the data analysed. Suicide by young people aged from 15 to 29 years old amounts to 8.5% of deaths due to an external cause in this age group, and in general terms it is the second cause of death after traffic accidents.15 Given the number of potential years of life that are lost and its importance as a public health indicator, this point means that the major preventive targets centre on young people. The factors influencing health for the population over the age of 65 years, such as increased frailty, physical and psychiatric comorbidities, widowhood and a rural environment seem to be the causes of this increase in the suicide rate.22,24
In urban as well as in rural areas the victim’s home was the preferred place for suicide. This agrees with other studies.25,26 Associated factors are: an increased sense of security in one’s own home, easy access to lethal resources and a lack of impediments when undertaking the fatal action.
Respecting the methods used, due to its characteristics hanging is a highly accessible and very lethal method in the home. Although it is used more often by men (in 45.5% of cases vs 33.3% for women), the differences between the sexes here are not significant. It would be hard to restrict access to hanging, as a wide range of objects can be used as a noose.26,27 Both of these factors, accessibility and lethality, are suggested as reasons why hanging is the most common method among all age groups, in different societies or geographical locations.
Falls from a height predominate in urban areas due to obvious architectural reasons. This corroborate the data we found in Valladolid, where the provincial capital city accounts for the majority of suicide using this method.
When the methods used are compared, the P value stands at .07, which is close to statistical significance (Table 1). When the corrected standardised residues are analysed the difference is found to lie mainly in the percentage of women who die due to a fall from a height (40.7%) as opposed to the men (18.2%). In this case, if the sample were larger it is possible that the differences would have been significant.
Falling from a height was the method used the most widely by both sexes in the period 1996–1997, ahead of hanging. This change may indicate an improvement in preventive actions, such as restricted access to high public places.22
Intoxication by medication is in third place in our series, and it is more common in women. It occupies lower places in the rankings shown by other studies.26,27 This method is in principle less lethal than the previous ones, so that it is associated more often with non-fatal suicide attempts than it is with fatalities. A similar pattern emerges when the sexes are compared here, as women predominate because men seem to prefer more lethal methods.24 Other methods were less common. For example, suicide by firearm occurred in 9.7% of cases, and it was only used by men. Drowning was only used in an urban area, favoured by easy access to the River Pisuerga where it runs through the provincial capital city.
Respecting seasonality, in our results the summer was the time with the highest incidence, with 27 deaths, although this figure hardly differs from those for winter and autumn, with 25 and 23 victims, respectively. The highest concentration of suicides arises in Spain during the summer, while on the contrary, autumn is the season with the lowest rates of death by suicide26–28.
According to studies of psychological autopsies, the presence of a psychiatric disorder is the main risk factor for suicide, although the literature cites rate of prevalence from 52% to 90%.6,25–27,29 In our case, the partial analysis aimed at established a clinical profile showed that there was a psychiatric history in 68% of deaths. This study agrees with other series analysed, in which mood-affective disorders (F30-39 CIE-10) and disorders associated with alcohol consumption are the two main complaints present in fatal suicides. Prevent and treating depression is equal to preventing suicide.2,19 The high rates of fatal suicides associated with alcohol consumption21,25–27,30 should lead us to reflect more and more completely on the permissiveness associated with this problem in Spain, above all in the youngest age groups in the population.
There is evident scientific interest in the problem of suicide and how to prevent it. In fact, 10% of the psychiatric publications in PubMed over the last 40 years have been on this subject.31 It is possible that problems such as faults in risk stratification due to the low frequency with which suicide occurs and a lack of sensitivity in identifying groups at risk may be partially responsible for the failure in prevention.31 This is also the case for the difficulty in evaluating the risk because of the lack of effective evaluation instruments and the limited results of proposed treatments and interventions in groups at risk. However, it is also true that State involvement and the allocated resources have been insufficient. Population strategies are necessary together with the creation and effective implementation of multilevel programmes covering broad sectors of the population. It would therefore be necessary for the IMLCF to coordinate and collaborate with mental health resources, as was the case here, as this would provide an important factor in the individualised analysis of cases, profiles and tendencies, as well as in creating effective preventive measures.27,30
LimitationsThe chief limitations here arise due to the data-gathering method, given that it was not possible to retrospectively obtain some of the records from the 1996–1997 database. These records would have enriched the analysis, and they include geographical area and the presence of physical or psychological comorbidity. It was also impossible to break down the results further according to age, which would have aided the calculation of standardised rates according to this factor. This study gave rise to the opportunity to create more detailed prospective data gathering.
Major year-on-year variations may occur because of the small sample size. It would therefore have been preferable to include a series over a longer time-span or to broaden it to include the whole Castile-Leon region, given its homogeneous demographic characteristics.
Finally, the inclusion of clinical data for only 22% of the sample is a great limitation, and it hinders drawing conclusions. This is mainly due to the difficulty of gaining access to digital clinical histories after the older records have been erased.
ConclusionsSuicide rates have remained relatively stable in the province of Valladolid in comparison with the study undertaken 23 years beforehand. The risk profile of those who die because of suicide has hardly changed, with the exception of the method used, as now hanging predominates over falls from a height. These questions may indicate that the preventive efforts undertaken to date have not been enough. The effective prevention of suicide must be based on the better identification, prevention and treatment of psychiatric disorders, especially depressive ones. It is also essential to create and implement multilevel programmes which include forensic sources and collaboration between the IMLCF and mental healthcare resources, which should play a fundamental role. This question should be treated as urgent, while also taking into account the current health crisis, in which an increase in the suicide rate is foreseeable.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Prieto Lorenzo V, Maderuelo Fernández JM, Gallardo Borge L, Santos Carrasco I, Queipo de Llano M, San Román A, et al. Análisis descriptivo del suicidio en el bienio 2018–2019 en Valladolid (España). Rev Esp Med Legal. 2021;47:143–149.