



Suicide is a major public health problem. The objective of this study is to analyse the demographic, clinical, and toxicological characteristics and the mechanisms of suicide in young people and middle-aged adults.
MethodRetrospective population study of completed suicide in subjects aged 14–55 who were subjected to a forensic autopsy in Bizkaia between 2016 and 2018.
Results272 suicides were recorded. The global incidence was 7.8/100.00 inhabitants/year. 127 were 14–55 years old. The rate was 3 times higher in men and increased with age. In 72%, some clinical risk factor was collected, mainly mental disorders (59%): mood disorders (23%), substance abuse (20.5%), and psychotic disorders (14%). 38% of addicts had another mental disorder. Physical illness (23%) and suicide attempt (20.5%) were also relevant factors. 41% were positive for alcohol and/or illicit drugs: ethanol (22%), cannabis (16%), cocaine (11%), and amphetamine (8%). This percentage was 79% in substance addicts. Substance abuse disorders (25% vs. 6.5%; P = 0.03) and presence of alcohol and/or drugs (49% vs. 16%; P = 0.001) were more prevalent in men. The most commonly used methods were fall from heights (35%) and hanging (31%).
ConclusionsThe incidence of suicide in Bizkaia is lower than the European average. Suicide is a complex problem associated with demographic and clinical factors (mainly depressive and substance abuse disorders) and recent use of alcohol and illicit drugs. Prospective multidisciplinary and multicenter researches are required in order to identify risk factors and to guide preventive measures.
El suicidio es un problema importante de salud pública. El objetivo del estudio es analizar las características demográficas, clínicas y toxicológicas, y los métodos del suicidio en jóvenes y adultos de mediana edad.
MétodoEl estudio fue retrospectivo poblacional del suicidio consumado en sujetos de 14-55 años que fueron objeto de autopsia forense en Bizkaia entre 2016-2018.
ResultadosSe registraron 272 suicidios. La incidencia global fue de 7,8/100.000 habitantes/año. Ciento veintisiete tenían entre 14 y 55 años. La tasa fue 3 veces superior en los varones y se incrementó con la edad. En el 72% se recogió algún factor de riesgo clínico, predominando los trastornos mentales (59%): del estado de ánimo (23%), por abuso de sustancias (20,5%) y psicóticos (14%). El 38% de los adictos tenía otro trastorno mental. La enfermedad física (23%) y el intento de suicidio (20,5%) fueron los factores relevantes. El 41% fueron positivos para sustancias de abuso: etanol (22%), cannabis (16%), cocaína (11%) y anfetamina (8%). Este porcentaje fue del 79% en los adictos a sustancias. Los trastornos por abuso de sustancias (25% vs. 6,5%; p = 0,03) y la presencia de alcohol y/o drogas (49% vs. 16%; p = 0,001) fueron más prevalentes en los varones.
ConclusionesLa incidencia del suicidio en Bizkaia es más baja que la media europea. El suicidio es un problema complejo asociado a factores demográficos, clínicos (principalmente, trastornos depresivos y abuso de sustancias) y al consumo reciente de alcohol y drogas ilegales. Para identificar los factores de riesgo y orientar las medidas preventivas se requieren investigaciones prospectivas multidisciplinares y multicéntricas.
Suicide is a major public health problem, due to its high incidence as well as the resulting economic burden for the affected family and social context.1–3
The act of suicide is a complex phenomenon that is associated with biological, psychological, socioeconomic, and cultural factors. Suicide is closely linked to multiple risk, protective, and causal factors, and it also gives rise to warning signs. To progress in the development of preventive strategies, it is necessary to know the impact of different risk factors within a territory, and this can be established by taking into account the demographic and pathological singularities of the victim.2,3
The knowledge generated within the forensic field is highly useful in the study of suicides, as an autopsy has to be carried out in all cases. Several forensic studies of suicide in Spain have been published in recent years.4–8 Forensic sources give a better reflection of the epidemiological magnitude of suicide than the official sources of the National Statistics Office.4 Furthermore, post-mortem study offers evidence that is relevant in clinical, pathological, and toxicological terms.
The characteristics of suicides in the young- and middle-aged adult populations have certain special connotations due to several reasons: the large number of years of life that are lost - which leads to a greater economic impact - and greater emotional repercussion on families; a range of risk factors have also been described, underlining the close association with alcohol and drug abuse.2,3,9
This study aims to analyse the demographical characteristics, clinical aspects (risk factors, triggers, and warning signs) and toxicological factors (recent consumption of alcohol, illegal drugs, and psychoactive medication), as well as to describe the mechanisms by which young people and middle-aged adults commit suicide.
Material and methodsStudy population. Sample selectionThis is a retrospective populational study of individuals aged from 14 to 55 years (inclusive) who had died due to suicide and were subjected to a forensic autopsy in Bizkaia from 1 January 2016 to 31 December 2018. Bizkaia is a province of the Autonomous Community of the Basque Country, and it has a total population of 1 158 439 individuals, of whom 141 554 are under the age of 14 years, 590 295 are aged from 14 to 55 years old, and 426 590 are older than 55 years (www.ine.es).
An autopsy is legally required to investigate violent deaths, which include suicides. In Bizkaia, this investigation corresponds to the single Forensic Pathology Department within the province.
Autopsy protocolThe autopsies were performed by forensic pathologists who had been trained following international recommendations. Clinical histories were recorded (relevant clinical data and data in connection with suicide, by means of accessing the electronic clinical history of the victim). The place of death was examined, and a complete autopsy was performed with macroscopic and microscopic examination and toxicological analysis of blood, urine and vitreous humour. As an alternative, in decomposing bodies the liver, kidney, or bile were used. The toxicological study, which was undertaken in the laboratory of the Basque Legal Medicine Institute, using the techniques of enzymatic immunoanalysis, liquid chromatography, and gas chromatography/mass spectrometry, was applied to all of the subjects except for those who were hospitalised, during more than 48 h.
Variables analysedThe following variables were analysed:
- •
Demographic variables. Two age groups were distinguished: young people aged from 14 to 34 years old, and middle-aged adults from 35 to 55 years old.
- •
Clinical data in connection with the suicide. Psychiatric disorders classified according to the CIE10, other risk factors (physical disease and/or chronic injury, previous suicide attempts, psychological, and personality factors and social or family risk factors) and acute factors (triggers and warning signs).
- •
Suicide mechanism. These were classified into 3 major groups: asphyxiation (hanging, suffocation, or drowning, etc.), violent methods (firearms, being run down by a train or tram, falls from a height, etc.) and toxic methods (the intake of caustic substances, intoxication by CO, intoxication by sulphuric acid, or medications, etc.).
- •
Toxicological findings, including substances of abuse and psychoactive drugs. A case was considered to be positive for alcohol when the concentration in the blood was ≥0.5 g/L.
Mortality rates were calculated on the basis of 2017 population census data of the National Institute of Statistics (www.ine.es). Gross rates of suicide were calculated for the total population and for each sex, as well as for the 14–34-year and 35–55-year age groups and for those over the age of 55 years.
Statistical analysis was undertaken using version 21.0 of the SPSS for Windows package. Categorical variables were compared using the χ2 test. The level of significance selected was P < .05.
ResultsTwo hundred and seventy two suicides were recorded in Bizkaia during the 3 years that the study lasted. 12% (n = 33) were aged from 14 to 34 years, 35% (n = 94) were aged from 35 to 55 years, and 53% (n = 145) were over the age of 55 years. The gross suicide rate was 7.8/100 000 inhabitants/year for the total population: 5.1 in the young people; 8.3 in the middle-aged adults, and 11.3 in those over the age of 55 years.
Six hundred and forty two autopsies were performed on individuals aged from 14 to 55 years: 318 were death by natural causes, 188 accidents, 127 suicides, and 9 homicides. The suicides represented 20% of all of the autopsies. Table 1 shows the demographic and clinical data, the mechanisms of suicide and the toxicological results of the suicides. 76% were male. The median age was 44 (percentile 25 = 34, and percentile 75 = 50) years. The relative risk of suicide was 3.1 times higher in men than it was in women.
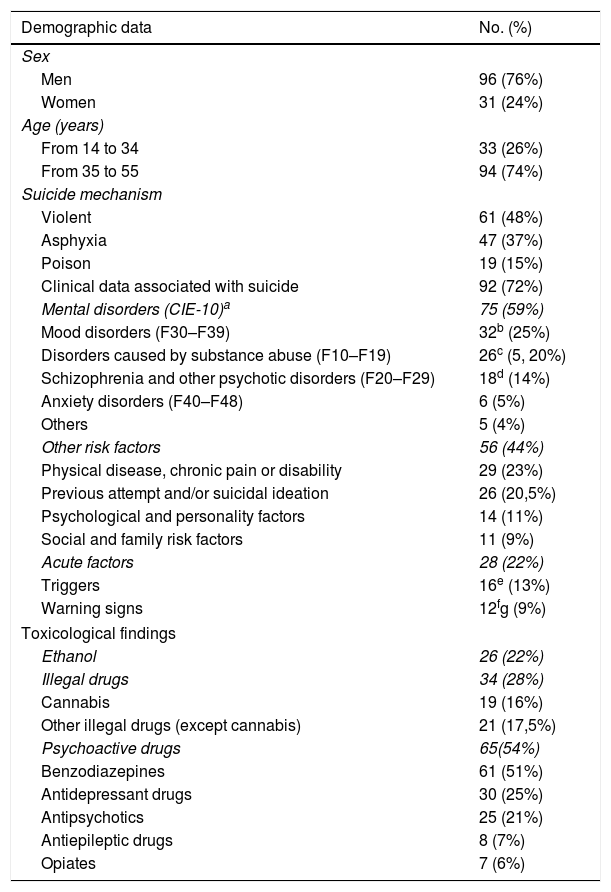
Descriptive analysis of the population examined: demographic data, suicide mechanisms, clinical data in connection with the suicide and toxicological results (n = 127).
| Demographic data | No. (%) |
|---|---|
| Sex | |
| Men | 96 (76%) |
| Women | 31 (24%) |
| Age (years) | |
| From 14 to 34 | 33 (26%) |
| From 35 to 55 | 94 (74%) |
| Suicide mechanism | |
| Violent | 61 (48%) |
| Asphyxia | 47 (37%) |
| Poison | 19 (15%) |
| Clinical data associated with suicide | 92 (72%) |
| Mental disorders (CIE-10)a | 75 (59%) |
| Mood disorders (F30–F39) | 32b (25%) |
| Disorders caused by substance abuse (F10–F19) | 26c (5, 20%) |
| Schizophrenia and other psychotic disorders (F20–F29) | 18d (14%) |
| Anxiety disorders (F40–F48) | 6 (5%) |
| Others | 5 (4%) |
| Other risk factors | 56 (44%) |
| Physical disease, chronic pain or disability | 29 (23%) |
| Previous attempt and/or suicidal ideation | 26 (20,5%) |
| Psychological and personality factors | 14 (11%) |
| Social and family risk factors | 11 (9%) |
| Acute factors | 28 (22%) |
| Triggers | 16e (13%) |
| Warning signs | 12fg (9%) |
| Toxicological findings | |
| Ethanol | 26 (22%) |
| Illegal drugs | 34 (28%) |
| Cannabis | 19 (16%) |
| Other illegal drugs (except cannabis) | 21 (17,5%) |
| Psychoactive drugs | 65(54%) |
| Benzodiazepines | 61 (51%) |
| Antidepressant drugs | 30 (25%) |
| Antipsychotics | 25 (21%) |
| Antiepileptic drugs | 8 (7%) |
| Opiates | 7 (6%) |
Other affective disorders (n = 11), recurring depressive disorder (n = 10), persistent mood disorders (n = 7), and bipolar disorder (n = 4).
Schizophrenia (n = 11), unspecified psychosis (n = 4), schizotypal disorder (n = 2), and delusional disorder (n = 1).
In 72% of the subjects, a clinical datum or risk factor associated with suicide was detected. Mental illness predominated among the risk factors, at 59%, of which mood disorders stood out (23%), disorders due to substance abuse (20.5%), and psychotic disorders (14%). 38% of the subjects with a diagnosis of disorder due to substance abuse had also been diagnosed with another mental disorder, chiefly mood disorders (23%) and psychotic disorders (11.5%).
Physical disease or chronic pain predominated among the other risk factors (23%), together with attempted suicide (20.5%). In 22% of cases, an acute factor was detected, in the form of a trigger or warning sign.
Suicide mechanisms48% of the suicides used violent means (falls: 35% of the total), 37% used asphyxiation (hanging: 31% of the total) and 15% used toxic substances (intoxication by medication: 11% of the total).
Toxicological resultsOf the 120 cases which were subjected to a toxicological study (94.5% of the total), 49 individuals (41%) tested positive for alcohol and/or illegal drugs. Twenty (20) of the 26 individuals who tested positive for alcohol showed high consumption of the same (concentration > 1 g/L). The most frequent illegal drug was cannabis (16%), followed by cocaine (11%) and amphetamines (8%). Other drugs were detected very rarely: heroin (2%) and ketamine (1%). The main psychoactive drugs were the benzodiazepines (51%), antidepressant drugs (25%), and antipsychotic drugs (21%) (Table 1).
Comparison of data according to sex and age groupSimilar percentages of men (59%) and women (58%) were diagnosed with a mental disorder. The only difference that can be underlined regarding mental disorders was that substance abuse occurred significantly more frequently in men (25% vs. 6.5%; P = .03). In post-mortem toxicological data the frequency of recent alcohol and/or drugs consumption was far higher in men (49% vs. 16%; = .001). The corresponding figures for illegal drugs were 34% vs. 13% (P = .03), while for ethanol they were 26% vs. 10% (P = .07).
The incidence of mental illness (63% vs. 48.5%) was higher in middle-aged adults than it was in young people, although the difference was not significant. No significant differences were found in the analysis of toxicological data between both age groups. The percentages of those who had recently consumed illegal drugs were similar (29% vs. 28%), while alcohol consumption (25% vs. 13%) and psychoactive drugs (58% vs. 42%) were slightly higher in the middle-aged adults.
No significant differences were found between the sexes or age groups in terms of the mechanism of suicide.
Comparison of the findings in connection with mental disordersThe presence of other risk factors was far higher in the subjects diagnosed with substance abuse than it was in the others (77% vs. 36%; P < .001). Those who were diagnosed with a mood disorder were more likely to have previously attempted suicide (41% vs. 14%; = .002).
Those who were diagnosed with a disorder caused by substance abuse were more likely to have consumed illegal drugs (58% vs. 21%; P = .001) and alcohol (37.5% vs. 18%; P = .05) than the others. 79% of those diagnosed with a disorder due to substance abuse had consumed illegal drugs or alcohol in the hours prior to their death.
Those who had a mental disorder were far more likely to have psychoactive drugs detected in their post-mortem toxicological analysis (81% vs. 19%; P < .001). Antidepressant drugs were detected more frequently in those who were diagnosed with a mood disorder (60% vs. 13%; P < .001), while antipsychotic drugs were detected more often in those who were diagnosed with psychosis (73% vs. 13%; P < .001).
DiscussionSeveral forensic studies have been published in recent years on the demographical and clinical characteristics of those who have committed suicide in different populations in Spain.5–8 This paper also presents toxicological findings which indicate recent exposure to substances of abuse (alcohol and illegal drugs), as these are considered to be a risk factor in young adults.2,9 On the other hand, toxicological analysis makes it possible to detect psychoactive drugs, thereby complementing the clinical information about the subjects. All of the above consideration enables better identification of the risk profiles for suicide, which is of use in preparing preventive strategies.
The annual suicide rate in Bizkaia (7.8/100 000 inhabitants) has remained stable from the year 2000 to date, varying from 7 to 8 cases per every 100 000 inhabitants.10 This figure is similar to the average rate recorded in Spain during the period analysed (which varied from 7.25 to 7.90),11 which is relatively low in comparison with other European countries, where the overall rate stands at 12.9 per 100 000.1 Respecting the difference according to sex, in Bizkaia the relative risk of men is three times that for women. This datum is similar to the one described for the majority of European countries, including Spain.1,10–12 The risk of suicide gradually rises with age,2,3,10–12 so that in this study suicide rates in those aged over 55 years old were double the rate for young adults.
The methods used to commit suicide vary geographically, depending on cultural patterns and their availability.1,2 The most widely used methods worldwide are hanging, poisoning by pesticides and the use of firearms.2 In Spain, hanging and falls from a height are the main mechanisms.5–8 Falls predominate in urban areas due to architectural considerations.5 As the majority of the population in Bizkaia is urban, it is not surprising that falls are the main method used. Although several works have concluded that the methods used to commit suicide vary according to sex2,13,14 (e.g., with poisoning being used more often by women) in Bizkaia we found no statistically significant differences.
The presence of risk factors and triggers associated with suicide varies depending on geographical and cultural criteria. The design of our study enabled highly reliable data-gathering for certain variables (the existence or otherwise of mental disorders and physical diseases in life, and the recent consumption of substances of abuse). It was less reliable for other variables, as they were not systematically covered by post-mortem studies (e.g., psychological or personality factors, as well as social and family aspects and triggers). This fact may have led to under-estimation of the real figures corresponding to these factors.
Mental disorders were the most common risk factors, and the presence of psychiatric diseases in the suicidal population would be up to 10 times greater than it is in the general population.2,3,15–19 In Bizkaia, 59% of the sample had been diagnosed with a mental disorder, and in 54%, toxicological analysis detected the presence of a psychoactive drug. From 60% to 90% of individuals who commit suicide have a mental disorder.2,16–18 One of the reasons why this study found a figure in the lower limit of this range may be the age of the population that was analysed, as individuals over the age of 55 years were excluded. Suicides associated with depression are more common in older people.2 The frequency of mental disorders in Bizkaia was therefore found to be somewhat higher in middle-aged adults than it was among younger subjects.
As is the case in the majority of studies, mood disorders2 were the most frequent. 25% of those who committed suicide had been diagnosed with a mood disorder, and antidepressant drugs were detected in 25% of the subjects. Nevertheless, the prevalence of depression was lower than in other series, which conclude that half of all suicides are associated with depression and other mood disorders. The prevalence of psychosis usually varies from 10% to 20%, and a similar figure was found in Bizkaia, with a prevalence of psychotic disorders amounting to 14% and the presence of antipsychotic drugs in 21%.2,16–21
In Bizkaia, an outstanding finding was the relatively high preponderance of individuals diagnosed with disorders due to substance abuse, as this was even higher than the proportion of those diagnosed with psychotic disorders. Another relevant datum is the high proportion of dual disease: 38% of those addicted to alcohol or illegal drugs had been diagnosed with another mental disorder, chiefly depression. The comorbidity of psychiatric disorders and substance abuse increases the risk of suicide.2
The prevalence of illegal drug consumption (28%) is higher in our study than is the case in the majority of publications. The prevalence of recent ethanol consumption was relatively high (20%), although it was lower than in other series.22–25 On the other hand, if we compare our data with those of sociological surveys of the general population in the same region, the rate of recent alcohol and drug consumption was higher than could have been expected.26 However, this comparison should be accepted with caution, given the differing sources of data.
Although in population surveys cannabis consumption is considerably higher than the consumption of all other drugs (the prevalence of weekly cannabis consumption is 4 times higher than the monthly consumption of other illegal drugs),26 in our sample the presence of other drugs was slightly higher than the presence of cannabis. If we take this datum into account together with the fact that the average duration of cannabis in the body is considerably longer, the impact of recent cocaine and amphetamine consumption (as these drugs were detected the most often in the suicides covered by this study) would be noticeably greater than that of cannabis. This agrees with the findings of other publications: the relative risk of suicide in individuals diagnosed with disorder due to cocaine use is especially high compared with other addictions;27 and cannabis consumption is not in itself considered to be a risk factor.2
The impact of acute consumption (the presence of substances of abuse in the post-mortem toxicological study) and chronic consumption (disorders caused by the use of psychoactive substances) of alcohol and drugs of abuse was significantly higher in men than it was in women, as has been described in other works,9 and this would be expected if we consider that such consumption is more prevalent in men in the general population.26
Of the other risk factors, physical disease or chronic pain were the most prevalent. This finding confirms the importance of physical diseases and chronic pain in cases of suicide.2,3 Approximately 40%–50% of suicides have a history of attempted suicide.3,8,28 In our study, this figure was lower, and this may be due to the age range of the population analysed (as it excluded those over the age of 55 years), together with the lower incidence of depressive disorders in our sample. Nevertheless, it is not possible to rule out under-estimation due to a distortion in data gathering. The figures for the remaining risk factors are lower than those found in other series, and this is due to the methodological deficiencies in the data gathering for our research.29
The main limitation of this work is that the study is retrospective without a control group, so that it neither proves causality nor establishes risk factors. Another limitation is the deficiency in data gathering for certain risk variables, triggers, and warning signs.
Implications for preventionThe fact that the suicide rate in our geographical area has not fallen10,11 shows the need to enhance suicide prevention strategies. Among other measures, the identification of risk factors should be improved in each population, to enable better management of the different prevention programmes.
Knowledge of the incidence and methods used to commit suicide, together with its distribution according to sex and age, is necessary to optimise preventive strategies. The findings of this work are useful as they add to our knowledge of the clinical and toxicological risk factors involved in suicide. A clinical factor associated with suicide is found in 3 of every 4 suicides, of which mental disorders stand out the most, chiefly mood disorders. Given the high prevalence of disorders caused by the abuse of alcohol and illegal drugs, and the high level of consumption of these substances by men, specific prevention campaigns should be prepared, aimed at those who consume substances of abuse.
The difficulties found in gathering data on certain risk factors show the need to create a complete, structured, and systematic system to ensure the correct recording of all of the factors associated with suicide, so that future prospective studies will be possible in which forensic, mental, and public health professionals will be able to work together.4
In the Basque Country, in the year 2019, the Health Department of the Basque Government activated the Suicide Prevention Strategy.3 The measures for epidemiological monitoring and research included the creation of a registry of suicides based on forensic data. The results of this work will be relevant in the preparation of a follow-up study of the factors associated with suicide, as well as to evaluate the efficacy of the different preventive measures included in the Suicide Prevention Strategy.
As has been shown by the experience in the field of sudden death,30 developing multicentre forensic studies would constitute a major advance in improving our knowledge of suicidal behaviour.
FinancingThe work described was previously published within the context of the end-of-degree project by Mikel Aiartzaguena.
This study received no specific grant from any public, commercial or not-for-profit body.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Aiartzaguena M, Morentin B. Factores de riesgo del suicidio consumado en los jóvenes y los adultos de mediana edad: estudio poblacional forense. Revista Española de Medicina Legal. 2021;48:53–59. https://doi.org/10.1016/j.reml.2021.09.003