



The approach to child abuse due to domestic violence is one of the most complex in forensic medicine. The objectives are the evaluation of the physical-psychological damage and of the indicators of child abuse, the analysis of credibility of the testimony and the study of the family dynamics. In this article, the systematic approach to child abuse is reviewed: sources of documentation, psychological evaluation, story gathering and use of psychological tests. A model of psychological exploration based on blocks is proposed, guidelines for the determination of the causal relationship between allegation of ill-treatment and damage detected are formulated, and recommendations for the analysis of credibility in order to conclude on the coherence of the story are suggested. The main indicators of child abuse are also described. The conclusions of the forensic report must be based on solid evidence, since poor evaluation could cause irreparable damage to children and their families.
El abordaje del maltrato infantil intrafamiliar (MII) es uno de los más complejos en medicina forense. Los objetivos periciales son la evaluación del daño físico-psíquico y de los indicadores de MII, el análisis de credibilidad del testimonio y el estudio de la dinámica familiar. En este artículo se revisa la sistemática de abordaje del MII (fuentes de documentación, evaluación psíquica, recogida del relato y uso de pruebas psicológicas); se propone un modelo de exploración psíquico basado en bloques, se formulan pautas para la determinación del nexo causal entre hechos denunciados y daño detectado y para el análisis de la credibilidad con el fin de concluir sobre la coherencia del relato. También se describen los principales indicadores de MII. Las conclusiones del informe forense se deben basar en evidencias sólidas ya que una peritación deficiente podría producir daños irreparables en víctimas menores y sus familias.
Child abuse can be defined as the harm caused to a child by behaviour that goes against social norms by another person or group of persons. This behaviour can have serious consequences in the development of child victims (CV) as children are particularly vulnerable to victimisation due to their level of dependence and lack of autonomy vis-à-vis the adult population. A few years ago, a study line emerged termed evolutionary victimology in order to study the diversity of abuse that CV can experience throughout their development, which has had major impact on the knowledge of this phenomenon. Child victimisation is currently considered one of the principal public and community health problems, and one of the most difficult to approach, both clinically and by experts.1–3
Of the different types of abuse that children might suffer, in this article we will focus on that occurring in the intra-familial environment. Intra-familial child abuse (ICA) can be defined as any action, omission or negligent treatment, not accidental, that deprives a minor of his/her rights and well-being, that threatens or interferes with his/her physical, mental or social development and whose perpetrators are from the family environment. Neglect is the most frequent, followed by emotional and physical abuse. Cases of sexual abuse are in the minority.4–9 In a recent study on the abuse of CV assessed in the Comprehensive Forensic Assessment Unit of Bizkaia, the most prevalent were emotional abuse and witnessing violence between parents in the family (gender-based violence), followed by physical violence, polyvictimisation and sexual violence.10
ICA is one of the most damaging traumas for CV and can have serious consequences for their well-being and development. It is also a determining factor in child neglect. Due to its special characteristics, it requires a differential social, health and legal approach.4–7 In the forensic area, intervention in ICA is of special interest due to its social and legal impact and because of the growing frequency of calls for experts and their complexity. Forensic expertise is first-rate scientific evidence in legal investigation through which the judge is made able to appreciate and assess criminal acts and their repercussions on the health of victims.
Certain elements make the forensic approach to ICA particularly complex and difficult to assess.4–11 ICA occurs in a private setting where the victim is physically and emotional dependent on the abuser, which makes it more difficult to disclose the abuse, and favours interference from the abuser as well as others. This interference may be motivated by an attempt to dissuade CV from mentioning what has happened, or that they are attempting to exaggerate or distort what they have experienced. This is especially dangerous in gruelling separation processes in which the child may be being instrumentalised.
On other occasions difficulty arises because forensic assessment is requested after the application of urgent social intervention measures. This is the case with minors in distress who find themselves living with foster families or in children’s centres. CV may reject further examination and be impermeable and reluctant to report details of their family life that they believe could jeopardise their return home.
Another differential factor of ICA is that it frequently concurs with gender-based violence.10 Law 26/2015, of 28 July, amending the system for the protection of children and adolescents, extends the consideration of gender-based violence victims to the children of female victims and grants them the same protection as their mothers. These experts require comprehensive assessment of the victims (women and minors) and of the accused, from a physical, psychological and social perspective, considering the consequences not only of specific assaults but also of a climate of continuous violence. This assessment is undertaken in the Units for Comprehensive Assessment of Gender-based Violence (UVIVG) that comprise multidisciplinary teams of professionals in forensic medicine, psychology and social work.
With the intention of improving care for abused CV, several ministerial documents on intervention guidelines have been published recently.8,9 However, their implementation in the Institutes of Legal Medicine and Forensic Sciences (IMLCF) is uneven, as the work must adapt to the creation or otherwise of specialist forensic services and to existing professional means. The comprehensive approach to ICA, unlike child sexual abuse,12,13 has received little coverage in the forensic literature.
The aim of this article is to study the forensic assessment of ICA in depth, focusing especially on the mental assessment and credibility of serious or repeated abuse with the intention of providing a basis to help homogenise forensic practice. It is a proposal that seeks to expose in a clear and simple way the methodology to be followed in the forensic medical assessment of this type of aggressions
Basic action criteriaThe main objectives of ICA experts are to assess physical and psychological injuries, the establishment of the causal link between the harm and events reported, to analyse the credibility of the testimony and study the family dynamics in order to recommend or otherwise the adoption of protective measures for the CV.
Intervention may be urgent or scheduled. The latter requires immediate assessment by the duty forensic officer. This is the case for minors who have suffered recent sexual assault or physical injuries that require health care. Scheduled experts are requested if there is suspicion of ICA and usually the specialist psychiatric services intervene. The UVIVG are in charge when this coexists with gender-based violence.
The following recommendations will be considered in the scheduled assessment:
- •
Examinations should be carried out according to a standardised protocol that includes a comprehensive and multidisciplinary assessment of the CV and their family environment.
- •
Professionals must have specific training in assessment techniques that enable collection of the story and analysis of psychological impact, as well as preventing secondary victimisation. They must also have knowledge of intrafamily and childhood problems, the available institutional resources and social-health strategies to be adopted.
- •
The multidisciplinary team must work in coordination with other institutions and with each other. Each IMLCF must define the role to be played by each professional. Social work will focus on the social indicators (risk and protection) present both in the CV and in their environment. To this end, in addition to taking part in interviews, it should play an active external role, with home interviews, visits to institutions and direct observation of the community reality. The work of medical and psychological personnel will focus on the interviews and examinations carried out in the consultation. Psychology personnel will also provide the data obtained in the psychological tests. The medical professional will assess physical and psychopathological damage to both victim and aggressor
- •
Some operatives should adhere to the principle of minimum intervention, limiting themselves to detecting suspicion of abuse and refer the CV to professionals with specific training.
- •
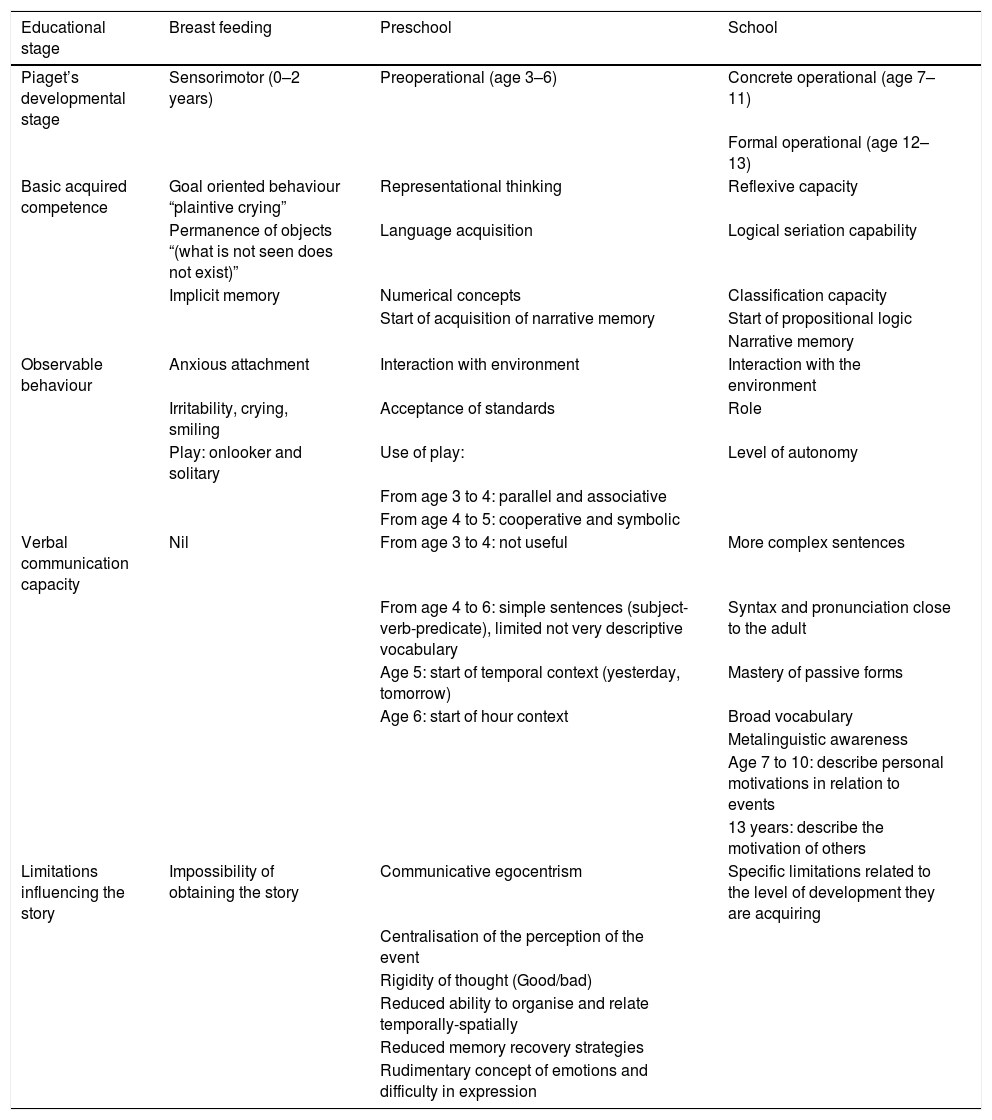
The interview must be adapted to the age and stage of maturity and development of the CV, as this is decisive in their ability to communicate (Table 1).
Table 1.Classification of minors according to their ability to communicate.
Educational stage Breast feeding Preschool School Piaget’s developmental stage Sensorimotor (0–2 years) Preoperational (age 3–6) Concrete operational (age 7–11) Formal operational (age 12–13) Basic acquired competence Goal oriented behaviour “plaintive crying” Representational thinking Reflexive capacity Permanence of objects “(what is not seen does not exist)” Language acquisition Logical seriation capability Implicit memory Numerical concepts Classification capacity Start of acquisition of narrative memory Start of propositional logic Narrative memory Observable behaviour Anxious attachment Interaction with environment Interaction with the environment Irritability, crying, smiling Acceptance of standards Role Play: onlooker and solitary Use of play: Level of autonomy From age 3 to 4: parallel and associative From age 4 to 5: cooperative and symbolic Verbal communication capacity Nil From age 3 to 4: not useful More complex sentences From age 4 to 6: simple sentences (subject-verb-predicate), limited not very descriptive vocabulary Syntax and pronunciation close to the adult Age 5: start of temporal context (yesterday, tomorrow) Mastery of passive forms Age 6: start of hour context Broad vocabulary Metalinguistic awareness Age 7 to 10: describe personal motivations in relation to events 13 years: describe the motivation of others Limitations influencing the story Impossibility of obtaining the story Communicative egocentrism Specific limitations related to the level of development they are acquiring Centralisation of the perception of the event Rigidity of thought (Good/bad) Reduced ability to organise and relate temporally-spatially Reduced memory recovery strategies Rudimentary concept of emotions and difficulty in expression - •
The best interests of the minor should always be paramount.
This information enables us to approach the case, guide the examination of the CV and avoid unnecessary re-assessments. In addition, it provides further evidence that may or may not be congruent with the events described. It is advisable to analyse these elements: allegation and investigation diligences; clinical history; medical-forensic report of injuries (in the event of on-call intervention); psychological reports and family psychosocial teams, community social services and educational guidance teams. The social worker’s role is invaluable for this purpose.
It is also necessary to interview adults related to the CV (mainly parents, but also teachers, paediatricians, foster family, etc.). Information provided by parents, principally in disputes over separation or custody, should be assessed with caution as it could be confusing or biased.
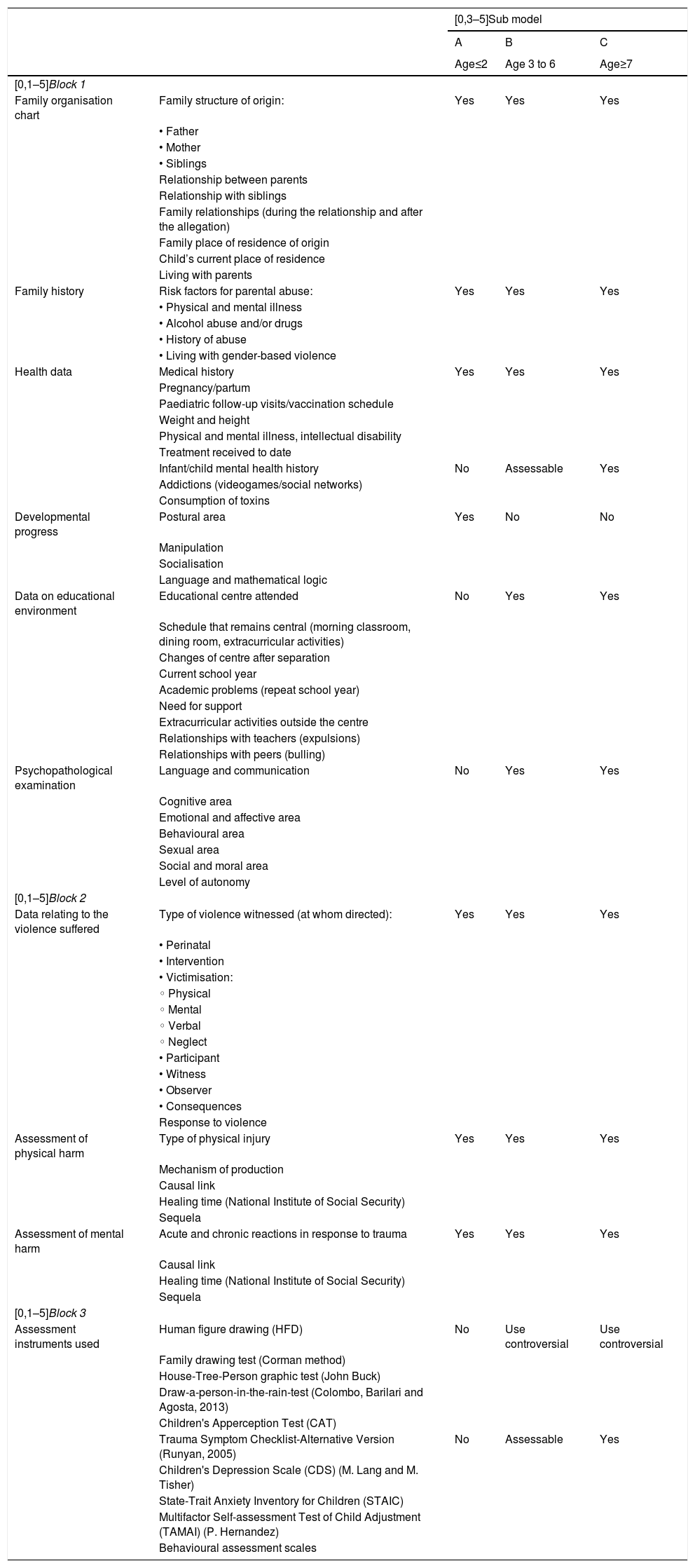
Interview and psychological examination of the child victimThe proposed examination model is based on a semi-structured interview divided into three blocks (Table 2). The biographical, family, educational and health data are collected in the first block at the same time as the psychopathological examination is undertaken. In the second block, the interview focusses on the analysis of the violence suffered and its consequences. An open and flexible script is recommended, with questions formulated in terms that facilitate broad answers and spontaneity. If there are no spontaneous references to the violence suffered, attempts should be made to deal with it in a simple manner, avoiding targeted or suggestive questions. Closed questions will be asked in the third block to gather specific information and decide which psychometric instruments will be applied.
Proposed examination model: Blocks and items to be explored according to the age of the child victim (A, B and C pattern).
| [0,3–5]Sub model | ||||
|---|---|---|---|---|
| A | B | C | ||
| Age≤2 | Age 3 to 6 | Age≥7 | ||
| [0,1–5]Block 1 | ||||
| Family organisation chart | Family structure of origin: | Yes | Yes | Yes |
| • Father | ||||
| • Mother | ||||
| • Siblings | ||||
| Relationship between parents | ||||
| Relationship with siblings | ||||
| Family relationships (during the relationship and after the allegation) | ||||
| Family place of residence of origin | ||||
| Child’s current place of residence | ||||
| Living with parents | ||||
| Family history | Risk factors for parental abuse: | Yes | Yes | Yes |
| • Physical and mental illness | ||||
| • Alcohol abuse and/or drugs | ||||
| • History of abuse | ||||
| • Living with gender-based violence | ||||
| Health data | Medical history | Yes | Yes | Yes |
| Pregnancy/partum | ||||
| Paediatric follow-up visits/vaccination schedule | ||||
| Weight and height | ||||
| Physical and mental illness, intellectual disability | ||||
| Treatment received to date | ||||
| Infant/child mental health history | No | Assessable | Yes | |
| Addictions (videogames/social networks) | ||||
| Consumption of toxins | ||||
| Developmental progress | Postural area | Yes | No | No |
| Manipulation | ||||
| Socialisation | ||||
| Language and mathematical logic | ||||
| Data on educational environment | Educational centre attended | No | Yes | Yes |
| Schedule that remains central (morning classroom, dining room, extracurricular activities) | ||||
| Changes of centre after separation | ||||
| Current school year | ||||
| Academic problems (repeat school year) | ||||
| Need for support | ||||
| Extracurricular activities outside the centre | ||||
| Relationships with teachers (expulsions) | ||||
| Relationships with peers (bulling) | ||||
| Psychopathological examination | Language and communication | No | Yes | Yes |
| Cognitive area | ||||
| Emotional and affective area | ||||
| Behavioural area | ||||
| Sexual area | ||||
| Social and moral area | ||||
| Level of autonomy | ||||
| [0,1–5]Block 2 | ||||
| Data relating to the violence suffered | Type of violence witnessed (at whom directed): | Yes | Yes | Yes |
| • Perinatal | ||||
| • Intervention | ||||
| • Victimisation: | ||||
| ◦ Physical | ||||
| ◦ Mental | ||||
| ◦ Verbal | ||||
| ◦ Neglect | ||||
| • Participant | ||||
| • Witness | ||||
| • Observer | ||||
| • Consequences | ||||
| Response to violence | ||||
| Assessment of physical harm | Type of physical injury | Yes | Yes | Yes |
| Mechanism of production | ||||
| Causal link | ||||
| Healing time (National Institute of Social Security) | ||||
| Sequela | ||||
| Assessment of mental harm | Acute and chronic reactions in response to trauma | Yes | Yes | Yes |
| Causal link | ||||
| Healing time (National Institute of Social Security) | ||||
| Sequela | ||||
| [0,1–5]Block 3 | ||||
| Assessment instruments used | Human figure drawing (HFD) | No | Use controversial | Use controversial |
| Family drawing test (Corman method) | ||||
| House-Tree-Person graphic test (John Buck) | ||||
| Draw-a-person-in-the-rain-test (Colombo, Barilari and Agosta, 2013) | ||||
| Children's Apperception Test (CAT) | ||||
| Trauma Symptom Checklist-Alternative Version (Runyan, 2005) | No | Assessable | Yes | |
| Children's Depression Scale (CDS) (M. Lang and M. Tisher) | ||||
| State-Trait Anxiety Inventory for Children (STAIC) | ||||
| Multifactor Self-assessment Test of Child Adjustment (TAMAI) (P. Hernandez) | ||||
| Behavioural assessment scales | ||||
The interview should be adapted to age and maturity, both to mark the course of the interview and to choose the type of questions to be asked. Generically, we can differentiate three sub-models:
- •
Sub model A: The assessment of minors up to 2 years old, without verbal communication skills. This will always be carried out accompanied by an adult, from whom the information of interest will be obtained. The data will be obtained with the child through play and observation.
- •
Sub model B: For assessment of minors from 3 to 6 years old, with limited verbal communication capacity.
- •
Sub-model C: For assessment of minors with the ability to maintain developed verbal communication (pre-adolescence and adolescence).
The informed consent of the relative must be given, explaining, both to the relative and to the CV, in an understandable way, the scope and objectives of the examination. If 2 experts are involved, the guidelines to be followed by each professional must be established: one must play a closer role with the victim, conducting the interview, and the other must maintain a secondary role, observing and collecting data, and adding, if necessary, unaddressed issues. If more than one interview is required, it will be scheduled in close succession (1–2 weeks) and will be conducted by the same professionals.
For the CV to talk about their experiences in detail and unreservedly, the following is recommended:5,14–19
- •
Use a methodology that prioritises their psychological well-being and encourages good rapport.
- •
Conduct the interview in a quiet space adapted for the forensic clinic.
- •
Encourage a safe environment and a climate of trust that minimises secondary victimisation and fear of retaliation by others.
- •
An attitude of empathy, openness, active listening and close eye contact. Interference and incentives should be avoided.
- •
Use simple questions and understandable language adapted to age.
- •
Use materials such as toys or drawings, especially with younger children, that stimulate symbolic communication and verbalisations
- •
Use the child's references and behaviours as guides, avoiding judicious comments
- •
Do not invade the CV's personal space or exert time pressure.
- •
Conduct the interview without the presence of parents (except in the case of minors without communication skills).
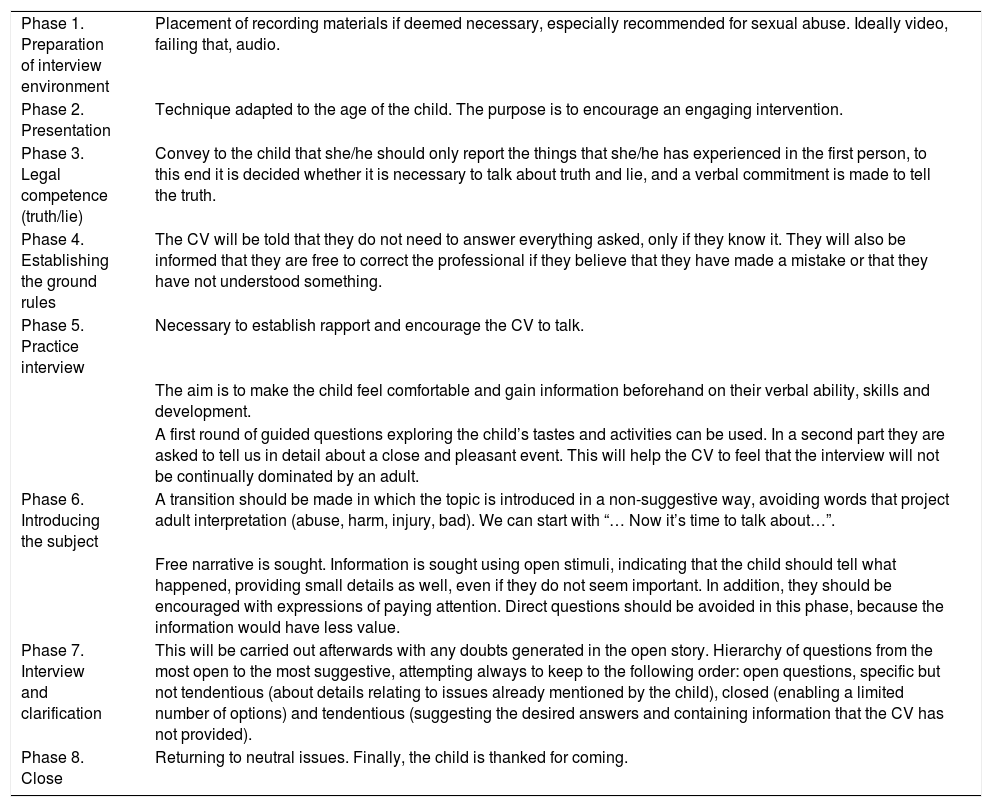
In order to systematise the interviews, various guidelines have been proposed, such as the Michigan State forensic interview protocol (Table 3) and the investigative protocol for victims of sexual abuse.18,19
Proposed stages for story collection in the "Michigan State Forensic Interview" protocol (partially modified).
| Phase 1. Preparation of interview environment | Placement of recording materials if deemed necessary, especially recommended for sexual abuse. Ideally video, failing that, audio. |
| Phase 2. Presentation | Technique adapted to the age of the child. The purpose is to encourage an engaging intervention. |
| Phase 3. Legal competence (truth/lie) | Convey to the child that she/he should only report the things that she/he has experienced in the first person, to this end it is decided whether it is necessary to talk about truth and lie, and a verbal commitment is made to tell the truth. |
| Phase 4. Establishing the ground rules | The CV will be told that they do not need to answer everything asked, only if they know it. They will also be informed that they are free to correct the professional if they believe that they have made a mistake or that they have not understood something. |
| Phase 5. Practice interview | Necessary to establish rapport and encourage the CV to talk. |
| The aim is to make the child feel comfortable and gain information beforehand on their verbal ability, skills and development. | |
| A first round of guided questions exploring the child’s tastes and activities can be used. In a second part they are asked to tell us in detail about a close and pleasant event. This will help the CV to feel that the interview will not be continually dominated by an adult. | |
| Phase 6. Introducing the subject | A transition should be made in which the topic is introduced in a non-suggestive way, avoiding words that project adult interpretation (abuse, harm, injury, bad). We can start with “… Now it’s time to talk about…”. |
| Free narrative is sought. Information is sought using open stimuli, indicating that the child should tell what happened, providing small details as well, even if they do not seem important. In addition, they should be encouraged with expressions of paying attention. Direct questions should be avoided in this phase, because the information would have less value. | |
| Phase 7. Interview and clarification | This will be carried out afterwards with any doubts generated in the open story. Hierarchy of questions from the most open to the most suggestive, attempting always to keep to the following order: open questions, specific but not tendentious (about details relating to issues already mentioned by the child), closed (enabling a limited number of options) and tendentious (suggesting the desired answers and containing information that the CV has not provided). |
| Phase 8. Close | Returning to neutral issues. Finally, the child is thanked for coming. |
CV: child victims.
First contact should promote spontaneous communication. It is suggested to start with an informal and friendly presentation to facilitate engaging with the CV. Through simple conversations it will be possible to assess their ability to communicate, express ideas and thoughts. Basic dialogue skills such as asking for clarifications or showing disagreement if they believe they have not been understood are not yet developed under the age of 7.
Course, intonation and content of language, as well as syntactic ability and richness of vocabulary must be assessed.
Cognitive areaWe will assess attention span, concentration, intellectual development and mnestic functions. The amount of information remembered will vary according to age at age 5–6, there is consistent memory capacity to offer a story with some details, but it will be difficult to order memories in an episodic way. There are other factors that influence memory, such as attention deficit, time elapsed since the experience and the habit of abuse, which tends to erase the differences between episodes and replace them with stereotyped scripts.
It will be necessary to take into account possible cognitive distortions derived from ICA such as hostile attributional biases that cause the CV to modify their relationship pattern with other people for fear of being rejected, the internalisation of aggressive conflict resolution patterns that could increase rejection among peers or guilt as a trigger for aggression. All of this will affect their self-concept and how they interpret and relate events experienced.
Emotional and affective areaIn the interview it is essential to explore the level of knowledge that the CV has of their affections and emotions and their ability to convey them. Graphic tools (e.g. drawings of faces or "little faces" or the "monster of emotions") facilitate this assessment
General mood and its fluctuations will be explored (“How do you feel most of the time?”, “What makes you happy?”, “What makes you sad?”), anger and rage (“What do you do when you want something and can’t have it?), “Are you very angry?” Do you fight outside the home?) and fears and feelings of distress (“I’m very afraid of spiders, is there anything that makes you feel very afraid for yourself?”, “What can you use to take that fear away?”, “Does anyone help you when you’re afraid?”).
Emotional expressions (postures, facial expressions, verbalisations) reactive to related events will be noted.
Assessment of this area is particularly complex due to children’s difficulty with introspection, which can cause biases in interpreting the story.
Behavioural areaThe attitude of the CV when entering the consultation and separating from the accompanying parent, the capacity to remain seated, actions and gestures, repetitive movements, unusual postures and excessive containment or passivity are assessed. In addition, their attitude towards the professional interview and questions asked, if they allow eye contact, if they are submissive, cooperative, cautious, attentive, friendly, hostile, rebellious, challenging, etc… In very small children, given the hyperactivity usual for their age, it is advisable to offer a wide space that allows play and that will serve to analyse the child’s stage of play.
Sexual areaSexual and gender identity and development should be analysed. From the age of 6 onwards, sexual identity begins to be established; until then it depends on superficial factors such as clothing.
In order to explore sexual maturity, it is practical to use films or stories that the child knows and in which he or she can identify with a character. Subsequently, we can ask the reason for their choice to detect whether it has been conditioned by differences linked to sex.
The CV’s knowledge of both their sexuality and the sexual activities of others will be considered, paying special attention to vocabulary, gestures and gestures that might make one suspect that she/he is having sexual contact inappropriate for their age (especially in sexual violence).
Social and moral areaIn ICA it is essential to determine the family structure: description of the members, type of relationships and intrafamily roles, and position occupied by the CV. The social network should also be investigated: general viewpoint of the school, attitude and relationships with teachers and students, and relationships in contexts outside the school, such as parks, extracurricular activities and neighbourhoods.
Up to the age of 7, social networks will be extending, which is the criterion for the selection of friends and important people, physical closeness or material attributes offered. From the ages of 7–12 the relationship pattern changes significantly, and the most outstanding feature is reciprocity or bilateral cooperation.
In order to obtain data on this area, questions such as "How many people make up your family?", "How many people live at home?", "Can you draw your family?", "How do you behave at home?", "and how do they say you behave?", "What happens if you misbehave?", "What do you have to do to misbehave? To analyse the type of relationships between equals, phrases such as: "What school do you go to?", "Who is your teacher?", "What part of school do you like best?", "What do you like to play at at school?", "Do you have a friend?", "What do you do with your friends?" will be used.
At puberty the person begins to be autonomous in their moral principles and develops normative awareness. During preschool and school, a child’s obedience is linked to "reward-punishment" and their vision of the world has a polarised "good-bad" perspective. For this reason, statements on issues involving moral judgments should be assessed with caution.
Collection of the storyOne of the main objectives of forensic expertise in ICA is to achieve a thorough account of the events under investigation. The story, in the absence of other indicators of abuse, is an indispensable piece and may even be the only proof of charge. It should be handled with care, avoiding suggestive questions and taking the special vulnerability of the CV into consideration.
The existence of biases that could compromise the objectivity of the forensic report is a matter of concern among ICA experts.17 The main biases that hinder the collection of a reliable story are:
- •
External bias, derived from interference from adults close to the CV. It can condition an adult interpretation of the events. It is frequent in families that maintain crossed allegations due to custody dispute.
- •
Interpretation bias, it is essential to bear in mind that the quality and richness of the story is conditioned by the minor’s stage of maturity and communication skills (Table 1).
- •
Methodological bias, which we will avoid by systematising the interview (Tables 2 and 3).
The use of scales or tests will be determined by the age and communication ability of the CV.18–22 (Table 1). They require education and training for application and interpretation. In the preschool stage questionnaires are of very limited or no value. Some experts use graphic projective techniques that enable access to the CV’s internal content and help establish good rapport.23 These should be presented as a game and not as a work tool.
The most used graphic projective techniques include the human figure drawing test (HFDT), the family drawing test (Corman method) and the House-Tree-Person projective technique (John Buck). Projective/pictorial tests such as the Children's Apperception Test (CAT) use plates that need to be interpreted by the child.23–25
Among the most used instruments for behavioural assessment at school age are two scales that assess problem behaviours through data provided by parents: the Child Behaviour Checklist,26,27 which covers the last 6 months and the Weekly Behaviour Report,28,29 which assesses the last week. The Trauma Symptom Checklist- Alternative Version,30 useful from the age of 8, assesses the characteristic symptoms of post-traumatic stress disorder, anxiety and depression.
The usefulness of psychological tests in clinical practice is well established, whereas this does not apply in the field of expertise.19–21 The forensic value of projective evidence for self and hetero scales applied is highly controversial and has been questioned regarding its lack of methodological rigour and sufficient empirical evidence.23,31 The validity of human figure drawings is even more limited. Some authors generally recommend abstaining from applying these techniques in specifically forensic contexts.31
If used, projective techniques should be interpreted in a manner that is complementary and integrated with the examination and interview data, and their use should be limited to helping the child clarify and support his or her story. They should not be considered a diagnostic test, nor should they be considered unique indicators in the assessment of ICA.24
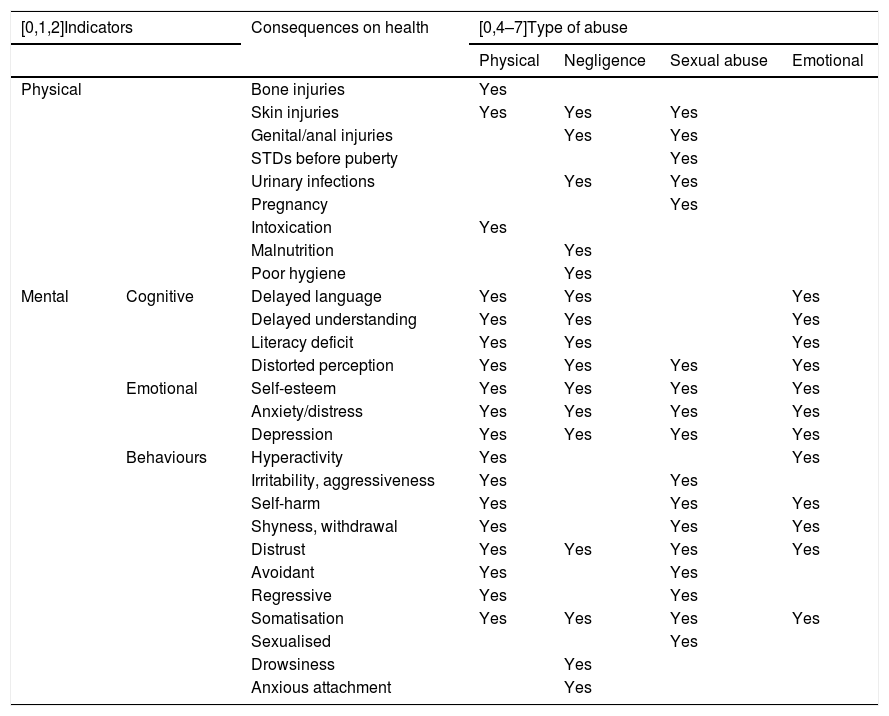
Analysis of indicators of intra-familial child abuseAnalysis of indicators from an expert point of view should be made with caution and with a global perspective. The indicators of risk and family and sociocultural protection that might have favoured violence within the family, child vulnerability factors and physical and psychological injuries detected in the victim will be taken into account (Table 4), which will be assessed as clinical indicators secondary to abuse. These indicators are characteristic and not specific, since they may be due to other causes.
Clinical, physical and mental characteristics of intrafamiliar child abuse.
| [0,1,2]Indicators | Consequences on health | [0,4–7]Type of abuse | ||||
|---|---|---|---|---|---|---|
| Physical | Negligence | Sexual abuse | Emotional | |||
| Physical | Bone injuries | Yes | ||||
| Skin injuries | Yes | Yes | Yes | |||
| Genital/anal injuries | Yes | Yes | ||||
| STDs before puberty | Yes | |||||
| Urinary infections | Yes | Yes | ||||
| Pregnancy | Yes | |||||
| Intoxication | Yes | |||||
| Malnutrition | Yes | |||||
| Poor hygiene | Yes | |||||
| Mental | Cognitive | Delayed language | Yes | Yes | Yes | |
| Delayed understanding | Yes | Yes | Yes | |||
| Literacy deficit | Yes | Yes | Yes | |||
| Distorted perception | Yes | Yes | Yes | Yes | ||
| Emotional | Self-esteem | Yes | Yes | Yes | Yes | |
| Anxiety/distress | Yes | Yes | Yes | Yes | ||
| Depression | Yes | Yes | Yes | Yes | ||
| Behaviours | Hyperactivity | Yes | Yes | |||
| Irritability, aggressiveness | Yes | Yes | ||||
| Self-harm | Yes | Yes | Yes | |||
| Shyness, withdrawal | Yes | Yes | Yes | |||
| Distrust | Yes | Yes | Yes | Yes | ||
| Avoidant | Yes | Yes | ||||
| Regressive | Yes | Yes | ||||
| Somatisation | Yes | Yes | Yes | Yes | ||
| Sexualised | Yes | |||||
| Drowsiness | Yes | |||||
| Anxious attachment | Yes | |||||
STDs: sexually transmitted diseases.
It is essential to analyse the family nucleus and the socio-cultural context in which the victim is being raised. Based on the premise that there are no demographic or family characteristics that exclude the possibility of ICA, it is possible to identify some indicators that are included in the comprehensive model of child abuse and that may facilitate abuse. This model differentiates between compensating (protection) and potentiating (risk and vulnerability) indicators.32,33
The main risk indicators for parents are socio-familial disharmony, a family history of abuse, skill shortages, mental illness, personality disorders, substance dependence and legal drug abuse.34 Indicators of vulnerability include disability from physical and/or mental illness, whether congenital or acquired, behavioural disorders, premature birth and unwanted children.
Indicators of psychological harmPsychological harm can be evidenced through heterogeneous symptoms affecting the cognitive, emotional or behavioural plane. Table 4 includes the most common clinical indicators. Their intensity varies according to the characteristics of the abuse (type, duration and frequency), of the family (psychiatric comorbidity, dysfunctional families, etc.), of the post-allegation socio-family support (age, subjective experience of the event and capacity to overcome the traumatic experience). A conditioning factor for resilience will be related with the cognitive attributions that the CV makes of the abuse suffered and the ability to cope with it.
Absence of psychological damage does not indicate absence of abuse. Between 25 % and 50 % of severely abused children are asymptomatic and have no emotional disturbances or psychiatric disorders at the time of assessment.5 In the case of child and preschool victims, the group of people who develop traumatic clinical symptoms is even smaller. On the other hand, the presence of associated psychological indicators in the literature on ICA in the expert-assessed child does not necessarily indicate that it corresponds to victimisation through ICA since there is no specific symptom of ICA and it may correspond to exposure to another psychological stressor.31 Even in sexual abuse it has been stated that there is overassessment when considering sexualised behaviours as an indicator of child sexual abuse.31 Determining the existence or otherwise of ICA cannot be inferred by the presence or absence of psychological symptoms (indicators), global and integrated assessment of all the findings is necessary.
The most frequent acute symptom in the period immediately following the abusive event is psychological distress, which is generally of short duration, although it can be maintained once the stressor has disappeared. After this distress, cognitive, emotional and behavioural changes may appear with greater or lesser intensity and duration. Sometimes these psychological changes are consolidated during childhood and can trigger child mental health disorders that can continue into adulthood.7,8
CV are at greater risk of behavioural, hyperactivity, attention, depression and attachment disorders. They are also at risk of developing behavioural disorders with academic problems and delinquency during adolescence. In cases of severe neglect during preschool age, emotional and cognitive development disorders can be triggered.7 In addition, we can find other psychopathologies such as post-traumatic stress disorder, acute stress disorder, adaptive disorder, disorder with somatic symptoms, separation anxiety disorder, reactive attachment disorder, uninhibited social relationship disorder, dissociative amnesia, regressions and phobias.7,8,17,35 There are differences according to gender, with girls more prone to internalisation disorders (depression, anxiety or isolation) and boys more prone to externalisation disorders (behavioural disturbances).
Socialisation disorders in adulthood and transgenerational violence are some of the noteworthy consequences that appear in the long term.36
Indicators of physical harmTraumatic injuries are rare and usually non-specific (Table 4). It is necessary to assess for delay in growth or motor development, relatively frequent in repeated ICA and neglect. The findings of complementary medical, toxicological and biological studies are of unquestionable value as objective elements in physical and sexual abuse. The importance must be stressed of early action to avoid losing physical or biological indices.
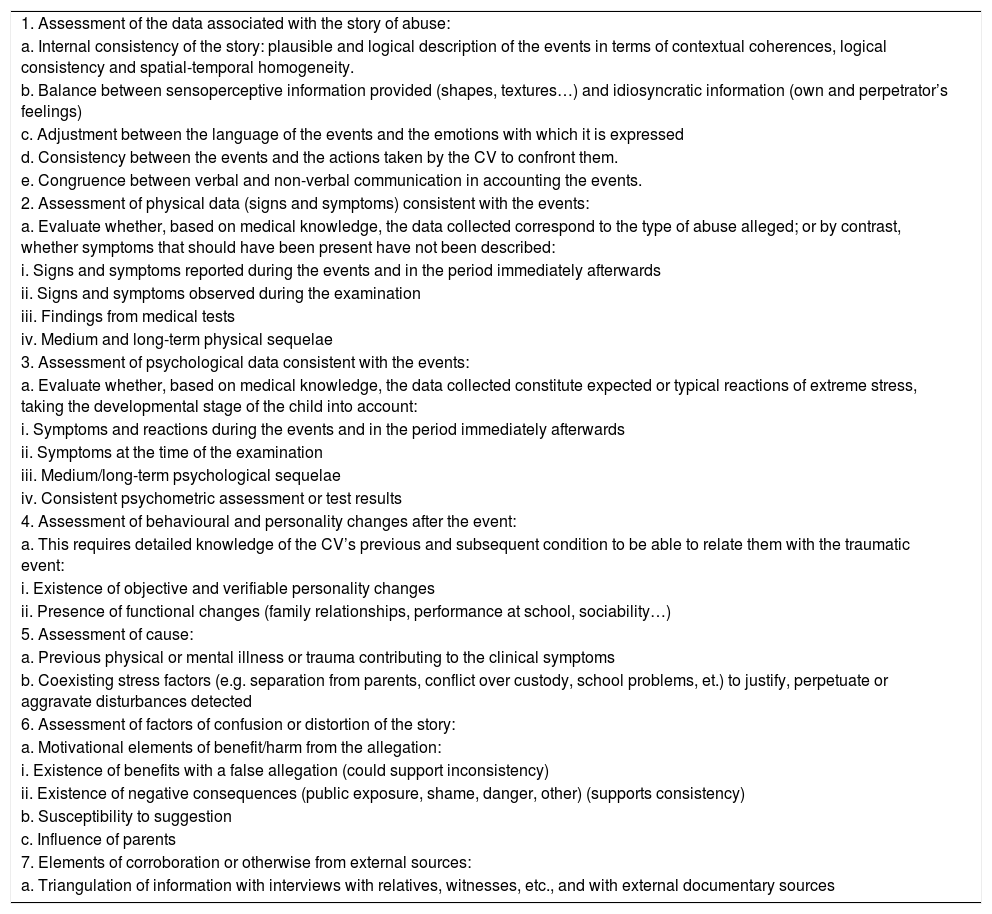
Causal link between events and damage. Analysis of credibilityOne of the most complex points in the assessment of ICA.37–39 Due to its complexity, a comprehensive and multidisciplinary assessment is essential, considering all available external sources of information. Table 5 lists the items to be analysed to conclude whether the findings are coherent, and to what extent, with what would be expected according to the story. The establishment of a causal link between psychological damage and victimisation requires in-depth analysis to detect the symptoms existing at the time of the events and the examination, the sequelae, the results of complementary tests, as well as the presence of behavioural and personality changes after the events. (Table 5).
Assessment of causality criteria and credibility analysis.
| 1. Assessment of the data associated with the story of abuse: |
| a. Internal consistency of the story: plausible and logical description of the events in terms of contextual coherences, logical consistency and spatial-temporal homogeneity. |
| b. Balance between sensoperceptive information provided (shapes, textures…) and idiosyncratic information (own and perpetrator’s feelings) |
| c. Adjustment between the language of the events and the emotions with which it is expressed |
| d. Consistency between the events and the actions taken by the CV to confront them. |
| e. Congruence between verbal and non-verbal communication in accounting the events. |
| 2. Assessment of physical data (signs and symptoms) consistent with the events: |
| a. Evaluate whether, based on medical knowledge, the data collected correspond to the type of abuse alleged; or by contrast, whether symptoms that should have been present have not been described: |
| i. Signs and symptoms reported during the events and in the period immediately afterwards |
| ii. Signs and symptoms observed during the examination |
| iii. Findings from medical tests |
| iv. Medium and long-term physical sequelae |
| 3. Assessment of psychological data consistent with the events: |
| a. Evaluate whether, based on medical knowledge, the data collected constitute expected or typical reactions of extreme stress, taking the developmental stage of the child into account: |
| i. Symptoms and reactions during the events and in the period immediately afterwards |
| ii. Symptoms at the time of the examination |
| iii. Medium/long-term psychological sequelae |
| iv. Consistent psychometric assessment or test results |
| 4. Assessment of behavioural and personality changes after the event: |
| a. This requires detailed knowledge of the CV’s previous and subsequent condition to be able to relate them with the traumatic event: |
| i. Existence of objective and verifiable personality changes |
| ii. Presence of functional changes (family relationships, performance at school, sociability…) |
| 5. Assessment of cause: |
| a. Previous physical or mental illness or trauma contributing to the clinical symptoms |
| b. Coexisting stress factors (e.g. separation from parents, conflict over custody, school problems, et.) to justify, perpetuate or aggravate disturbances detected |
| 6. Assessment of factors of confusion or distortion of the story: |
| a. Motivational elements of benefit/harm from the allegation: |
| i. Existence of benefits with a false allegation (could support inconsistency) |
| ii. Existence of negative consequences (public exposure, shame, danger, other) (supports consistency) |
| b. Susceptibility to suggestion |
| c. Influence of parents |
| 7. Elements of corroboration or otherwise from external sources: |
| a. Triangulation of information with interviews with relatives, witnesses, etc., and with external documentary sources |
CV: child victims.
The influence of distorting or confusing factors and the existence of other potential psychosocial stressors that may justify psychological harm should be investigated (Table 5). It is advisable to indicate the possibility of a monocausal link between abuse and injury.
It is a question of determining the existence of credibility criteria in the statements made by children with a history of abuse and determining falsibility criteria in those who have falsified or invented the statement. When there are no objective physical or biological indicators and the evidence gathered from external documentation sources is scarce or non-existent, analysis of the credibility of the testimony is a fundamental pillar in the investigation. In these cases, the interpretative and subjective risk of the expert is greater, and they should be particularly cautious in their conclusions.
The personal factors of the CV need to be considered that affect their capacity to accurately relate an experienced event: ability to communicate, intellectually, mnestically and linguistically; influence of the psychological treatment received; and resistance to external interference (suggestibility). Other variables that may affect the story are the delay between the abuse and the interview, multiple recovery (distortion of memory by repeatedly remembering abuse) and stress during the examination.39
The most used technique in the forensic context in credibility is the Statement Validity Assessment (SVA), which consists of an interview aimed at obtaining as extensive and accurate testimony as possible, analysis of the story under the Criterion Based Content Analysis (CBCA) reality criteria, and a validity list that weighs up external factors in the story.
The CBCA covers 19 criteria grouped in to five categories:
- 1
General characteristics: logical structure, unstructured production, quantity of details.
- 2
Specific contents: contextual embedding, descriptions of interactions, reproduction of conversation, unexpected complication during the incident.
- 3
Peculiarities of content: unusual details, superfluous details, accurately reported details misunderstood, related external associations, accounts of subjective mental state, attribution of perpetrator’s mental state.
- 4
Motivation-related contents: spontaneous corrections, admitting lack of memory, raising doubts about one’s own testimony, self-deprecation, pardoning the perpetrator.
- 5
Offence-specific elements: specific details.
This instrument was developed for the technical analysis of witness evidence in child sexual abuse and cannot be extrapolated to other population groups or other types of victims of non-sexual crimes, although it is used as a methodology to guide other types of abuse.
Recent studies have assessed the validity of the CBCA by studying the correlation coefficient among different experts who analysed statements of sexual abuse. The results are not completely homogeneous. One study concluded that the SVA is a robust method in the forensic setting, although it proposed improving some of the criteria.39 Another study concluded that its results were less convincing and proposed increasing the diagnostic accuracy of the CBCA by adding new criteria.38
Civil measuresThe General Council of the Judiciary40 advises that in cases where the family unit has been recognised by the UVIVG, the report should also conclude on the most appropriate regime of guardianship and custody and visits with the non-custodial parent. Therefore, a thorough analysis of the families and assessment of the wishes and real needs of the CV should be carried out, without establishing by default that shared custody is in their best interests. The real interest of the child is to have his/her opinion considered provided they have an adequate degree of maturity.
Medical-forensic reportThe report should contain the data of the intervening forensic team, the personal data of the CV and the methodology followed (information sources; examination model used and use of complementary tests). The relevant data for the judicial case should be indicated in the items of the examination of blocks 1, 2 and 3 (Table 2); as well as the type of physical and psychological harm suffered (Table 4), the need for treatment, the prospects of recovery and the possible causal link of the damage with the events reported.
Conclusions must be based on sound evidence since unprofessional expertise can cause irreparable harm to children and families. In addition to directly expert questions, appropriate therapeutic recommendations or protective measures for CV based on familiar structure must be included.
Please cite this article as: García-Martín R, Morentin B. Valoración forense integral del maltrato infantil intrafamiliar. Rev Esp Med Legal. 2020;46:28–40.