




To be able to prevent suicides. The exact magnitude of suicides must be known in order to prevent them. There is evidence that data provided on the number of suicides by the Spanish Statistical Office (Instituto Nacional de Estadística [INE]) differs from that identified by forensic pathologists. This paper aims to determine whether the INE data are the same as those recorded by the agencies responsible for conducting autopsies in Spain (IML), and to calculate the number of missing cases.
MethodIML was requested to provide the number of suicides in a 5-year period (2006–2010) and this was compared with those offered by INE in its site. A new rate of suicides per 100,000 was obtained and used to calculate the number of suicides in Spain.
ResultsFor every year of the studied period, the number of suicides reported by the INE was lower than that obtained directly from the IML. Using the highest annual suicide rate registered by province and the total number, a count was obtained of identified suicides that for some reason had not been recorded in the INE or the IML data. Based on these figures, the mean rate of suicides per 100,000 was 0.97 (SD 0.10) higher than official INE data, which indicates a mean loss of 443.86 (SD 46.72) cases reported each year. Possible factors that may influence the missing recorded cases are discussed.
ConclusionsAccording to the results, there is a discrepancy between INE and IML about the number of suicides in Spain. Neither of the two sources can be considered more reliable than the other.
Para poder prevenir el suicidio es necesario conocer su magnitud. Hay discrepancias entre las cifras de suicidios en estudios realizados con médicos forenses y las obtenidas a través del Instituto Nacional de Estadística (INE). Este trabajo pretende comprobar si los datos del INE coinciden o difieren con los registrados por los organismos encargados de la realización de autopsias médico-legales en España (Institutos de Medicina Legal [IML]).
MétodoSe solicitó a los directores de IML el número de suicidios en un periodo de 5 años (2006–2010) y se comparó con los ofrecidos por el INE en su sede virtual. Se calcularon las tasas de suicidio según ambas fuentes.
ResultadosEl número total de suicidios según el INE fue menor al obtenido directamente por los IML en todos los años. Con la cifra de suicidio registrado por provincia y año más alta, ya fuera de los IML o del INE, se obtuvo la cifra de casos de suicidio identificados (NSI) y que por algún motivo no quedaron registrados en una u otra entidad. Las cifras de NSI indicaban una tasa media de suicidios por 100.000 habitantes 0,97 (DE: 0,10) más alta que la que señalaba el INE, con una pérdida media de 443,86 (DE: 46,72) casos registrados cada año. Se discuten los posibles factores que influyen en esta pérdida de casos registrados.
ConclusionesSegún los resultados obtenidos, existe una discrepancia entre INE e IML sobre el número de suicidios en España sin que ninguna de las fuentes consultadas pueda considerarse más fiable.
Suicide is a global health problem and its prevention a priority for the World Health Organisation (WHO)1 and national health systems such as the Spanish one.2 According to official figures, suicide is the most frequent cause of non-natural death in Spain, ahead of traffic accidents.3 The magnitude of the problem of suicidal behaviour is a matter that worries both clinicians and researchers.4 One of the ways to ascertain the importance of suicide in a country is through the death figures by this cause. In Spain, this information comes from the official figures of the Spanish Statistics Office (Instituto Nacional de Estadística [INE]) since 1906.5 These data have been used in the recent study that deals with the relationship between the economic crisis in Spain and the number of suicides.6 This initial step is called into question by studies that indicate poor reliability of the official data in numerous countries.7
Knowing the exact number of suicide attempts or suicides is a complex task. The incidence of suicide attempts is usually calculated extrapolating from the data in a specific area and period, normally from emergency services. This was the method followed in a multicentre study instigated by the WHO that is still the key reference today when evaluating the figures for suicide attempts in Europe.8 However, this case collection methodology implicitly involves an underestimation of the real cases. To cite just an example, suicide attempts in which the person repents at the last moment and have not been seen by a third party rarely go to emergency services.
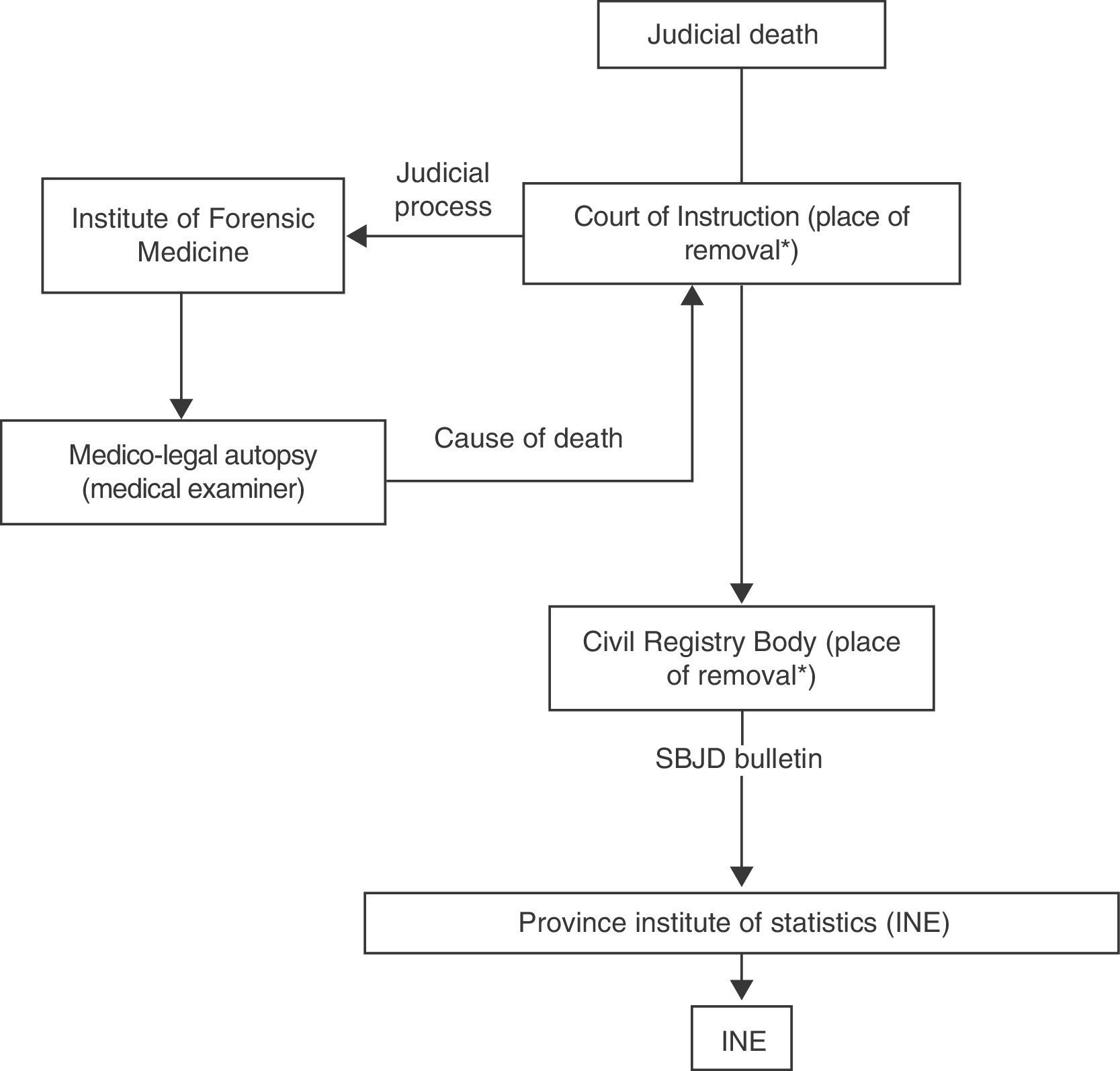
Insofar as suicide, identifying the number of cases would be easier a priori. This is true in countries in which a medico-legal autopsy has to be performed in all violent deaths or those involving suspicion of criminality, as is the case in Spain. However, this does not occur in many other countries, such as the Anglo-Saxon ones, in which the coroner establishes, without the need for an autopsy on some occasions, the cause of death. In Spain, when there is a violent death or one involving suspicion of criminality the body is recovered and examined, which requires the action of a legal commission composed of a judge, court registrar and medical examiner. We point out that the judge and court registrar work at the Court of Instruction for the legal jurisdiction in which the body has appeared, while medical examiners carry out their functions at the Institute of Forensic Medicine (Instituto de Medicina Legal [IML]) of the province or region in which the death is detected. (The exception is the Community of Madrid, where the system of medical examiner assignment is similar to that of judges and court registrars.) After an autopsy is performed, the medical examiner issues a “forensic autopsy” report establishing the nature of the death (natural or violent) and the medico-legal aetiology (suicide, homicide or accidental), submitting it to the Court of Instruction handling the case.
Independently and for civil purposes of registration of the death and for statistical reporting requirements, the Court of Instruction that initiates the investigation communicates the data provided by the medical examiner to the civil registry (civil registry offices [CRO]) of the municipality in whose municipal limits the cadaver is found; these offices are normally located in the magistrate's court or the town hall, in the absence of such a court. At the heads of legal jurisdictions, the CRO is usually assigned to one of the courts that constitute the jurisdiction. A civil servant in this CRO is the one responsible for compiling the Statistical Bulletin on Judicial Deaths (SBJD) (Boletín Estadístico de Defunción con Intervención Judicial)9 and sending it to the local branch of the Spanish Statistics Office, which includes the data in official records on suicide in Spain.
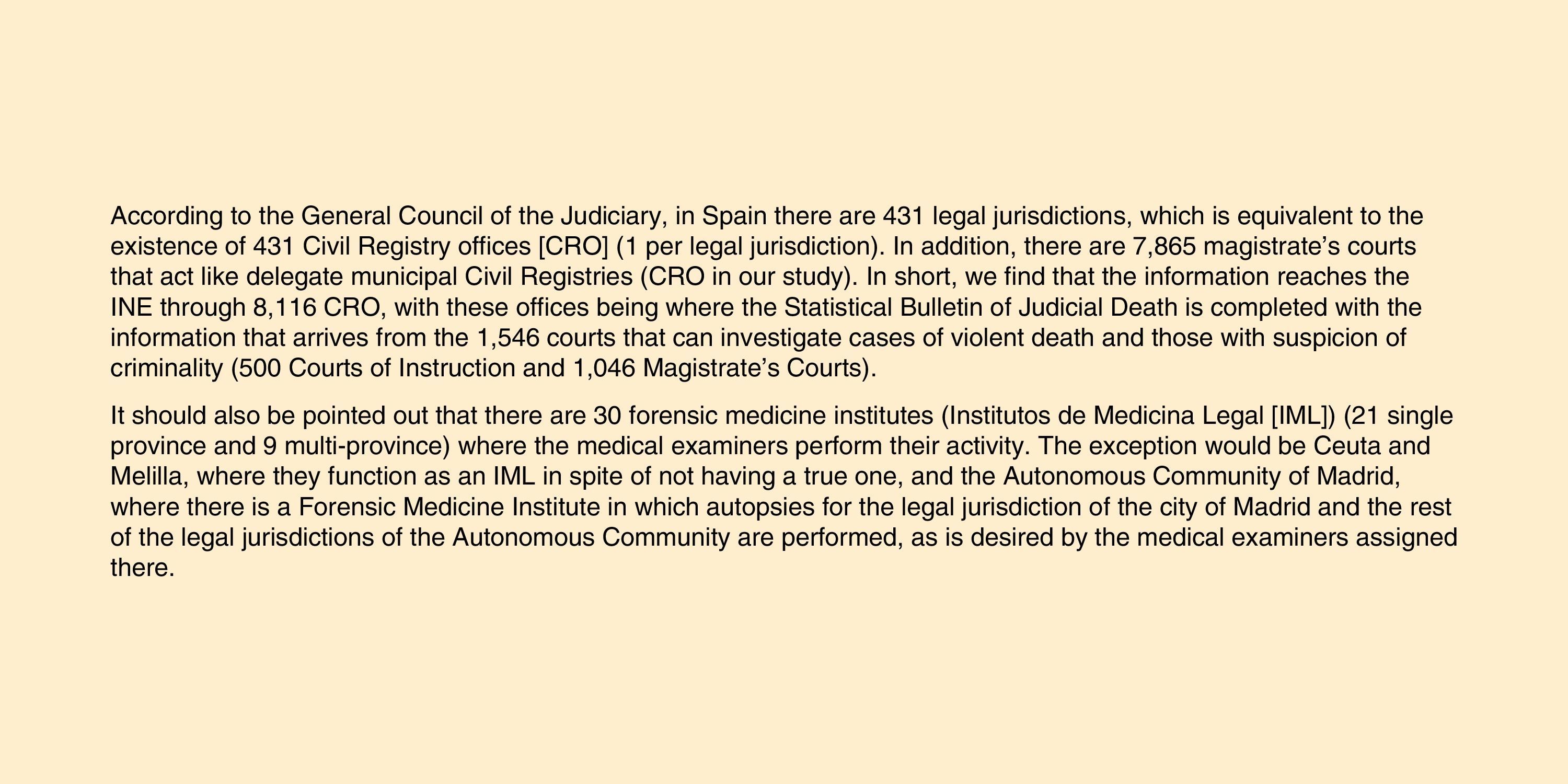
In short, it can be seen that the information is currently sent in Spain from 33 IML (including those in Madrid, Ceuta and Melilla with the exceptions that will be indicated later) to 1543 instruction or mixed courts, as appropriate, and from there to the 8093 CRO and then finally to the Spanish Statistics Office, or INE (Fig. 1). The last step is handled through the SBJD bulletin indicated previously; this is of special importance given that the INE results depend on the proper completion of the SBJD bulletin forms. The data in ‘Discussion’ section of this bulletin, “Cause of death”, are essential, to the extent that lack of information from the court will prevent the INE from carrying out its function appropriately. This information is found in the case documentation (cadaver removal report of medical examiner's report). However, there is no standard as to the data to be send to the CRO for compliance of their duties; given the great number of courts that send information and their organisation, it is easy for the information to arrive incomplete at its destination (Fig. 2).
. *Corresponding to the municipality where the cadaver is found.")
, including the Institute of Forensics for Madrid, Ceuta and Melilla; INE: Instituto Nacional de Estadística (Spanish Statistics Institute).")
Additionally, deaths from suicide are not always identifiable. There are cases of suicide by drowning, suicide through traffic accident, and even cases of death from drug or toxin overdose that are difficult to tell from accidental violent deaths. Other deaths with suicidal aetiology (such as hanging, firearms and weapons with blades) can be easier to identify at first from direct or indirect signs (for example, signs of struggle, defence wounds or from microscope examination of wound vitality). Consequently, establishing a death as a suicide has greater specificity than sensitivity; not all of the suicides that are produced are identified, but those identified as suicides are indeed so.
In spite of what has been indicated previously, there are studies in which, after obtaining the number of deaths by suicide through different IML, it did not coincide with the official figures offered by the INE. For example, Calvet-Roura et al.10 presented a descriptive study of completed suicide in the 2006–2009 period in the province of Girona, in which the data were obtained directly through the forensic medicine services (Servei de Medicina Forense) in that province. It was indicated in that study that there had been 269 deaths by suicide in the province of Girona in those 4 years, while the INE reported 215 for that same time period and place.
Our study attempted to analyse whether there were differences or not in the data collected in the IML and those reported by the INE.
MethodContact was established by telephone, e-mail and/or postal mail with the directors of the IML in Spain, as well as with the coordinating medical examiners in Ceuta and Melilla and the director of the Madrid forensic institute (from this point on, included generically as IML). In all, 33 sources were consulted to obtain the figures for deaths by suicide identified during 5 consecutive years (2006–2010). Suicide is a medico-legal diagnosis that forensic doctors give after studying the circumstances of the death and performing the autopsy. We compared these data with the official figures provided by INE and obtained through their webpage (www.ine.es). Consequently, the areas studied each year were those in which we obtained data from the IML and then we compared them with those that the INE offered in the same territory and year.
For the provinces that provided data for the IML, the number of suicides and the population figures (on 1 January of the year in question) were obtained through the INE webpage. With these figures, the suicide rates per 100,000 inhabitants according to the INE and according to the IML were calculated. The population of reference for the calculation differed slightly in the case of Madrid; the suicide rates calculated for the INE data included the total population of Madrid, while that calculated for the IML did not include the legal jurisdictions that did not perform autopsies in the Institute of Forensics.
As to registering the deaths, there is a possibility that, in both the INE and the IML, cases are lost during the registry process; however, deaths that are not suicides are unlikely to be registered as such. Based on this premise, it was considered that the highest number of suicides in a province and year would be the number of cases. This figure, which we called the number of province suicides identified (NPSI), could come from the IML or from the INE depending on the year and province. The sum of NPSI from the Spanish territory studied gave the total number of suicides identified (TNSI) and a new suicide rate. This rate, extrapolated to the total national territory, made it possible to calculate the minimum number of real suicides and compare it with the official figure.
The study was carried out following procedures in conformity with the ethical standards of the responsible committee for human experimentation and in agreement with the World Medical Association and the Declaration of Helsinki.
ResultsFrom the 33 IML or centres in charge of performing autopsies, 18 provided the data requested completely, 4 did so incompletely, 7 did not provide data of any years period and 4 did not reply. Among those that could not provide the data for all or part of the period requested, the main reason given was the lack of availability of a register of the causes of death per year or the absence of computer tools that would facilitate the task. In the specific case of Madrid, the register did not include the legal jurisdictions of Alcorcón (1 municipality), Coslada (3 municipalities), Colmenar Viejo (10 municipalities), Móstoles (5 municipalities) and Torrelaguna (42 municipalities).
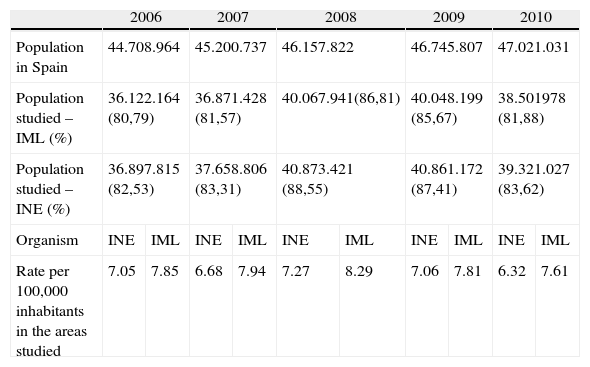
As the INE data were always available, the area and population studied would depend on the data for provinces provided by the IML. Consequently, in 2006, the population was 36,122,164 (80.79% of the population in Spain). For the calculation of rates with the INE data in this same year in the same provinces (with the exception that the 61 municipalities belonging to the legal jurisdictions of Madrid mentioned were included), the population under study was 36,897,815 (82.53%). In the successive years, the population studied with the IML was 81.57% in 2007; 86.80% in 2008; 85.67% in 2009; and 81.88% in 2010 (Table 1).
Number of suicides and rate by 100,000 inhabitants in the areas studied during the 2006–2010 period.
| 2006 | 2007 | 2008 | 2009 | 2010 | ||||||
| Population in Spain | 44.708.964 | 45.200.737 | 46.157.822 | 46.745.807 | 47.021.031 | |||||
| Population studied – IML (%) | 36.122.164 (80,79) | 36.871.428 (81,57) | 40.067.941(86,81) | 40.048.199 (85,67) | 38.501978 (81,88) | |||||
| Population studied – INE (%) | 36.897.815 (82,53) | 37.658.806 (83,31) | 40.873.421 (88,55) | 40.861.172 (87,41) | 39.321.027 (83,62) | |||||
| Organism | INE | IML | INE | IML | INE | IML | INE | IML | INE | IML |
| Rate per 100,000 inhabitants in the areas studied | 7.05 | 7.85 | 6.68 | 7.94 | 7.27 | 8.29 | 7.06 | 7.81 | 6.32 | 7.61 |
IML: Instituto de Medicina Legal (Medico-legal Institute), including the Institute of Forensics in Madrid, Ceuta and Melilla; INE: Instituto Nacional de Estadística (Spanish Statistics Institute).
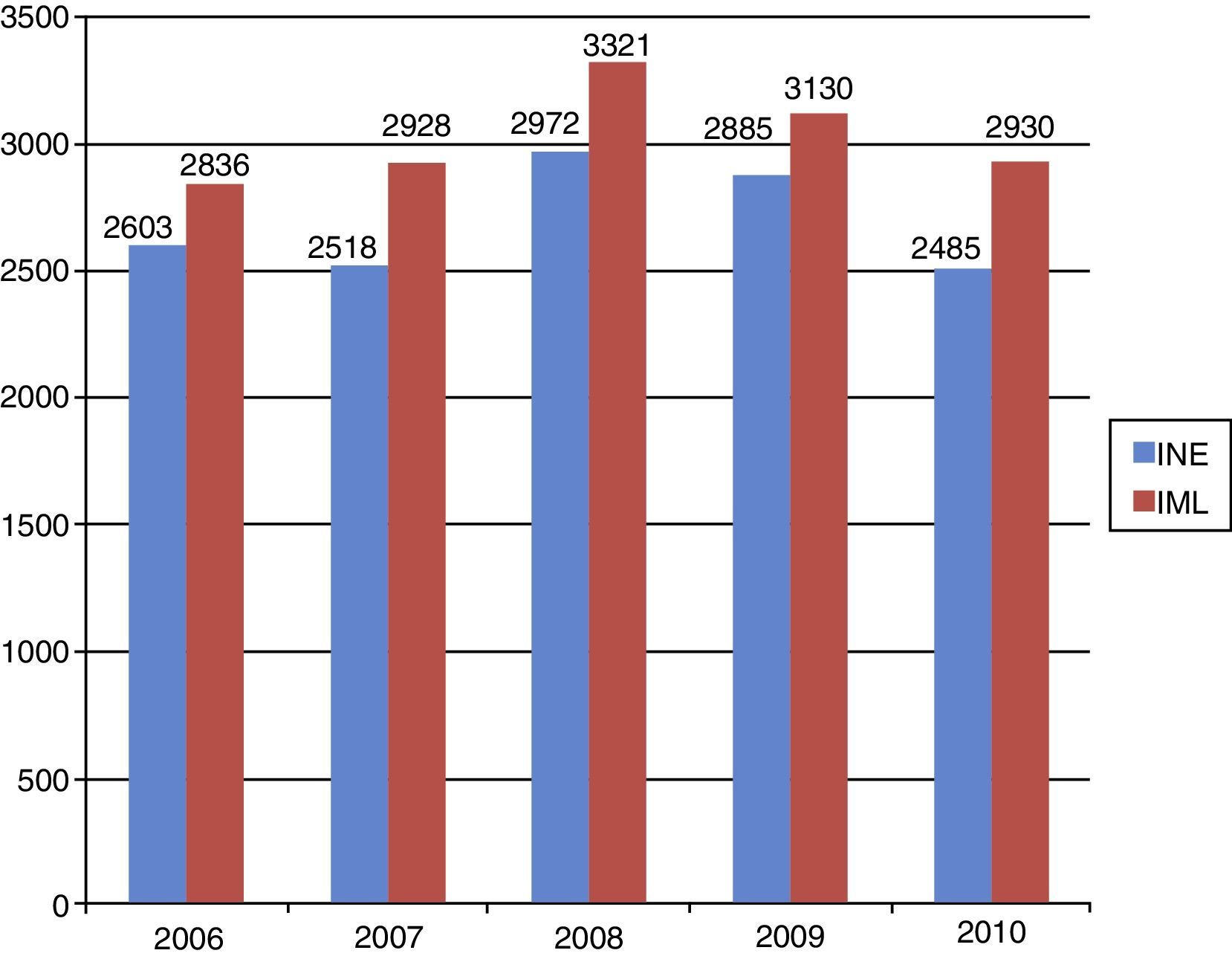
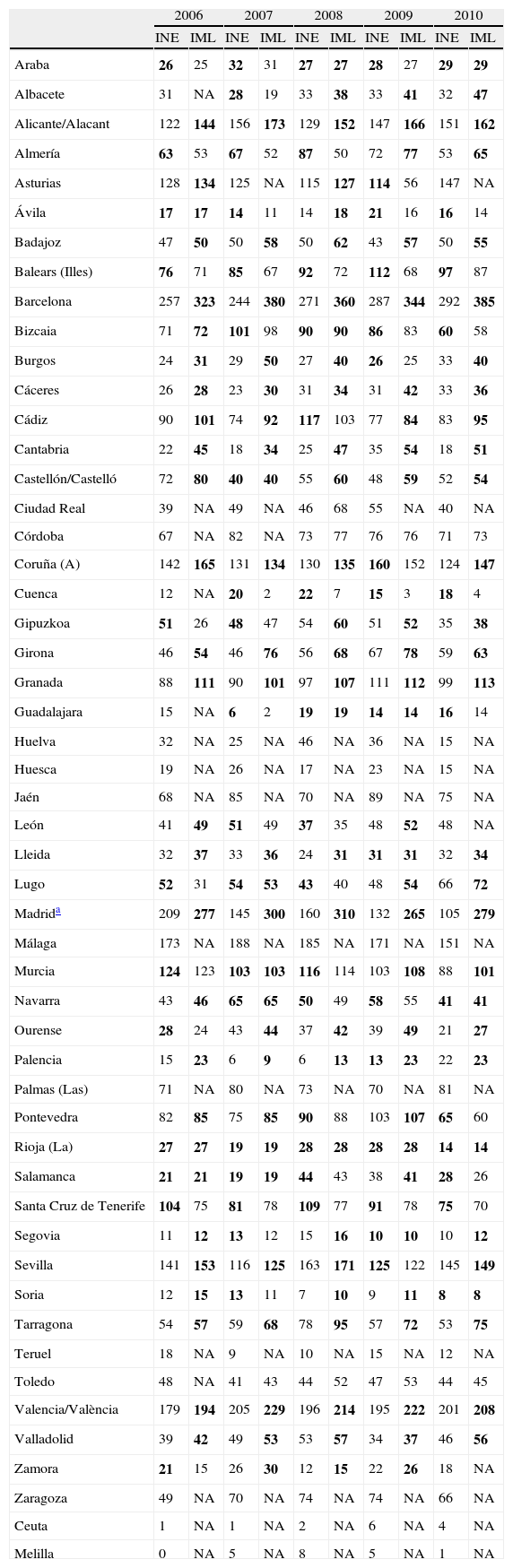
The number of suicides obtained through the INE and through the various IML differed in almost every province. They only agreed in 3 provinces in 2006, 4 in 2008 and 2010, and 5 in 2007 and 2009. It was only in La Rioja that the figures from the IML and INE coincided in every year studied. According to province and year, the figures were higher in the IML or in the INE (Table 2, indicated in bold type and equivalent to NPSI). The total number of suicides according to the IML in the areas in which the data were available from both organisations was higher than that indicated by the INE in all the years studied (Fig. 3). Likewise, the annual rates of suicide for the population studied were also higher than those calculated using the INE values (Table 1).
Number of suicides registered by province by the IML and by the INE.
| 2006 | 2007 | 2008 | 2009 | 2010 | ||||||
| INE | IML | INE | IML | INE | IML | INE | IML | INE | IML | |
| Araba | 26 | 25 | 32 | 31 | 27 | 27 | 28 | 27 | 29 | 29 |
| Albacete | 31 | NA | 28 | 19 | 33 | 38 | 33 | 41 | 32 | 47 |
| Alicante/Alacant | 122 | 144 | 156 | 173 | 129 | 152 | 147 | 166 | 151 | 162 |
| Almería | 63 | 53 | 67 | 52 | 87 | 50 | 72 | 77 | 53 | 65 |
| Asturias | 128 | 134 | 125 | NA | 115 | 127 | 114 | 56 | 147 | NA |
| Ávila | 17 | 17 | 14 | 11 | 14 | 18 | 21 | 16 | 16 | 14 |
| Badajoz | 47 | 50 | 50 | 58 | 50 | 62 | 43 | 57 | 50 | 55 |
| Balears (Illes) | 76 | 71 | 85 | 67 | 92 | 72 | 112 | 68 | 97 | 87 |
| Barcelona | 257 | 323 | 244 | 380 | 271 | 360 | 287 | 344 | 292 | 385 |
| Bizcaia | 71 | 72 | 101 | 98 | 90 | 90 | 86 | 83 | 60 | 58 |
| Burgos | 24 | 31 | 29 | 50 | 27 | 40 | 26 | 25 | 33 | 40 |
| Cáceres | 26 | 28 | 23 | 30 | 31 | 34 | 31 | 42 | 33 | 36 |
| Cádiz | 90 | 101 | 74 | 92 | 117 | 103 | 77 | 84 | 83 | 95 |
| Cantabria | 22 | 45 | 18 | 34 | 25 | 47 | 35 | 54 | 18 | 51 |
| Castellón/Castelló | 72 | 80 | 40 | 40 | 55 | 60 | 48 | 59 | 52 | 54 |
| Ciudad Real | 39 | NA | 49 | NA | 46 | 68 | 55 | NA | 40 | NA |
| Córdoba | 67 | NA | 82 | NA | 73 | 77 | 76 | 76 | 71 | 73 |
| Coruña (A) | 142 | 165 | 131 | 134 | 130 | 135 | 160 | 152 | 124 | 147 |
| Cuenca | 12 | NA | 20 | 2 | 22 | 7 | 15 | 3 | 18 | 4 |
| Gipuzkoa | 51 | 26 | 48 | 47 | 54 | 60 | 51 | 52 | 35 | 38 |
| Girona | 46 | 54 | 46 | 76 | 56 | 68 | 67 | 78 | 59 | 63 |
| Granada | 88 | 111 | 90 | 101 | 97 | 107 | 111 | 112 | 99 | 113 |
| Guadalajara | 15 | NA | 6 | 2 | 19 | 19 | 14 | 14 | 16 | 14 |
| Huelva | 32 | NA | 25 | NA | 46 | NA | 36 | NA | 15 | NA |
| Huesca | 19 | NA | 26 | NA | 17 | NA | 23 | NA | 15 | NA |
| Jaén | 68 | NA | 85 | NA | 70 | NA | 89 | NA | 75 | NA |
| León | 41 | 49 | 51 | 49 | 37 | 35 | 48 | 52 | 48 | NA |
| Lleida | 32 | 37 | 33 | 36 | 24 | 31 | 31 | 31 | 32 | 34 |
| Lugo | 52 | 31 | 54 | 53 | 43 | 40 | 48 | 54 | 66 | 72 |
| Madrida | 209 | 277 | 145 | 300 | 160 | 310 | 132 | 265 | 105 | 279 |
| Málaga | 173 | NA | 188 | NA | 185 | NA | 171 | NA | 151 | NA |
| Murcia | 124 | 123 | 103 | 103 | 116 | 114 | 103 | 108 | 88 | 101 |
| Navarra | 43 | 46 | 65 | 65 | 50 | 49 | 58 | 55 | 41 | 41 |
| Ourense | 28 | 24 | 43 | 44 | 37 | 42 | 39 | 49 | 21 | 27 |
| Palencia | 15 | 23 | 6 | 9 | 6 | 13 | 13 | 23 | 22 | 23 |
| Palmas (Las) | 71 | NA | 80 | NA | 73 | NA | 70 | NA | 81 | NA |
| Pontevedra | 82 | 85 | 75 | 85 | 90 | 88 | 103 | 107 | 65 | 60 |
| Rioja (La) | 27 | 27 | 19 | 19 | 28 | 28 | 28 | 28 | 14 | 14 |
| Salamanca | 21 | 21 | 19 | 19 | 44 | 43 | 38 | 41 | 28 | 26 |
| Santa Cruz de Tenerife | 104 | 75 | 81 | 78 | 109 | 77 | 91 | 78 | 75 | 70 |
| Segovia | 11 | 12 | 13 | 12 | 15 | 16 | 10 | 10 | 10 | 12 |
| Sevilla | 141 | 153 | 116 | 125 | 163 | 171 | 125 | 122 | 145 | 149 |
| Soria | 12 | 15 | 13 | 11 | 7 | 10 | 9 | 11 | 8 | 8 |
| Tarragona | 54 | 57 | 59 | 68 | 78 | 95 | 57 | 72 | 53 | 75 |
| Teruel | 18 | NA | 9 | NA | 10 | NA | 15 | NA | 12 | NA |
| Toledo | 48 | NA | 41 | 43 | 44 | 52 | 47 | 53 | 44 | 45 |
| Valencia/València | 179 | 194 | 205 | 229 | 196 | 214 | 195 | 222 | 201 | 208 |
| Valladolid | 39 | 42 | 49 | 53 | 53 | 57 | 34 | 37 | 46 | 56 |
| Zamora | 21 | 15 | 26 | 30 | 12 | 15 | 22 | 26 | 18 | NA |
| Zaragoza | 49 | NA | 70 | NA | 74 | NA | 74 | NA | 66 | NA |
| Ceuta | 1 | NA | 1 | NA | 2 | NA | 6 | NA | 4 | NA |
| Melilla | 0 | NA | 5 | NA | 8 | NA | 5 | NA | 1 | NA |
IML: Instituto de Medicina Legal (Medico-legal Institute), including the Institute of Forensics for Madrid, Ceuta and Melilla); INE: Instituto Nacional de Estadística (Spanish Statistics Institute); NA: data not available.
The number of province-identified suicide is indicated in bold.
, including the Institute of Forensics in Madrid, Ceuta and Melilla; INE: Instituto Nacional de Estadística (Spanish Statistics Institute).")
Total number of suicides registered by the INE and by the IML that took place in the study area by years. IML: Instituto de Medicina Legal (Medico-Legal Institute), including the Institute of Forensics in Madrid, Ceuta and Melilla; INE: Instituto Nacional de Estadística (Spanish Statistics Institute).
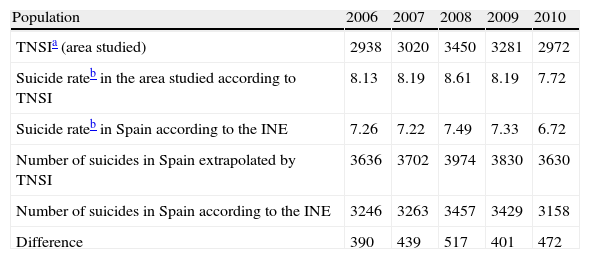
To calculate TNSI, we took into consideration (as has been mentioned) that in the registers of both the INE and the IML data could be lost, but that it was highly unlikely that non-existent cases of suicide would be registered. We consequently calculated TNSI for each year bearing this in mind (Table 3). These results show suicide rates above those calculated using only INE data, with a mean difference in this period of 0.97 (SD: 0.10). This would represent a mean loss of at least 443.86 (SD: 46.72) registered cases each year.
Number of suicides identified, suicide rates and number of suicides extrapolated to the entire national territory calculated by years.
| Population | 2006 | 2007 | 2008 | 2009 | 2010 |
| TNSIa (area studied) | 2938 | 3020 | 3450 | 3281 | 2972 |
| Suicide rateb in the area studied according to TNSI | 8.13 | 8.19 | 8.61 | 8.19 | 7.72 |
| Suicide rateb in Spain according to the INE | 7.26 | 7.22 | 7.49 | 7.33 | 6.72 |
| Number of suicides in Spain extrapolated by TNSI | 3636 | 3702 | 3974 | 3830 | 3630 |
| Number of suicides in Spain according to the INE | 3246 | 3263 | 3457 | 3429 | 3158 |
| Difference | 390 | 439 | 517 | 401 | 472 |
INE: Instituto Nacional de Estadística (Spanish Statistics Institute); TNSI: total number of suicides identified.
The figures for suicides registered obtained from the IML or through the INE matched in almost none of the years and provinces. This is very worrying given the importance that knowing the real magnitude of suicide in Spain has. The difference in the number of suicides registered by the INE or by the IML varies every year. In addition, the greater number of cases is not for one or the other organism consistently, but they alternate. Consequently, the same IML can register more suicide cases than the INE in a province in a year and then be the opposite the next year. These differences can reach up to 174 cases, as it occurred in the province of Madrid, which are additionally not included in their entirety. Such disparate figures make us raise the question of the reason for this discrepancy in the register of suicides. It might be partially due to the fact that, in the case of violent deaths, when they are added to the Civil Registry, the aetiology has not been established and the cause is waiting to be determined by tests of a toxicological or other nature. However, these cases in themselves do not justify the divergence found. Other factors have to be considered, such as the intricate path through which the information flows from the time it is obtained by the medical examiner until the data are entered into the CRO. We understand that the important number of individuals that are involved in the entire process (medical examiner, personnel at the Court of Instruction, workers at the Civil Registries, staff at the INE) can cause a progressive loss of information from its origin to its final destination.
As has been mentioned, and as Farmer indicated, the number of deaths identified and classified as suicides are, necessarily, fewer than the real ones for different reasons11: (1) Criteria of the definition of suicide: consequently, there is the possibility of classifying a death as indeterminate in some countries but not in others. Specifically, in Spain, the definitive report that the medical examiner issues at the petition of the court that handles the case of the death establishes the nature of the death (natural or violent) as well as its aetiology (accidental, homicide or suicide). There are situations in which the aetiological diagnosis of the death cannot be issued until the results of complementary tests, so the report can be considered as indeterminate, waiting for the test results that will change that report to definitive. (2) The need to confirm the subject's intentionality: determining the intention of a deceased person is difficult. This intentionality is important in cases in which it could be mistaken for an accidental death and in which there were no witnesses. In a suicide by drowning, the person might have fallen in the water accidentally, or by falling from a building. The same is true in the case of a traffic accident in which the driver might have had a period of unconsciousness or something similar that provoked lack of control of the vehicle. Schmidt et al. indicated that only 1.7% of the deaths resulting from traffic were considered suicides in a 6-year period.12 Other suicides use less violent methods, such as chronically-ill patients in which taking more or less of the prescribed medication can have fatal consequences.13 (3) Attitudes towards suicide: these can be cultural and/or religious or even economic for the insurance policies that the deceased individual could have signed. For these reasons, when faced with cases in which the aetiology of the death raises doubts, accidental death is usually chosen as the cause, because it involves fewer psychological consequences for the family and less social sigma,14 to which we could add the economic results according to the insurance that the deceased might have. It is important to know these facts when estimating that the magnitude of the problem of suicide is even greater that what we can appreciate by knowing the figures of suicide registered officially.
However, this discrepancy between the figures of suicide published in the INE and those collected by the different IML studied has nothing to do with what we have just mentioned, relating to the diagnosis of suicide and not to registering the cases already identified as such. Even though the causes of these differences remain unclear, what is evident is that the current system of collecting the causes of death is not efficient or reliable. The longer the chain of information collection is, the greater the possibility of error. It is not the objective of this study, but there is a possibility that the accounting for other types of death, whether natural or violent, also contains errors, with discrepancies between the classified cases and the real ones.
This finding is important in being able to ascertain the real problem that suicide represents in Spain and the position that it occupies among other countries. The official figures put Spain among the countries with the lowest suicide rates in the European Union. This is backed by a lower prevalence of suicidal ideation, suicide planning and suicide attempts in the Spanish population in comparison to other countries.8,15 Cantor16 proposed dividing Europe into 4 zones according to similarity in the tendency of the annual suicide figures. These areas would be southern Europe (Greece, Portugal, Italy and Spain), western Europe Occidental (Austria, Belgium, France, Germany, Holland and Switzerland), Scandinavia (Denmark, Finland, Norway and Sweden) and, lastly, what are called Old World Anglo-Saxons (the United Kingdom and Ireland).
Faced with these results and the possibility that the data from the INE and the IML concerning suicide and other causes of death are erroneous, we propose what happens in non-judicial deaths (neither violent nor with suspicion of criminality) as a solution. In those cases, with the medical certificate of cause of death, the INE form is attached for completion, with both documents signed by the physician that knows the cause of death.
In our case of judicial deaths, the proposal consists of having the person in charge of filling in all the information corresponding to ‘Discussion’ section of the SBJD bulletin (“Causes of death”) be the medical examiner responsible for performing the autopsy and, consequently, determining the medico-legal diagnosis. This person is the one who possesses the capacity and knowledge needed about everything that happened in the death of a person, so this person is the one who informs the Court of Instruction to investigate the death. By extension, this would be the ideal individual to provide the death-related data that are of interest for the SBJD bulletin. In this way, the information about the cause of death would arrive from the origin (IML) to the INE through the Court of Instruction or directly; consequently, the only thing that would change from the current process is who would fill in the data in a section of the SBJD bulletin and it would be more similar to what is done in natural deaths with a medical certificate.
LimitationsThe entire national territory was not included in this study, although data from a very high percentage of it were obtained. Likewise, the TNSI figures are an approximation from the minimum figures of suicide in Spain, assuming that the greatest numbers per province and per year are of existing cases. As for the province of Madrid, the figures with which we analysed the INE figures are not the same as those of the Institute of Forensics. Consequently, the figures for this autonomous community are not comparable. However, the difference in population does not seem to affect data distortion; in fact, it indicates the need to optimise the reporting of suicides.
ConclusionsBased on the results obtained, there is a discrepancy between the official data offered by the INE about suicides in Spain and those obtained directly through those responsible for performing autopsies on suicide cases, the medical examiners in the IML. In general, the number of suicides was greater in the IML compared with the INE. However, the figures per province and year were not greater systematically in either of the 2 organisms, so it does not seem that the IML are presently a reliable source in the registering of cases. From the results obtained, everything seems to indicate that the figures for identifiable suicide cases, if not those of real suicides, are higher than what the INE has been indicating. The INE's lack of reliability in registering suicides may be due to the fact that the individual responsible for filling in the data that should be sent to the INE has not got sufficient data, given that they are sent by the Court of Instruction. This situation could be changed and could be more reliable if the person responsible for completing the forms with the data related to deaths with judicial intervention was the same medical examiner who prepared the autopsy report and sends it to the Court of Instruction.
Ethical responsibilitiesProtection of people and animalsThe authors state that no experiments were performed on human being or on animals for this research.
Data confidentialityThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
We thank the following IML directors and IML coordinators, who carried out this function in July–August 2012, and for providing the data that made this study possible: Joaquín Garijo (IML Albacete, Cuenca and Guadalajara), Juan José Payo (IML Alicante), Laura Márquez (IML Almería), Antonia Martínez (IML Asturias), Enrique Mendoza (IML Badajoz), Vidal Santos (IML Baleares), José Amador Martínez (IML Ávila, Burgos, Segovia and Soria), Mercedes González Salinas (IML Cádiz), José María Montero (IML Cáceres), Pilar Guillén (IML Cantabria), Mario Ventura (IML Castellón), Jordi Medallo (IML Cataluña), María del Carmen Martín (IML Ciudad Real and Toledo), José Sáez (IML Córdoba), Gilberto Giménez (IML Granada), Benito López de Abajo. (IML Galicia), Jorge González (IML La Rioja), Mariano de la Torre (IML León and Zamora), Eduardo Andreu (Instituto Anatómico Forense de Madrid), Rafael Bañón (IML Murcia), Rafael Teijeira (IML Navarra), Carlos Cubero (IML País Vasco), María Victoria García (IML Palencia, Salamanca and Valladolid), Jesús Parejo (IML Sevilla), Jesús Vega (IML Tenerife) and Vicente Matías (IML Valencia); and to the coordinating medical examiners Leticia Alonso (coordinator of Melilla) and Ángel Macías (coordinator of Ceuta). Likewise, we thank the civil servants of the Civil Registry in Sevilla and the Magistrate's Court in Mairena del Aljarafe (Sevilla) for clearing up the itinerary that the registry of deaths from suicide follow at present. In addition, we are grateful to Antonia Rodríguez and Samuel Aidan Kelly for their critical appraisal and help with writing this article and to the Consortium for Excellence in Forensic Research in Andalucia (abbreviated CEIFA in Spanish) for their collaboration in the research into suicidal behaviour.
Please cite this article as: Giner L, Guija JA. Número de suicidios en España: diferencias entre los datos del Instituto Nacional de Estadística y los aportados por los Institutos de Medicina Legal. Rev Psiquiatr Salud Ment (Barc). 2014;7:139–146.