





We used data from the Global Burden of Disease, Injuries, and Risk Factors Study 2010 to report on the burden of neuropsychiatric disorders in Spain.
Materials and methodsThe summary measure of burden used in the study was the disability-adjusted life-year (DALY), which sums of the years of life lost due to premature mortality (YLLs) and the years lived with disability (YLDs). DALYs were adjusted for comorbidity and estimated with 95% uncertainty intervals.
ResultsThe burden of neuropsychiatric disorders accounted for 18.4% of total all-cause DALYs generated in Spain for 2010. Within this group, the top five leading causes of DALYs were: depressive disorders, Alzheimer's disease, migraine, substance-use disorders, and anxiety disorder, which accounted for 70.9% of all DALYs due to neuropsychiatric disorders. Neurological disorders represented 5.03% of total all cause YLLs, whereas mental and substance-use disorders accounted for 0.8%. Mental and substance-use disorders accounted for 22.4% of total YLDs, with depression being the most disabling disorder. Neurological disorders represented 8.3% of total YLDs.
ConclusionsNeuropsychiatric disorders were one of the leading causes of disability in 2010. This finding contributes to our understanding of the burden of neuropsychiatric disorders in the Spanish population and highlights the importance of prioritising neuropsychiatric disorders in the Spanish public health system.
Se analizaron los datos españoles relacionados con los trastornos neurológicos, mentales y por consumo de sustancias procedentes del estudio Global Burden of Diseases (GBD 2010), Injuries and Risk Factors.
Materiales y métodosSe calcularon los años de vida ajustados por discapacidad (AVAD), que son el resultado de la combinación de los años de vida perdidos por mortalidad prematura (AVP) y los años vividos con discapacidad (AVD). Los AVAD se ajustaron por comorbilidad y se estimaron con intervalos de confianza del 95%.
ResultadosLa carga de los trastornos neuropsiquiátricos supuso el 18,4% del total de AVAD generados en España en 2010. Dentro de este grupo, las 5 causas principales de AVAD fueron: depresión, enfermedad de Alzheimer, migrañas, trastornos por consumo de sustancias y trastornos de ansiedad, que representaron el 70,9% del total de los trastornos neuropsiquiátricos. Los trastornos neurológicos supusieron el 5,03% del total de AVP, mientras que los trastornos mentales y por consumo de sustancias representaron el 0,8%. Los trastornos mentales y por consumo de sustancias constituyeron el 22,4% del total de AVD, siendo la depresión la enfermedad más incapacitante. Por otra parte, los trastornos neurológicos sumaron el 8,3% del total de AVD.
ConclusionesLos trastornos neuropsiquiátricos fueron en España una de las principales causas de discapacidad en 2010. Este estudio contribuye al entendimiento de la carga que suponen dichos trastornos en la población española y pone de manifiesto la necesidad de dar prioridad a los trastornos neuropsiquiátricos en la sanidad pública española.
The Global Burden of Disease, Injuries, and Risk Factors Study (the GBD study), led by Murray and Lopez, was initially conducted in 1990.1 This study was the first large-scale, systematic effort to provide a comparable assessment of health loss due to diseases and injuries at both global and regional levels. In the GBD framework, the summary measure of disease burden is the disability-adjusted life-year (DALYs), which sums years of life lost due to premature mortality (YLLs) and years lived with disability (YLDs) due to a particular disease.2 One DALY represents the loss of 1 year of full health. By combining YLLs and YLDs, DALYs facilitated the comparison of the burden of diseases and injuries that cause early death as well as those that cause disability, an approach that was ground-breaking in that it was able for the first time to highlight neuropsychiatric disorders (a disease category including neurological, mental and substance-use disorders) as leading causes of disease burden.
Notable key findings emerging from the 1990 study were that neuropsychiatric disorders accounted for more than 25% of global YLDs with 5 of the top 10 causes of disability included within the neuropsychiatric category (unipolar major depression, alcohol use, bipolar disorder, schizophrenia and obsessive–compulsive disorders). Depression was the leading cause of YLDs while dementia was associated with high rates of both YLDs and YLLs.3–6
Investigations of prevalence within Europe also highlight mental and neurological disorders as a highly impacting group of disorders.7–10 For instance, in Spain, data from the EseMed study reported a lifetime prevalence of mental disorders of 19.5%.7 According to the National Institute of Statistics,11 neurological disorders were the fourth leading cause of death in Spain for 2012. Murray and colleagues estimated that, in 2020, the overall proportion of neuropsychiatric disorders will be 14.7% worldwide.4 Similarly, the World Health Organisation estimated an increase of 15%,12 although in both instances, estimates were derived using data projections from previous years.
In 2007, a new Global Burden of Disease study (GBD 2010) was carried out and published in late 2012. Remarkable improvements in methodology were introduced to overcome limitations from the previous 1990 study, such as the use of population-based surveys to calculate disability weights which had been previously derived from expert consensus and the estimation of 95% uncertainty around all burden estimates.13 GBD 2010 also expanded on the set of neuropsychiatric disorders investigated. New categories (e.g. pervasive developmental disorders, childhood behavioural disorders) were included and existing categories were expanded (e.g., unipolar depression was divided into major depressive disorder and dysthymia; drug use disorders were divided into cocaine, cannabis, opioid and amphetamine dependence). Changes in methodology between the 1990 GBD study and its most recent iteration (GBD 2010) have been summarised in greater detail elsewhere.6,14,15 As these changes in methodology invalidated any comparison of burden estimates between the two studies, GBD 2010 estimated burden for both 1990 and 2010 to facilitate the investigation of burden across time.16
GBD 2010 findings highlighted that nine of the top 20 causes of disability were included within the neuropsychiatric category (e.g. depression, anxiety disorders, migraine, drug use disorders). Shifts in population growth and ageing due to increases in life expectancy also meant that more of the world's population were living to the age when neuropsychiatric disorders are most prevalent.14,17 Although GBD 2010 global findings for neuropsychiatric disorders has been previously reported,6,14 it is also important to present on the trends in burden at a national level. Knowledge of differences in burden at the country level is needed for priority setting in national health agendas and the development of health policies that address age, sex and year specific trends in burden and their impact on national health systems.
In this paper, we aim to report on the burden of neuropsychiatric disorders in Spain, for 1990 and 2010. To the best of our knowledge, this is the first study reporting on the burden of neuropsychiatric disorders in Spain using data from the GBD 2010 study.
Materials and methodsThe GBD 2010 study involved a comprehensive assessment of burden for 291 diseases and injuries, and 67 risk factors for 20 age groups in 187 countries distributed across 21 world regions.2,13–15 Burden was assessed in terms of YLLs, YLDs and DALYs. Information about GBD 2010 definitions and methods will be briefly summarised here as they have been described in detail elsewhere.13–15
In this paper, Spanish outcomes with respect to neuropsychiatric disorders are presented. Neuropsychiatric disorders were made up of neurological, mental and substance-use disorders, defined using the Diagnostic and Statistical Manual of Mental Disorders18 and the International Classification of Diseases.19 More specifically, neurological disorders included: Alzheimer's disease and others dementias, Parkinson's disease, epilepsy, multiple sclerosis, migraine, tension-type headache. Mental and substance-use disorders were made up of schizophrenia, alcohol, opioid, cocaine, amphetamine, and cannabis dependence, depressive disorders (major depressive disorder and dysthymia), bipolar disorder, anxiety disorders, eating disorders, pervasive developmental disorders (autism, Asperger's syndrome), childhood behavioural disorders (attention-deficit hyperactivity disorder, conduct disorder), idiopathic intellectual disability; and for disorders for which there was insufficient data to be assessed individually, three residual groups of other neuropsychiatric disorders were included.14
Years lost due to premature mortality (YLLs)YLLs were calculated by multiplying the number of deaths attributable to a given disease by the standard life expectancy at the age of death for the Spanish population. Data on standard life expectancy came from standard model life tables derived specifically for GBD 2010.12 Estimates of death came from comprehensive reviews of vital registrations, verbal autopsy, mortality surveillance databases, and other sources dating back to 1980, for each of the 187 countries included in GBD 2010. Deaths could only be attributed to neuropsychiatric disorders when the disorder was considered as the direct cause of death following ICD-10 guidelines.15,16,20 Based on this, deaths and YLLs were presented specifically for schizophrenia, alcohol-use disorders, drug-use disorders, anorexia nervosa, Alzheimer's disease, Parkinson's disease, multiple sclerosis, epilepsy and the residual groups of other neuropsychiatric disorders.
Years lived with disability (YLDs)Systematic reviews of the published and unpublished literature were conducted to determine the global prevalence, incidence, remission, and excess-mortality associated with each disorder.16 The case definition for each disorder followed criteria proposed by the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV)18 or the International Classification of diseases (ICD-10).19 Neuropsychiatric disorders were included in the study when there was sufficient epidemiological information to generate defensible nationally representative epidemiological estimates by age, sex and year. Although data on the prevalence of neuropsychiatric disorders were available for many countries, they were typically incomplete (e.g. not stratified by age, sex or year) and there was very little available on the incidence, remission and excess-mortality of these disorders. For that reason, DisMod-MR (Disease Modelling Meta-Regression), a Bayesian meta-regression tool, was used to reproduce for each disorder, from the raw epidemiological data that were available, consistent estimates of prevalence, incidence, remission and excess-mortality for all age, sex, country, and year groups.14,16 Uncertainty intervals (UIs) were also propagated from the raw epidemiological estimates to the final modelled output.21
YLDs were computed as the prevalence of a given disorder multiplied by the average disability weight for that disorder. In GBD 2010 a total of 1160 sequelae were included to capture the clinical outcomes associated with specific diseases and injuries, which were finally mapped onto 220 different health states. Disability weights were calculated for each health state to measure the degree of associated disability.14
New disability weights were computed for GBD 2010 using data collected through face-to-face interviews (in Peru, Bangladesh, Indonesia and Tanzania), telephone interviews (in the USA) and open access internet surveys. These efforts aimed to quantify the severity of health losses sustained for 220 health states on a range from 0 to 1, where 0 represents “perfect health” and 1, health loss proportionate to death.13,22,23 As some neuropsychiatric disorders comprised of more than one health state, multiple disability weights were estimated. This was done to better accommodate for differences in disability within the course of the disorder. Where this was the case, survey data reporting on the distribution of these health states in the population were then used to proportionally aggregate individual disability weights into an average disability weight.14
Disability weights were also adjusted for comorbidity between diseases using micro-simulation methods.14 Uncertainty was also propagated from the DisMod-MR prevalence output, disability weights and death statistics through to final burden estimates. This method has been described in more detail elsewhere.6,14,15
Finally, disability-adjusted life years (DALYs) were expressed as the sum of YLLs and YLDs.15
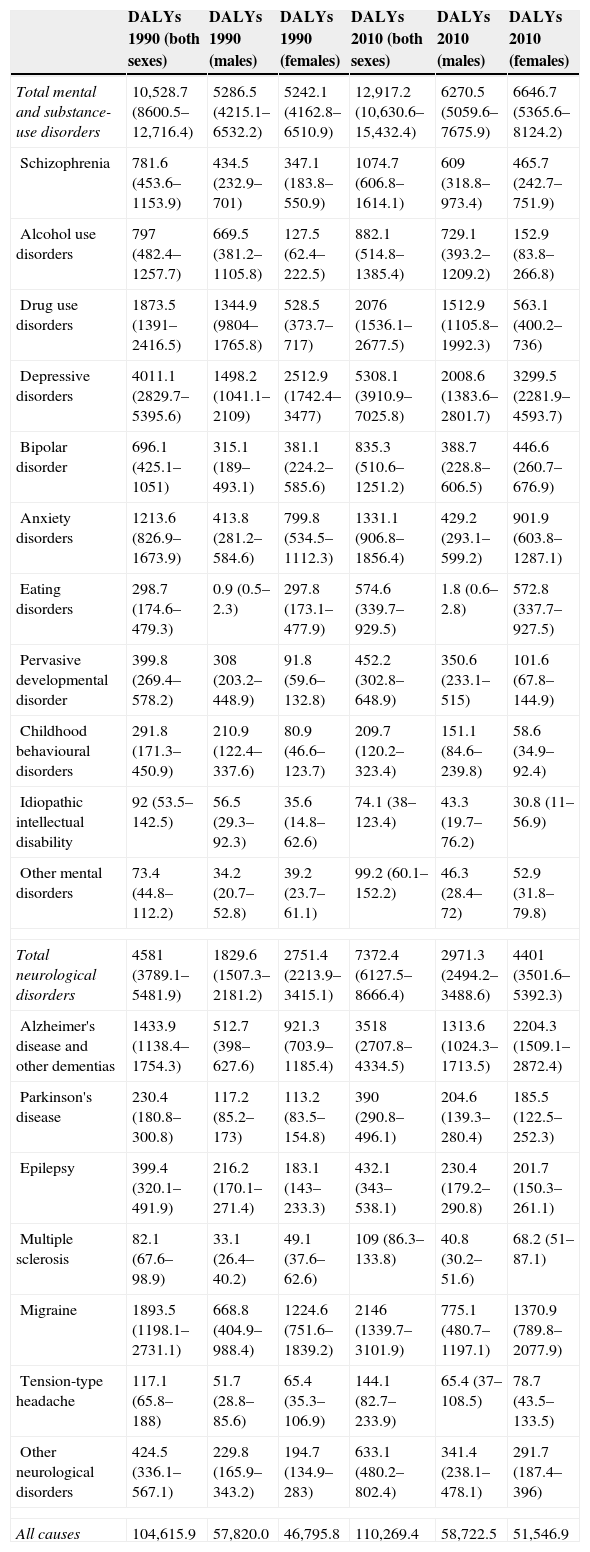
ResultsDisability-adjusted lived years (DALYs)Absolute burdenOverall, the diseases and injuries included in GBD 2010 generated 110,269.4 hundred DALYs in Spain in 2010. Neuropsychiatric disorders were responsible for 18.4% of this burden with 7372.4 hundred (95% UI 6127.5–8666.4) DALYs due to neurological disorders, and 12,917.2 hundred (95% UI 10,630.6–15,432.4) DALYs due to mental and substance-use disorders. Table 1 shows the number of DALYs in 1990 and 2010 in Spain due to each neuropsychiatric disorder. The proportion of DALYs attributable to mental and substance-use disorders were almost double that of neurological disorders (11.7% vs 6.7% respectively).
Comparison of DALYs due to neurological, mental and substance-use disorders in Spain, for 1990 and 2010 (in hundreds with 95% uncertainty).
| DALYs 1990 (both sexes) | DALYs 1990 (males) | DALYs 1990 (females) | DALYs 2010 (both sexes) | DALYs 2010 (males) | DALYs 2010 (females) | |
|---|---|---|---|---|---|---|
| Total mental and substance-use disorders | 10,528.7 (8600.5–12,716.4) | 5286.5 (4215.1–6532.2) | 5242.1 (4162.8–6510.9) | 12,917.2 (10,630.6–15,432.4) | 6270.5 (5059.6–7675.9) | 6646.7 (5365.6–8124.2) |
| Schizophrenia | 781.6 (453.6–1153.9) | 434.5 (232.9–701) | 347.1 (183.8–550.9) | 1074.7 (606.8–1614.1) | 609 (318.8–973.4) | 465.7 (242.7–751.9) |
| Alcohol use disorders | 797 (482.4–1257.7) | 669.5 (381.2–1105.8) | 127.5 (62.4–222.5) | 882.1 (514.8–1385.4) | 729.1 (393.2–1209.2) | 152.9 (83.8–266.8) |
| Drug use disorders | 1873.5 (1391–2416.5) | 1344.9 (9804–1765.8) | 528.5 (373.7–717) | 2076 (1536.1–2677.5) | 1512.9 (1105.8–1992.3) | 563.1 (400.2–736) |
| Depressive disorders | 4011.1 (2829.7–5395.6) | 1498.2 (1041.1–2109) | 2512.9 (1742.4–3477) | 5308.1 (3910.9–7025.8) | 2008.6 (1383.6–2801.7) | 3299.5 (2281.9–4593.7) |
| Bipolar disorder | 696.1 (425.1–1051) | 315.1 (189–493.1) | 381.1 (224.2–585.6) | 835.3 (510.6–1251.2) | 388.7 (228.8–606.5) | 446.6 (260.7–676.9) |
| Anxiety disorders | 1213.6 (826.9–1673.9) | 413.8 (281.2–584.6) | 799.8 (534.5–1112.3) | 1331.1 (906.8–1856.4) | 429.2 (293.1–599.2) | 901.9 (603.8–1287.1) |
| Eating disorders | 298.7 (174.6–479.3) | 0.9 (0.5–2.3) | 297.8 (173.1–477.9) | 574.6 (339.7–929.5) | 1.8 (0.6–2.8) | 572.8 (337.7–927.5) |
| Pervasive developmental disorder | 399.8 (269.4–578.2) | 308 (203.2–448.9) | 91.8 (59.6–132.8) | 452.2 (302.8–648.9) | 350.6 (233.1–515) | 101.6 (67.8–144.9) |
| Childhood behavioural disorders | 291.8 (171.3–450.9) | 210.9 (122.4–337.6) | 80.9 (46.6–123.7) | 209.7 (120.2–323.4) | 151.1 (84.6–239.8) | 58.6 (34.9–92.4) |
| Idiopathic intellectual disability | 92 (53.5–142.5) | 56.5 (29.3–92.3) | 35.6 (14.8–62.6) | 74.1 (38–123.4) | 43.3 (19.7–76.2) | 30.8 (11–56.9) |
| Other mental disorders | 73.4 (44.8–112.2) | 34.2 (20.7–52.8) | 39.2 (23.7–61.1) | 99.2 (60.1–152.2) | 46.3 (28.4–72) | 52.9 (31.8–79.8) |
| Total neurological disorders | 4581 (3789.1–5481.9) | 1829.6 (1507.3–2181.2) | 2751.4 (2213.9–3415.1) | 7372.4 (6127.5–8666.4) | 2971.3 (2494.2–3488.6) | 4401 (3501.6–5392.3) |
| Alzheimer's disease and other dementias | 1433.9 (1138.4–1754.3) | 512.7 (398–627.6) | 921.3 (703.9–1185.4) | 3518 (2707.8–4334.5) | 1313.6 (1024.3–1713.5) | 2204.3 (1509.1–2872.4) |
| Parkinson's disease | 230.4 (180.8–300.8) | 117.2 (85.2–173) | 113.2 (83.5–154.8) | 390 (290.8–496.1) | 204.6 (139.3–280.4) | 185.5 (122.5–252.3) |
| Epilepsy | 399.4 (320.1–491.9) | 216.2 (170.1–271.4) | 183.1 (143–233.3) | 432.1 (343–538.1) | 230.4 (179.2–290.8) | 201.7 (150.3–261.1) |
| Multiple sclerosis | 82.1 (67.6–98.9) | 33.1 (26.4–40.2) | 49.1 (37.6–62.6) | 109 (86.3–133.8) | 40.8 (30.2–51.6) | 68.2 (51–87.1) |
| Migraine | 1893.5 (1198.1–2731.1) | 668.8 (404.9–988.4) | 1224.6 (751.6–1839.2) | 2146 (1339.7–3101.9) | 775.1 (480.7–1197.1) | 1370.9 (789.8–2077.9) |
| Tension-type headache | 117.1 (65.8–188) | 51.7 (28.8–85.6) | 65.4 (35.3–106.9) | 144.1 (82.7–233.9) | 65.4 (37–108.5) | 78.7 (43.5–133.5) |
| Other neurological disorders | 424.5 (336.1–567.1) | 229.8 (165.9–343.2) | 194.7 (134.9–283) | 633.1 (480.2–802.4) | 341.4 (238.1–478.1) | 291.7 (187.4–396) |
| All causes | 104,615.9 | 57,820.0 | 46,795.8 | 110,269.4 | 58,722.5 | 51,546.9 |
Between 1990 and 2010 absolute DALY values increased from 4.3% to 6.7% for neurological disorders and from 10% to 11.7% of total DALYs for mental and substance-use disorders. Within neuropsychiatric disorders, the top five leading causes of DALYs in 2010 were: depressive disorders, Alzheimer's disease, migraine, substance-use disorders, and anxiety disorders, accounting for 70.9% of all neuropsychiatric disorders. These DALY findings for 2010 are similar to those obtained in 1990 except for Alzheimer's disease (Table 1).
Sex and age trendsRegarding gender differences, DALYs for Alzheimer's disease, migraine, depressive disorders, anxiety disorders and eating disorders were highest in females. In comparison, DALYs for substance-use disorders, pervasive developmental disorders and childhood behavioural disorders were highest in males (Table 1).
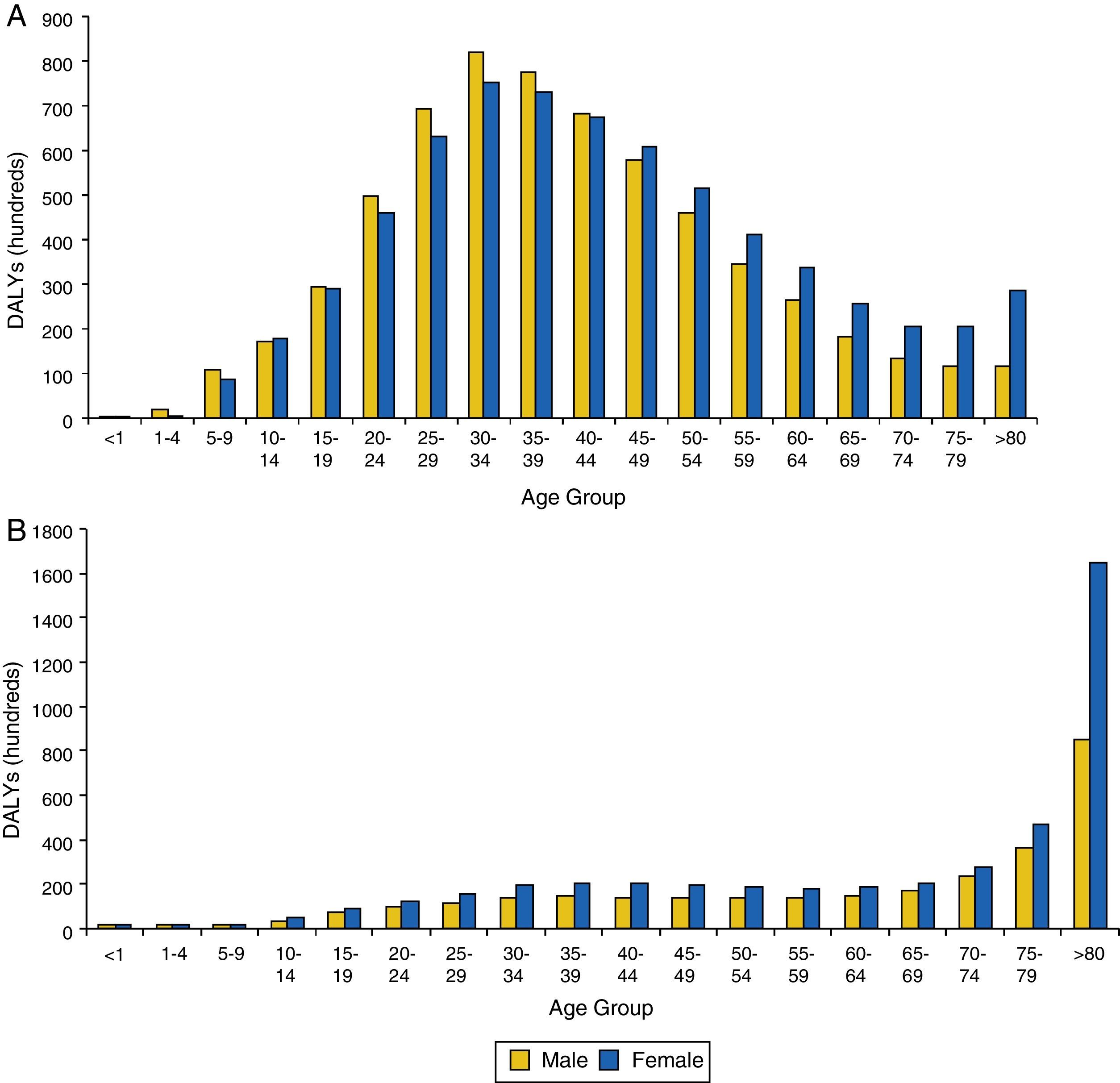
Overall, males accounted for 45.5% of total DALYs for neuropsychiatric disorders while females accounted for 54.5%. Fig. 1a shows the distribution of DALYs due to mental and substance-use disorders (as a group) by age and sex. DALYs peaked between 25 and 44 years, accounting for 44.7% of DALYs. Up to 44 years, males explained a higher proportion of DALYs in mental and substance-use disorders whereas from 44 years old onwards, this effect was reversed with females explaining a higher proportion of DALYs. Fig. 1b shows the distribution of DALYs due to neurological disorders (as a group) by age and sex. DALYs increased substantially through life due to the contribution of disorders such as dementia that are more prevalent in the elderly. There was also a higher proportion of DALYs among females compared to males, especially in the elderly.
 DALY in Spain, in 2010, for all related mental and substance use disorders, sex and age. (B) DALY in Spain, in 2010, for all neurological disorders, by sex and age.")
Fig. 2a illustrates the distribution of DALYs attributable to each mental and substance-use disorder by age. Depressive disorders explained the highest proportion of DALYs throughout the entire life span representing 26% of all DALYs. The burden associated with substance-use disorders increased during adolescence, with a peak between 20 and 34 years. A similar course to that in drug-use disorders has been observed in alcohol-use disorders, accounting for 20.5% of burden among the youngest individuals (aged 15–29) and 58% for adults (aged 30–55), with a decrease over the years.
 DALY in Spain, in 2010, for each related mental and substance use disorder by age. (B) DALY in Spain, in 2010, for each neurological disorder by age.")
Less common mental disorders, such as bipolar disorder or schizophrenia, had a later onset although they tended to be more chronic. These accounted for the greatest proportion of burden from 25 to 55 years. DALYs due to other disorders such as eating disorders, anxiety disorders and childhood behavioural disorders were highest in childhood and adolescence, and in the case of anxiety disorders, the burden remained steady at all ages.
Fig. 2b illustrates the distribution of DALYs due to neurological disorder by age, which shows a different pattern compared with that of mental and substance-use disorders. The distribution of DALYs was skewed to the right (i.e., a higher number of DALYs in older age groups), with Alzheimer's disease making the largest contribution to the burden (47.7%) of all neurological disorders. Migraine was the second leading cause of DALYs for neurological disorders (29%) and was highest amongst those aged 30–50 years. The burden of epilepsy began in childhood, increased in adulthood and remained steady in the elderly. DALYs due to Parkinson's disease was also highest in the elderly.
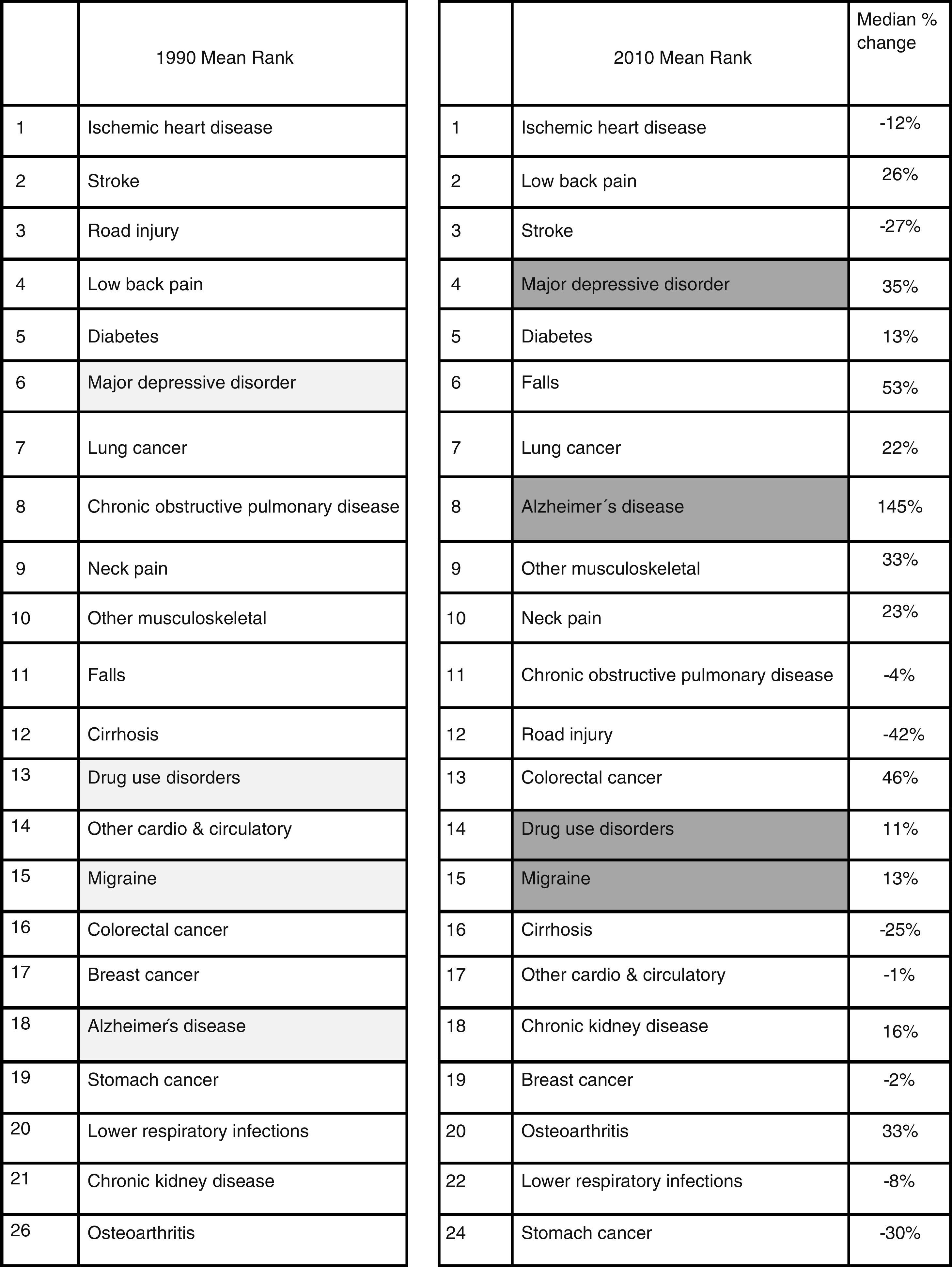
Burden rankingFig. 3 summarises the top 26 leading causes of DALYs in Spain, in 1990 and 2010. This was derived using burden rankings produced by GBD 2010.15 Ischaemic heart disease maintained its position as the primary cause of DALYs in both 1990 and 2010 although, a number of neuropsychiatric disorders moved up in terms of ranking between 1990 and 2010. Four of the top 20 causes of DALYs in 2010 were neuropsychiatric disorders (i.e., depressive disorders, Alzheimer's disease, drug-use disorders, and migraine). In 1990, depressive disorders were ranked as the sixth leading cause of DALYs but reached fourth position in 2010, representing an increase of 35%. The most remarkable change was observed in Alzheimer's disease, with an increase of 145%, moving from eighteenth position in 1990 to eighth in 2010. Migraine and substance-use disorders were in the same position in 1990 and 2010, however, both saw an increase in terms of absolute of DALYs between the two time points (11% for substance-use disorders and 13% for migraine).
Years lived with disability (YLDs)
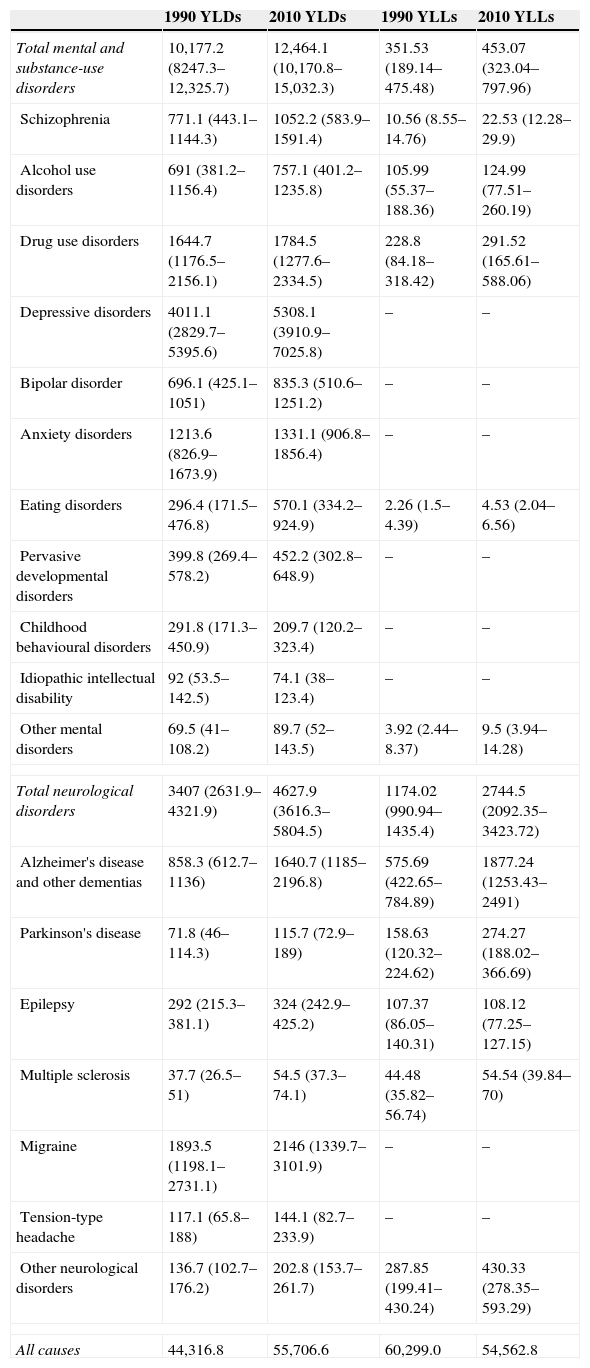
Table 2 shows YLDs and YLLs due to neuropsychiatric disorders in Spain, in 1990 and 2010. Overall, the diseases and injuries included in GBD 2010 generated 55,706.6 hundred YLDs. Mental and substance-use disorders made an important contribution, accounting for 22.4% of all YLDs in 2010. Depression was found to be the most disabling disease (5308.1 hundred, 95% UI 3910.9–7025.8), accounting for 42.6% of mental and substance-use disorders. The burden attributable to depression in 1990 was lower (39.4%). Drug-use disorders and anxiety disorders accounted for 14.3% and 10.7% of mental and substance-use disorder YLDs respectively. The leading causes of YLDs among neurological disorders were migraine and Alzheimer's disease, representing more than 80% of YLDs for neurological disorders. Compared with 1990, Alzheimer's disease increased its contribution to YLDs from 25.2% to 35.5%.
Comparison of YLLs and YLDs for neurological, mental and substance-use disorders in Spain for 1990 and 2010 (in hundreds, with 95% uncertainty).
| 1990 YLDs | 2010 YLDs | 1990 YLLs | 2010 YLLs | |
|---|---|---|---|---|
| Total mental and substance-use disorders | 10,177.2 (8247.3–12,325.7) | 12,464.1 (10,170.8–15,032.3) | 351.53 (189.14–475.48) | 453.07 (323.04–797.96) |
| Schizophrenia | 771.1 (443.1–1144.3) | 1052.2 (583.9–1591.4) | 10.56 (8.55–14.76) | 22.53 (12.28–29.9) |
| Alcohol use disorders | 691 (381.2–1156.4) | 757.1 (401.2–1235.8) | 105.99 (55.37–188.36) | 124.99 (77.51–260.19) |
| Drug use disorders | 1644.7 (1176.5–2156.1) | 1784.5 (1277.6–2334.5) | 228.8 (84.18–318.42) | 291.52 (165.61–588.06) |
| Depressive disorders | 4011.1 (2829.7–5395.6) | 5308.1 (3910.9–7025.8) | – | – |
| Bipolar disorder | 696.1 (425.1–1051) | 835.3 (510.6–1251.2) | – | – |
| Anxiety disorders | 1213.6 (826.9–1673.9) | 1331.1 (906.8–1856.4) | – | – |
| Eating disorders | 296.4 (171.5–476.8) | 570.1 (334.2–924.9) | 2.26 (1.5–4.39) | 4.53 (2.04–6.56) |
| Pervasive developmental disorders | 399.8 (269.4–578.2) | 452.2 (302.8–648.9) | – | – |
| Childhood behavioural disorders | 291.8 (171.3–450.9) | 209.7 (120.2–323.4) | – | – |
| Idiopathic intellectual disability | 92 (53.5–142.5) | 74.1 (38–123.4) | – | – |
| Other mental disorders | 69.5 (41–108.2) | 89.7 (52–143.5) | 3.92 (2.44–8.37) | 9.5 (3.94–14.28) |
| Total neurological disorders | 3407 (2631.9–4321.9) | 4627.9 (3616.3–5804.5) | 1174.02 (990.94–1435.4) | 2744.5 (2092.35–3423.72) |
| Alzheimer's disease and other dementias | 858.3 (612.7–1136) | 1640.7 (1185–2196.8) | 575.69 (422.65–784.89) | 1877.24 (1253.43–2491) |
| Parkinson's disease | 71.8 (46–114.3) | 115.7 (72.9–189) | 158.63 (120.32–224.62) | 274.27 (188.02–366.69) |
| Epilepsy | 292 (215.3–381.1) | 324 (242.9–425.2) | 107.37 (86.05–140.31) | 108.12 (77.25–127.15) |
| Multiple sclerosis | 37.7 (26.5–51) | 54.5 (37.3–74.1) | 44.48 (35.82–56.74) | 54.54 (39.84–70) |
| Migraine | 1893.5 (1198.1–2731.1) | 2146 (1339.7–3101.9) | – | – |
| Tension-type headache | 117.1 (65.8–188) | 144.1 (82.7–233.9) | – | – |
| Other neurological disorders | 136.7 (102.7–176.2) | 202.8 (153.7–261.7) | 287.85 (199.41–430.24) | 430.33 (278.35–593.29) |
| All causes | 44,316.8 | 55,706.6 | 60,299.0 | 54,562.8 |
Overall, the diseases and injuries included in GBD 2010 generated 54,562.8 hundred YLLs in 2010. Neurological disorders accounted for 2744.5 hundred (95% UI 2092.35–3423.72) YLLs, equivalent to 5.03% of total YLLs. Within this group, Alzheimer's disease was the main cause of mortality, accounting for 58.7% of YLLs for neurological disorders. Mental and substance-use disorders accounted for 453.07 hundred (95% UI 323.04–797.96) YLLs, equivalent to 0.8% of total YLLs. Within this group, substance-use disorders were the main cause of mortality accounting for 64.34% of YLLs for mental and substance-use disorders (Table 2).
DiscussionIn spite of the low contribution of neuropsychiatric disorders to global YLLs, this group of disorders was the most disabling, accounting for 30.7% of total YLDs in Spain in 2010. Overall, most neuropsychiatric disorders increased in burden between 1990 and 2010. This increase was driven by changes population growth and ageing and in some instances (e.g. for substance-use disorders) increases in the prevalence rate. Depressive disorders were the most disabling of the neuropsychiatric disorders due to the high prevalence and disability weight associated with major depressive disorder.6 Nevertheless, it is important to note that, as illustrated by Whiteford and colleagues, other neuropsychiatric disorders such as schizophrenia and Parkinson's disease were ranked with a high disability weight in GBD 2010 but accounted for a lower percentage of YLDs and DALYs because their prevalences were lower.6,24
The burden of neuropsychiatric disorders varied across the lifespan. Burden was high in young adults and the elderly. The high proportion of burden due to neuropsychiatric disorders in young adults could be explained in some cases by an early onset of disorders associated with a high prevalence such as substance-use disorders, anxiety disorders and depressive disorders. The results also showed a high proportion of burden due to neurological disorders in the elderly. This was largely explained by the increase in the prevalence of highly disabling neurological disorders such as Alzheimer's disease or Parkinson's disease. As the population ages due to increases in life expectancy, it is expected that burden of diseases occurring in the elderly will also increase making neuropsychiatric disorders an important target for both the current and future health of the Spanish population.25
Significant differences were found when comparing Spanish data with global results. In 2010, neuropsychiatric disorders accounted for 10.4% of all DALYs worldwide, and 15.4% in developed countries,15 whereas in the Spanish population the figure was 18.4%. Although trends are similar in Spain and globally over the years, neuropsychiatric disorders make a larger contribution to disease burden in Spain.
Concerning the burden of disease in other European countries, we observed that, overall, the burden attributable to neuropsychiatric disorders was similar as well. All neuropsychiatric diseases included in the top 20 causes of DALYs increased their percentage contribution from 1990. Indeed, depression was the most disabling disorder among neuropsychiatric disorders in countries such as France, the United Kingdom, Germany and Italy, ranking between third and seventh position in terms of absolute DALYs. Other disorders, which were also among the 20 leading causes of DALYs in France, the United Kingdom, Germany and Italy, were Alzheimer's disease, drug-use disorder, migraine, anxiety disorders or alcohol-use disorder, with varying percentages.26–29
Findings from GBD 2010 are in line with findings from previous epidemiological studies that have demonstrated the high impact of neuropsychiatric disorders in the population.8,10 For instance, the ESEMeD study reported a high prevalence of mental disorders in Spain, particularly depression.7 Separate analyses of burden in Spain have also highlighted the impact of neuropsychiatric disorders, although there were differences in the methodology used to estimate burden. These studies also emphasised neuropsychiatric disorders as a leading contributor of total DALYs, especially for women and those ages between 15 and 30 years of age.30,31 Similarly, dementia was also highlighted as a major contributor of disease burden in the elderly.32 Research focused on the Valencia and Andalusia regions of Spain obtained comparable results.33,34
In spite of these findings, the direct and indirect costs of neuropsychiatric disorders are inadequately covered in most countries.35 The budget set for neuropsychiatric disorders in Spain represents less than 10% of public health expenditure36 and not in line with our results which highlight neuropsychiatric disorders as a leading contributor to disability. Our findings underline the importance of prioritising neuropsychiatric disorders in the national health policies and allocating resources towards their prevention and management.
LimitationsDespite the progress made compared with previous GBD studies, we need to consider the limitations associated with GBD 2010 while interpreting findings. First, as the number of disorders included was limited, the burden of neuropsychiatric disorders may have been underestimated. Disorders were included if there was sufficient data to derive defensible estimates of burden. As such, disorders such as personality disorders, somatoform disorders and substance-abuse were not included.
Second, neuropsychiatric disorders were defined according to DSM and ICD guidelines which may not capture all presentations of the disorders. However, this was necessary to facilitate the comparison of epidemiological data and burden estimates between settings. Future work on burden of disease will have to explore how recent changes to these guidelines (for instance, the changes proposed in the latest iteration of DSM) will impact on the estimated burden of neuropsychiatric disorders in Spain. Third, neuropsychiatric disorders contributed to a much smaller proportion of YLLs compared to YLDs. The ICD-10 guidelines used in GBD 2010s cause of death allocations can only attribute deaths to the direct (rather than the underlying) cause. As such, deaths due to neuropsychiatric were allocated to other causes in GBD 2010 (e.g. suicide related deaths due to having a mental disorder allocated to injuries).9,22,37
Fourth, was the non-inclusion of social consequences in estimating disability weights. The impact of neuropsychiatric disorders on functioning and society at large, although well publicised was not considered.38,39 Finally, although 95% uncertainty intervals were presented for all high level findings in GBD 2010, given the lack of data available on the epidemiology of neuropsychiatric disorders, uncertainty intervals were often large and overlapping. This needs to be considered while interpreting findings. With ongoing epidemiological research and updates of GBD estimates, we aim to be able to reduce the unexplained sources of uncertainty around estimates of burden for neuropsychiatric disorders.
ConclusionsThis study contributes to understanding of the burden of neuropsychiatric disorders in Spain and demonstrates that they should be considered an integral component of the public health system. Findings highlight the urgent need for health policy focusing on the development of effective and affordable approaches to reducing the existing burden of neuropsychiatric disorders in Spain and prevention programmes to reduce incident-cases of these disorders in the population. That said, more epidemiological research is needed for a better understanding of burden. Future studies should also consider the contribution of social and economic determinants to the burden of neuropsychiatric disorders.
FundingThis study has been supported by Bill & Melinda Gates Foundation. This study was done as part of GBD 2010.
Conflict of interestThe authors declare that they have no conflict of interests.
We would like to acknowledge all members who have contributed to the Global Burden of Disease Study 2010 (GBD 2010). Specifically, we would like to thank the GBD 2010 Expert Groups on Neurological, Mental and Substance Use Disorders and Illicit Drug. We would also like to express our sincere thanks to all Spanish participants in this study.
Please cite this article as: Lara E, Garin N, Ferrari AJ, Tyrovolas S, Olaya B, Sànchez-Riera L, et al. La carga de la enfermedad en España 2010: trastornos neurológicos, mentales y re: trastornos neurológicos, mentales y relacionados con el consumo de sustancias. Rev Psiquiatr Salud Ment (Barc.). 2015;8:207–217.