




Anxiety symptoms in childhood and adolescence are an important risk factor for developing anxiety disorders in subsequent developmental stages. This study examines the frequency and characteristics of the symptoms of the principal anxiety disorders in children and adolescents using a self-report questionnaire based on the diagnostic categories of the American Psychiatric Association (APA) manual.
Materials and methodsA cross-sectional, non-interventional study was conducted on 2522 children and adolescents aged 8 to 17 years (49% males), enrolled from different schools in the Province of Alicante who completed the Spence Children's Anxiety Scale.
ResultsThe mean score obtained on the scale (range: 0–114) was 25.15 (standard deviation (SD)=13.54). More than one in four (26.41%) of the children and adolescents showed high scores in any anxiety disorder. The anxiety symptoms due to separation were the most frequent in the sample (5.5%), followed by physical fears (5.1%). Girls scored significantly higher in all disorders (P<.001), except in obsessive-compulsive disorder. Differences were found as regards to age in all disorders, except physical fears, but the effect sizes were only in anxiety due to separation, which decreased with age, and generalised anxiety, which was higher in adolescents than in children.
ConclusionsFrom the mental health perspective, it is important to be able to detect anxiety symptoms in children from 8 years onwards, in order to intervene early and prevent the development of anxiety disorders in later life.
Los síntomas de ansiedad en la infancia y adolescencia constituyen un importante factor de riesgo para el desarrollo de los trastornos de ansiedad en etapas evolutivas posteriores. Este estudio examina la frecuencia y características de los síntomas de los principales trastornos de ansiedad en niños y adolescentes empleando una medida de autoinforme basada en las categorías diagnósticas del manual de la APA.
Material y métodosSe trata de un estudio transversal no intervencionista. Participaron 2.522 niños y adolescentes de 8 a 17 años (49% varones), reclutados de diversos colegios de la provincia de Alicante, que completaron la Escala de Ansiedad Infantil de Spence.
ResultadosLa puntuación media obtenida en la escala (rango: 0-114) fue 25,15 (DT=13,54). El 26,41% de los niños y adolescentes mostraron puntuaciones elevadas en cualquier trastorno de ansiedad. Los síntomas de ansiedad por separación son los más frecuentes en la muestra (5,5%), seguidos por los miedos físicos (5,1%). Las niñas puntúan significativamente más alto en todos los trastornos (p<,001), excepto en el trastorno obsesivo-compulsivo. Se hallaron diferencias en función de la edad en todos los trastornos, excepto en los miedos físicos, pero los tamaños del efecto fueron medios únicamente en la ansiedad por separación, que desciende con la edad, y en la ansiedad generalizada, mayor en los adolescentes que en los niños.
ConclusionesSe destaca la importancia de que, desde el ámbito de salud mental, se lleve a cabo una detección temprana de los síntomas de ansiedad en los niños a partir de 8 años para facilitar la intervención y evitar el desarrollo posterior de los trastornos de ansiedad.
Epidemiological studies indicate that anxiety disorders are the most frequently diagnosed psychological problem in Spanish children and adolescents and those that are most in demand in the mental health units.1 Their prevalence can vary considerably depending on age, assessment tools used in the studies and source of information, among other variables.2 In general, it is estimated that 15–20% of children and adolescents have an anxiety disorder,2 although some studies have found a lower prevalence.3–5 Various studies have explored the symptomatology and characteristics in the Spanish population, due to its elevated prevalence. However, most of these studies focus on a specific anxiety disorder. Consequently, there is a great deal of data on, for example, separation anxiety,6 social anxiety7 or specific fears,8,9 while others such as generalised anxiety, obsessive-compulsive disorder and panic disorder have been the object of fewer studies.
There are numerous tools with good psychometric properties for assessing anxiety in children and adolescents. Among them, the Spence Children's Anxiety Scale (SCAS) stands out because of its advantages compared with other assessment measurements.10 The SCAS was originally created to apply with Australian community populations, but it has been translated and validated for its application to children and adolescents in 17 countries; it is considered one of the self-report measurements most utilised internationally. In contrast to other scales, the SCAS is not an adaptation of a test designed for adults, so it takes into consideration the differential symptoms in anxiety disorders in children and adults. In creating the SCAS, its author based it on the symptoms of the anxiety disorders most common in childhood and adolescence according to the categories diagnosed in the DSM-IV.11 The test therefore permits assessing, through 6 domains, the symptoms of the anxiety disorders most frequently found in children and adolescents. The scale has been used in numerous international studies for research and clinical purposes. Although it is not a diagnostic test, the SCAS has been used clinically as a screening tool to identify children and adolescents with high levels of anxiety symptoms who may need intervention. At the research level, the scale has been applied to study cultural differences of anxiety in childhood.12,13
In spite of the prevalence of anxiety disorders in Spanish children and adolescents and the demand for services in our country, there are no recent studies that examine the characteristics of the most frequent disorders using measurement tools based on the APA manual diagnostic categories. Our study updates the literature on the prevalence and characteristics of some anxiety disorders studied over a decade ago and provides information on disorders for which fewer data are available with the Spanish population. The objectives of this study were therefore to examine, in a community sample of Spanish children and adolescents from 8 to 17 years old, the following: (1) the frequency of the symptoms of the main anxiety disorders using the SCAS, an internationally recognised self-report tool based on the APA manual diagnostic categories, and (2) the differences in the anxiety disorder symptoms depending on age and sex.
Materials and methodsParticipantsThis was a non-interventionist transversal study in which the participants were 2522 children and adolescents from 8 to 17 years old, 49% being males. The age distribution was as follows: 5.9% (n=149) 8 years old, 9.1% (n=229) 9 years, 9.4% (n=237) 10 years, 13% (329) 11 years, 17.6% (n=444) 12 years, 10.5% (n=265) 13 years, 10% (n=251) 14 years, 11.3% (n=284) 15 years, 8.2% (208) 16 years, and 5% (n=126) 17 years old. As to nationality, 85.3% were Spanish and the remaining participants had been born in other countries. The socio-economic level, based on the parents’ labour situation and the location of the school the children attended, was middle class. With respect to family, 74% had married parents; 18%, separated or divorced parents; 5% lived with their parents, who were not married; 1% had a single parent situation with the mother; and 2% were orphans, lacking 1 parent or both. Most of the children and adolescents had only 1 brother or sister (59%), 19% had 2 siblings, 13% were the only children, 6% had 3 siblings, and the remaining participants had more than 4 siblings.
ProcedureWe recruited the participants in 15 schools (state schools and non-state schools that received state funding) in the province of Alicante, randomly chosen from rural and city areas, from the coastal and inner regions. The school directors gave their authorisation and the children's parents gave their informed consent, with 95% of the parents consenting that their children could participate in the study. The participants filled out the questionnaires anonymously in the classrooms. The questionnaires were handed out and the instructions were read out loud. The participants were asked to answer honestly and openly and to raise a hand if they had any doubts. No participant left more than 20% of the items blank, so no questionnaire was excluded from the data analysis. The Ethics Committee of the institution to which the authors form a part had previously approved the study.
Assessment toolsThe participants filled in a brief socio-demographic questionnaire, providing information as to age, gender, mother and father's employment, family situation, number of siblings and country of birth.
The anxiety disorder symptoms were assessed using the Spanish version of the Spence Children's Anxiety Scale.14 The SCAS is a 44-item scale designed to measure anxiety disorder symptoms in community samples of children and adolescents. The maximum score is 114. The scale consists of 5 subscales that correspond to the DSM-IV anxiety disorders most frequently in the child-adolescent population: generalised anxiety disorder (range: 0–18), obsessive-compulsive disorder (range: 0–18), panic and agoraphobia (range: 0–27), social phobia (range: 0–18), separation anxiety disorder (range: 0–18) and physical fears (range: 0–15). For each item, the children had to indicate how often each symptom occurred, using a Likert-style 4-point scale: never, sometimes, often or always. The psychometric properties of the scale are good with Spaniards, with high internal consistency (Cronbach's alpha=0.89) and appropriate convergent validity with another anxiety disorder measurement (r=0.41). The factorial structure of the Spanish version maintains the 6 factors used in the original test version.14
Statistical analysisWe established 3 age groups based on the level of development and in agreement with other authors’ classification15: preadolescence (from 8 to 11 years old), middle adolescence (12–13) and adolescence (14–17 years old). The mean scores, standard deviations (SD) and percentage of sample subjects showing symptoms of each disorder were found; the criterion of the mean plus 2 SD was used as recommended by the author of the test. To ascertain the differences by age and gender, we performed multivariate variance analysis (MANOVA), including sex and gender as fixed factors and the SCAS subscales as dependent variables. We found the Cohen's size effect for the comparisons that were significant, considering 0.20 as a small size, 0.50 as medium and 0.80 as big.16 All the statistical analyses were performed using the program PASW.
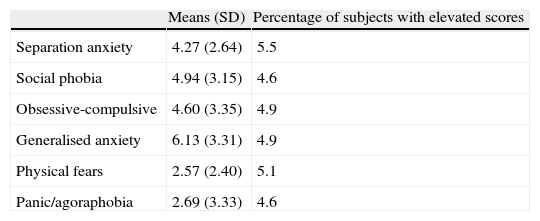
ResultsThe mean participant score obtained on the scale was 25.15 (SD=13.54). Table 1 indicates the mean scores on the test subscales, as well as the percentage of children and adolescents that showed high symptoms in each disorder. The cut-off point for considering anxiety disorder symptoms elevated was 12.8 for the separation anxiety disorder subscale, 11.2 for social phobia, 11.3 for obsessive-compulsive disorder, 7.4 for physical fears, 9.4 for panic and agoraphobia, and 52.2 for the total score. Out of the total for the sample, 26.41% (n=666) of the participants had high scores on some type of anxiety disorder. We did not find any high percentages of comorbidity between the symptoms of the disorders. The comorbidity most frequently found was between separation anxiety disorder and physical fears (1.6%), between separation anxiety disorder and panic disorder (1.5%), and between panic disorder and obsessive-compulsive disorder (1.4%).
Means (standard deviations) and sample percentage with elevated anxiety disorder symptoms.
| Means (SD) | Percentage of subjects with elevated scores | |
| Separation anxiety | 4.27 (2.64) | 5.5 |
| Social phobia | 4.94 (3.15) | 4.6 |
| Obsessive-compulsive | 4.60 (3.35) | 4.9 |
| Generalised anxiety | 6.13 (3.31) | 4.9 |
| Physical fears | 2.57 (2.40) | 5.1 |
| Panic/agoraphobia | 2.69 (3.33) | 4.6 |
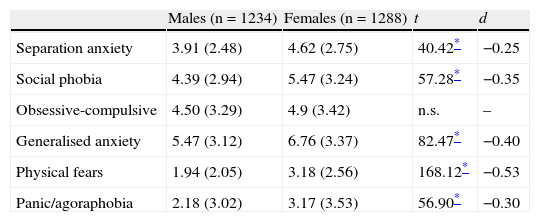
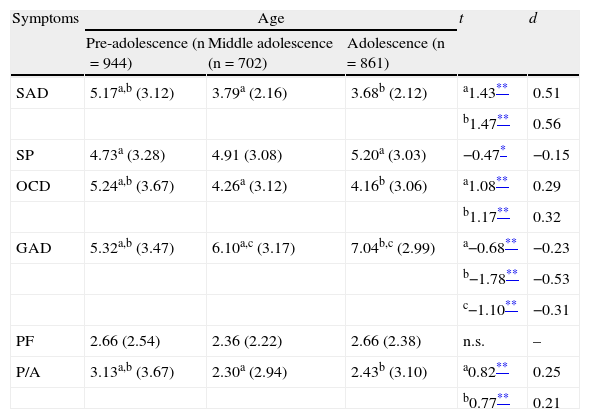
Significant differences were found in all the dependent variables based on the gender of the participants (F=37.435; P<.001), on age (F=4416; P<.001) and on the interaction between both factors (F=3.657; P<.001). Looking at gender, the differences were significant in all the subscales, with higher scores by the girls than the boys (P<.001); the only exception was in the symptoms for the obsessive-compulsive disorder, in which there were no significant differences. Table 2 shows the means and SDs for males and females, as well as the result of the comparisons in each subscale and in the total score, plus the size of the effect. Based on age, the differences were significant for all the variables except for physical fears. In the subscales for separation anxiety disorder, obsessive-compulsive disorder and panic/agoraphobia, the pre-adolescents presented higher score than the participants in middle adolescence (P<.001) or adolescence (P<.001). In social phobia, the adolescents presented higher scores than those in middle adolescence (P<.01). In generalised anxiety disorder, the differences were significant between all the developmental stages, the older the child, the higher the score (P<.001). The means and SDs for each age group, as well as the post hoc comparisons and the size of the effect are presented in Table 3. The interaction between the factors of age and gender was significant only in the subscale for separation anxiety disorder (F=4.672; P<.01).
Differences by gender: means (standard deviations), statistical significance and size of the effect.
| Males (n=1234) | Females (n=1288) | t | d | |
| Separation anxiety | 3.91 (2.48) | 4.62 (2.75) | 40.42* | −0.25 |
| Social phobia | 4.39 (2.94) | 5.47 (3.24) | 57.28* | −0.35 |
| Obsessive-compulsive | 4.50 (3.29) | 4.9 (3.42) | n.s. | – |
| Generalised anxiety | 5.47 (3.12) | 6.76 (3.37) | 82.47* | −0.40 |
| Physical fears | 1.94 (2.05) | 3.18 (2.56) | 168.12* | −0.53 |
| Panic/agoraphobia | 2.18 (3.02) | 3.17 (3.53) | 56.90* | −0.30 |
d=Cohen's effect size; n.s.=non-significant differences.
Differences by age: means (standard deviations), statistical significance and size of the effect.
| Symptoms | Age | t | d | ||
| Pre-adolescence (n=944) | Middle adolescence (n=702) | Adolescence (n=861) | |||
| SAD | 5.17a,b (3.12) | 3.79a (2.16) | 3.68b (2.12) | a1.43** | 0.51 |
| b1.47** | 0.56 | ||||
| SP | 4.73a (3.28) | 4.91 (3.08) | 5.20a (3.03) | −0.47* | −0.15 |
| OCD | 5.24a,b (3.67) | 4.26a (3.12) | 4.16b (3.06) | a1.08** | 0.29 |
| b1.17** | 0.32 | ||||
| GAD | 5.32a,b (3.47) | 6.10a,c (3.17) | 7.04b,c (2.99) | a−0.68** | −0.23 |
| b−1.78** | −0.53 | ||||
| c−1.10** | −0.31 | ||||
| PF | 2.66 (2.54) | 2.36 (2.22) | 2.66 (2.38) | n.s. | – |
| P/A | 3.13a,b (3.67) | 2.30a (2.94) | 2.43b (3.10) | a0.82** | 0.25 |
| b0.77** | 0.21 | ||||
GAD: generalised anxiety disorder; OCD: obsessive-compulsive disorder; P/A: panic/agoraphobia; PF: physical fears; SAD: separation anxiety disorder; SP: social phobia.
d=Cohen's effect size; n.s.=non-significant differences.
The means that share the same superscript are statistically significant.
The objective of this study was to examine the characteristics of the symptoms of the main types of anxiety disorder in a wide sample of children and adolescents with ages that ranged from 8 to 17 years old. Our study results show that the symptoms of separation anxiety disorder are the most frequent, followed by the symptoms of physical fears. These findings coincide with the results of previous studies that indicated that separation anxiety disorder, together with specific phobias, is the most frequent anxiety disorder in children and adolescents.2 Our study also provides information on the frequency of the symptoms of other types of anxiety disorder less studied in Spanish children and adolescents, such as generalised anxiety disorder or panic disorder (the latter being the one of least prevalence, along with social phobia). The percentage of children and adolescents with high scores in one of the types of anxiety disorder is greater in our study as compared to previous studies.2–5 The higher prevalence found could be due to the fact that our study assessed symptoms of anxiety disorders and not diagnosed disorders.
Looking at the differences by gender, the girls showed more anxiety than did the boys in all the disorders, except for in obsessive-compulsive disorder. Numerous international studies17,18 state that anxiety disorders are more frequent in females, which coincides with our findings. The absence of significant differences in the symptoms of obsessive-compulsive disorder in function of gender coincides with the results of previous studies in which boys and girls do not differ in the percentage that manifest the symptoms of this disorder.19
The results indicate that, the older the child, the fewer the symptoms of separation, obsessive-compulsive and panic disorders, but the greater the symptoms of social phobia and anxiety disorder. The sizes of the effect also suggest that it is in the symptoms for separation and generalised anxiety disorders where the differences by age are greatest. The fact that separation anxiety disorder symptoms decrease with age is a common finding in previous studies.6 The explanation is that this disorder is considered a developmental fear that tends to disappear as the child matures, but it can constitute an anxiety disorder typical in childhood, with onset before the age of 18 years. Despite previous studies20,21 indicating that the risk of having an obsessive-compulsive disorder and a panic disorder increase with age, in our study the prevalence was lower as children's ages increased, although the size of the effect indicated only very small differences. The discrepancy between our results and previous findings could be due to the fact that we used a self-report instrument that evaluates elevated anxiety disorder symptoms in a community sample, not clinical disorders. With respect to obsessive–compulsive disorder symptoms, prior studies indicated that rituals and manias are common in small children22; these could therefore have considered such rituals as excessive, thereby obtaining higher scores than the adolescents. The higher scores in social phobia and generalised anxiety disorder reached at older ages coincides with the published scientific literature that indicates that both the social fears and the excessive worries characteristic of generalised anxiety disorder usually appear from pre-adolescence on.23,24 Lastly, the physical fears in our study participants are constant with age, in agreement with the data in the literature indicating that the fears and phobias that occur in adults might derive from intense fears that appeared in childhood or adolescence.25
This study presents certain limitations and strengths. The main limitation lies in that the information was collected through a report from the children and adolescents and anxiety disorder measurements were not obtained through the parents. It is true that it would have been helpful to have included more than one source of information in the assessment. In spite of this, given the subjective component of discomfort inherent in anxiety disorders, we considered assessment by the subjects themselves an appropriate option. As a study strength, we can emphasise that it updates data on the frequency and characteristics of the symptoms of anxiety disorders in a community sample of children and adolescents, based on the APA manual classification; this in turns makes it possible to know, in greater detail, specific anxiety disorders little studied in Spanish children and adolescents. Greater knowledge of such symptoms makes it easier for mental health professionals to detect and treat them earlier, preventing such subclinical manifestations from constituting clinical anxiety disorders in later developmental stages.
FundingThis research was funded by a Bancaja-UMH project and a Spanish Scientific Research, Development and Technological Innovation Plan project (EDU2008-05060).
Ethical responsibilitiesProtection of people and animals. The authors declare that no experiments were performed on humans or animals for this study.
Data confidentiality. The authors declare that no patient data appear in this article.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Conflict of interestThe authors have no conflict of interest to declare.
Please cite this article as: Orgilés M, et al. Síntomas de trastornos de ansiedad en niños y adolescentes: diferencias en función de la edad y el sexo en una muestra comunitaria. Rev Psiquiatr Salud Ment (Barc.). 2012;5:115–20.