

An angiomyofibroblastoma-like tumor is a rare mesenchymal tumor that arises in the scrotum, inguinal region or perineum in men. It is usually described as superficial, originating in subcutaneous tissues. In the present case we found an angiomyofibroblastoma-like tumor with a different clinical presentation. We describe a benign tumor that mimicked a testicular tumor clinically and in imaging exams. This tumor was herniated to the scrotum through an indirect inguinal hernia that had arisen from the omentum and the mesenteric/splanchnic circulation; these were the only structures it was linked to. Surgical excision is the recommended treatment and cure is obtained in most cases.
Um angiomiofibroblastoma é um tumor mesenquimatoso raro que, nos homens, se desenvolve ao nível do escroto, da região inguinal ou do períneo. Habitualmente este tumor é superfi e origina-se no tecido celular subcutâneo. No presente caso encontrámos um angiangiomiofibroblastoma com uma apresentação clinica diferente. Descrevemos um tumor benigno que, do ponto de vista clinico e imagiológico, mimetizava um tumor do testículo. Este tumor encontrava-se ligado aos vasos da circulação esplâncnica/mesentérica e ao epiploon e fazia herniação para o escroto através de uma volumosa hérnia inguinal. A ressecção cirúrgica é o tratamento recomendado para estes tumores, com a cura a ser obtida na maioria dos casos.
Angiomyofibroblastoma-like tumor is a rare mesenchymal tumor that occurs in men. Its name is based on similarities with the female angiomyofibroblastoma. The histogenesis of this tumor is the subject of speculation, with some evidence suggesting an origin from a perivascular mesenchymal cell. We describe an angiomyofibroblastoma-like tumor with a different clinical presentation and probably a different origin compared to cases described previously.
Case reportA 37-year-old man with no relevant medical history presented with an increased volume of the right testicle with a two-year evolution.
Clinically, in the right scrotum we palpated a tender, homogeneous and nonpainful mass of approximately 10cm; the epididymis and testicle could not be isolated from this mass. No pathological inguinal nodes were detected.
Ultrasonography detected a pronounced increase in the volume of the right testicle, with a 5.6cm cephalocaudal diameter, hipoecoic and diffusely heterogeneous; these aspects suggested an expansive lesion.
A Computed Tomography Scan of the pelvis and abdomen revealed a right testicle partially visualized with increased dimensions embedded in the context of a proliferative mass; the fat around the spermatic cord was prominent. Peri-testicular vascular ingurgitation was also present that seemed to have a connection with the splanchnic/mesenteric circulation.
Tumor markers for testicular cancer, β-HCG and α-FP, were within the normal range.
We assumed the patient had a testicular tumor and he was proposed to radical orchiectomy.
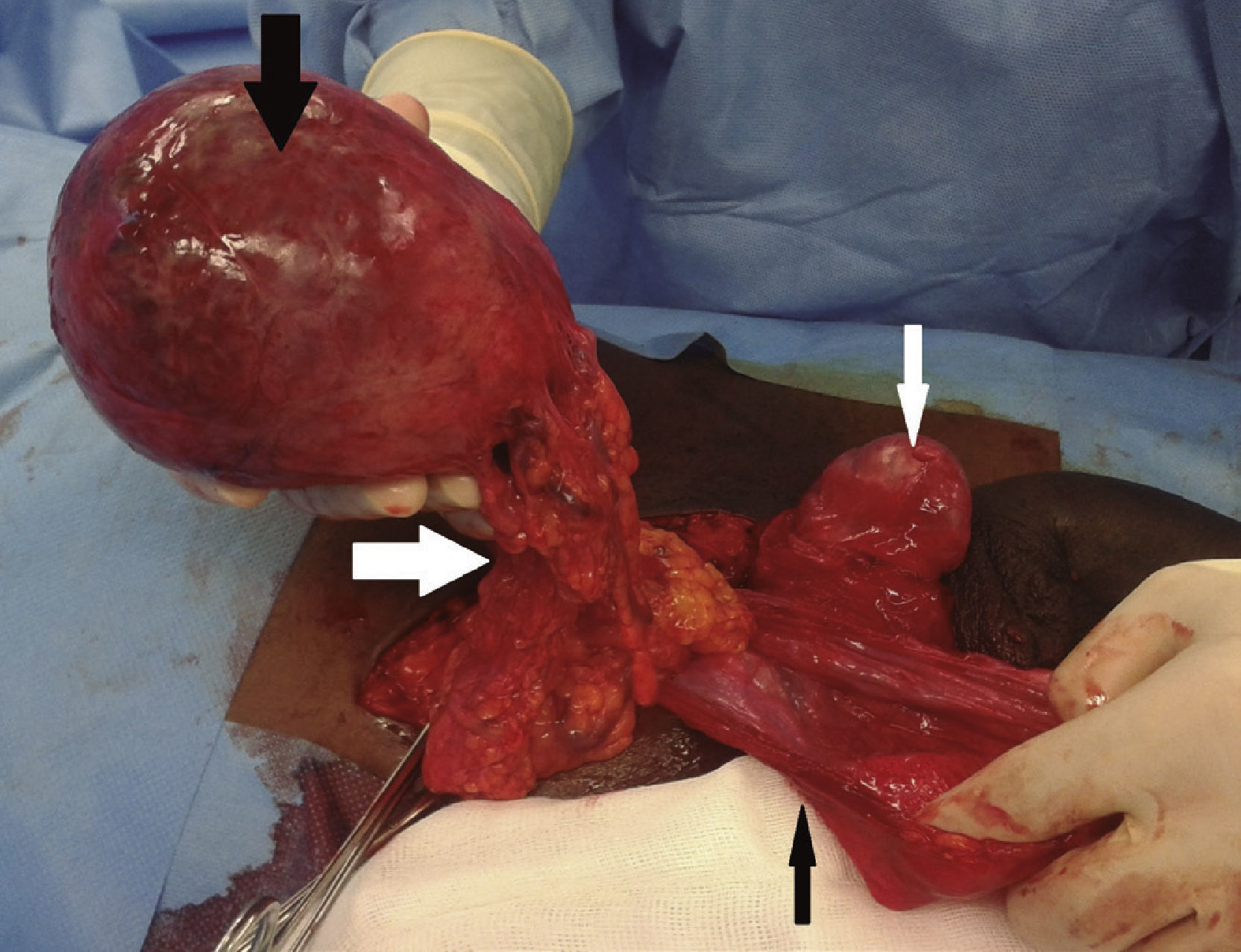
During the surgery, contrary to expectations, it was ascertained that inside the scrotum the patient had a healthy right testicle and spermatic cord together with an indirect inguinal hernia whose sac surrounded the large mass (Fig. 1).
 and spermatic cord together with an indirect inguinal hernia which sac (thin black arrow) was surrounding the big mass (thick black arrow); this mass was linked to the epiploon and splanchnic/mesenteric circulation (thick white arrow).")
Appearance of the structures inside the right scrotum of the patient during the surgery; inside the right scrotum the patient had a healthy right testicle (thin white arrow) and spermatic cord together with an indirect inguinal hernia which sac (thin black arrow) was surrounding the big mass (thick black arrow); this mass was linked to the epiploon and splanchnic/mesenteric circulation (thick white arrow).
The mass inside the herniary sac was completely separated from it and only fixed to a small portion of the omentum and vessels; this portion was ligated, the mass was completely removed and the indirect inguinal hernia was corrected.
This tumor measured 12 × 9.5 × 7.5cm and had a firm to soft consistency. Other macroscopic features included a solid cut surface, grey, with a brown/hemorrhagic stipple, and a central cystic hemorrhagic area of about 5cm.
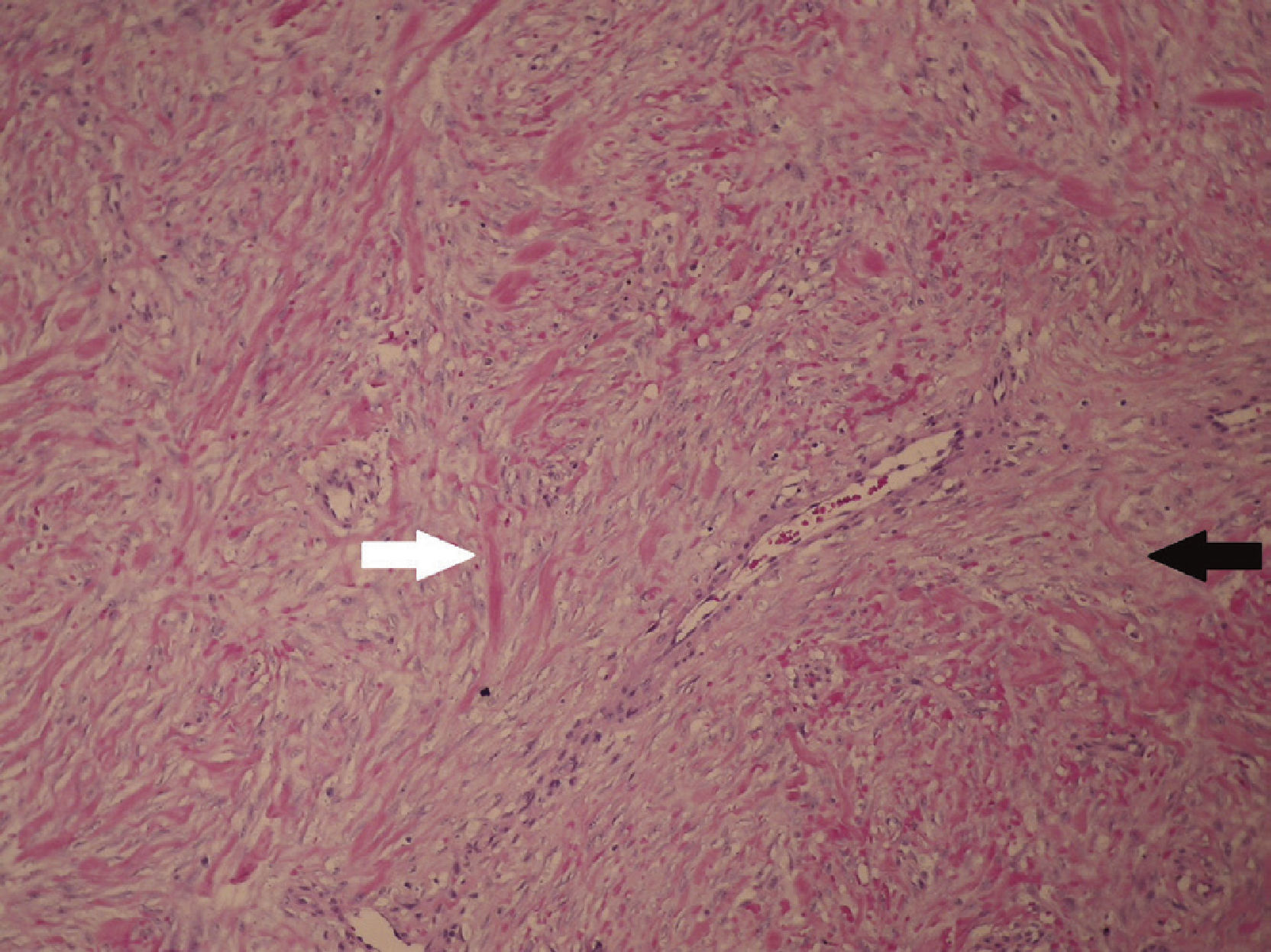
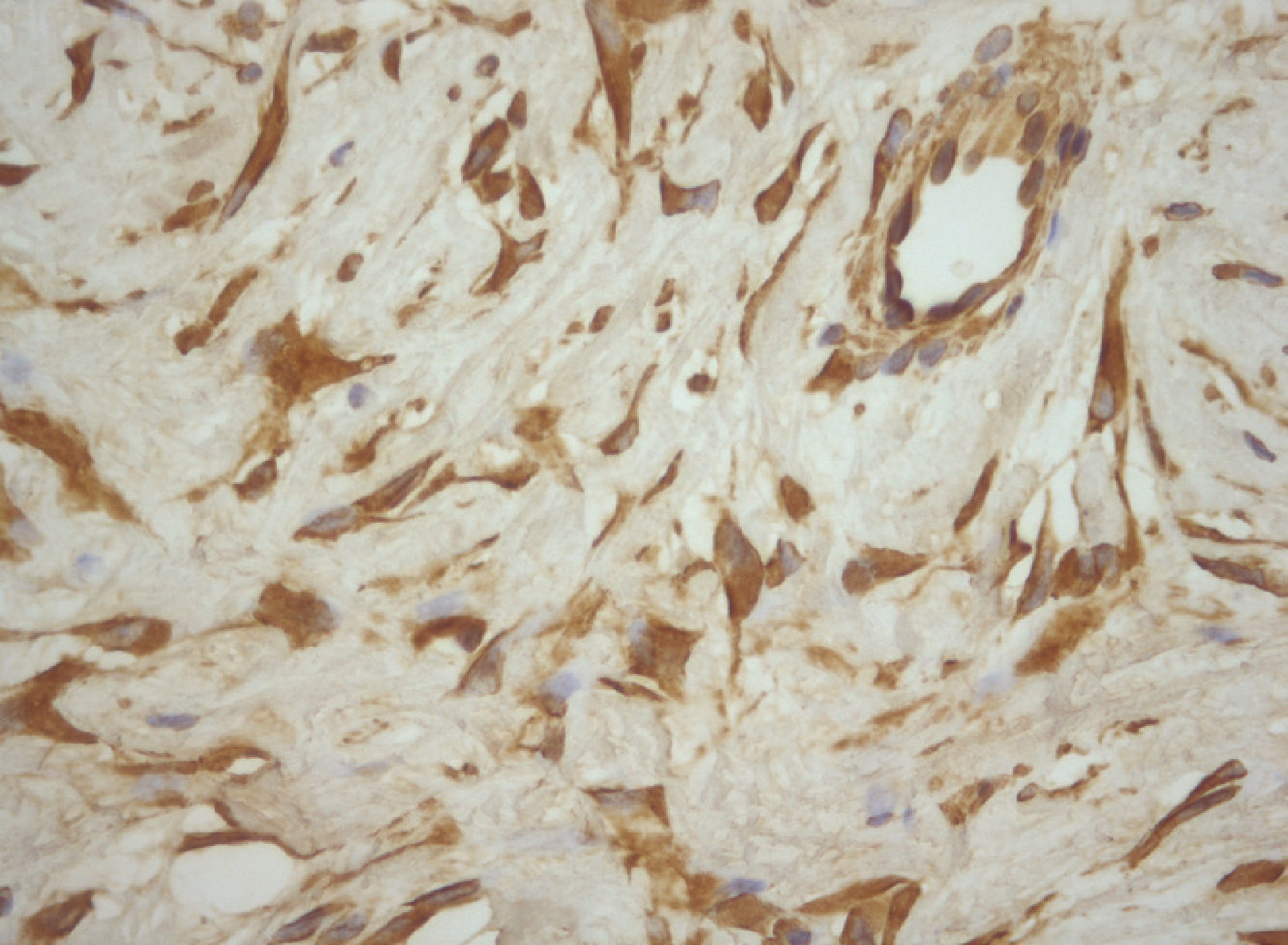
Microscopically, the tumor was a mesenchymal, spindled hypocellular proliferation, with cytonuclear atypia sparse or absent. These cells were in a stromal matrix containing small to medium sized blood vessels, composed of thick, eosinophilic collagen fibers with an admixture of thinner and lighter collagen fibers. Necrosis or mitotic figures were absent (Fig. 2). Immunohistochemical analysis showed that the neoplastic cells reacted positively with vimentin (Fig. 3) and focally with desmin. Immunoreactivity was negative for: smooth muscle actin, CD117, B-catenin, ALK, CKAE1-AE3, CA5.2, Calretin, WT1, trombomodulin, S100, CD68, CD99, bcl2 and IgG4.
 with an admixture of more thin and light collagen fibers (black arrow) (hematoxylin-eosin, ×100).")
Photomicrograph of the tumor reveals a mesenchymal, spindled hypocellular proliferation in a stromal matrix, containing small to medium size blood vessels, composed by thick, eosinophilic collagen fibers (white arrow) with an admixture of more thin and light collagen fibers (black arrow) (hematoxylin-eosin, ×100).
.")
The microscopic features and immunohistochemical profile were very suggestive that this mass could be an angiomyofibroblastoma-like tumor of the male genital tract.
After two years of follow-up, there was no evidence of recurrence.
DiscussionFletcher et al.1 in 1992 described a new type of mesenchymal tumor named angiomyofibroblastoma that arose in the vulva and was different from aggressive angiomyxoma, which was locally invasive.2
According to the authors1 the designation angiomyofibroblastoma was based on the two integral components of this tumor: the blood vessels and the stroma; this tumor is composed of relatively bland spindled appearing cells and a loosely collagenous stroma with numerous small and medium sized vessels.3–7 Vessels are usually rounded but occasionally compressed, with perivascular fibrosis; intralesional fat may be present.7–9 There are differences between the clinical forms of these tumors in men and women.
Concerning immunohistochemical analysis, angiomyofibroblastoma reacts positively and diffusely with vimentin1,5–7,9,10 and has variable expression of desmin,1,4–7,9,10 CD34,1,3–8 smooth muscle actin5,7,8,10 estrogen and progesterone receptors.5,7–9
The histogenesis of angiomyofibroblastoma is a subject of speculation,3,9 but Laskin et al. consider that derivation of this tumor from a perivascular mesenchymal cell, with a capacity for fatty and myofibroblastic differentiation under environmental influences, cannot be excluded.7,9 This progenitor cell could be related to the CD-34 positive fibroblast-like cells that normally exist around the vessels. Theoretically, this cell may lose its ability to express CD-34 with myofibroblastic differentiation,7 in male angiomyofibroblastoma.
Angiomyofibroblastoma-like tumor is a rare mesenchymal tumor that occurs in men in the scrotum,3,4,7,8,10 inguinal region,3,4,7,8,10 and perineum.3 This tumor was first described in 1997 as a cellular angiofibroma; its name was changed to angiomyofibroblastoma-like tumor by Laskin et al. in 19987 due to its similarities with the angiomyofibroblastoma tumor described in women in 1992.3,8
Angiomyofibroblastoma-like tumor is a superficial, well marginated and indolent tumor,3,6–8,10 ranging in size from to 14cm.7,10 It is usually asymptomatic but is occasionally associated with pain.3,5,7–10 The majority of cases described occur during the fifth to eight decades.3,4,6
In our case study we have an indolent and superfi 12cm tumor that appears in the scrotum, all characteristics of an angiofibroblastoma-like tumor; but, instead of arising from the subcutaneous tissues as usual, it seems to have developed from an atypical structure for this type of tumor, the omentum and mesenteric/splanchnic circulation, the only structures linked to the mass; it was identifi in the scrotum only because it was herniated through an indirect inguinal hernia.
Mesenchymal tumors are described as having a relationship with inguinal hernias,2,6 Some authors believe that the angiomyofibroblastoma-like tumor, could clinically simulate a hernia or a hydrocele,7,9,10 but in the available literature we do not find a description of this type of tumor herniated to the scrotum or linked to the omentum.
The recommended treatment for these tumors is surgical excision.3,6,8,10 The lesion is usually non recurrent,1,8–10 with only one case of recurrence described thirteen years after surgery.7
In conclusion, we describe an angiomyofibroblastoma-like tumor with a different clinical presentation and probably a different origin compared to the cases described before; in this case report the tumor had a subcutaneous presentation simulating a testicular tumor but apparently did not arise from the subcutaneous tissues of the scrotum, perineum or inguinal region as usual3,4,7,8,10 but from the omentum and the vessels of the mesenteric circulation, the only structures linked to the mass.
Ethical disclosuresProtection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Right to privacy and informed consent. The authors declare that no patient data appear in this article. The authors declare that no patient data appear in this article.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.The authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
