


Prevalence of allergic diseases and impaired pulmonary function may be high in children born prematurely. This study aimed to assess pulmonary function and prevalence of asthma, atopic diseases and allergic sensitisation in these patients.
MethodsA cross-sectional study was conducted with children aged 6–14 years who were born prematurely with birth weight <2000g from January 2008 to May 2011. Exclusion criteria were: major malformations, or acute respiratory disorders. The International Study of Asthma and Allergies in Childhood questionnaire was applied followed by allergic skin prick test and spirometry.
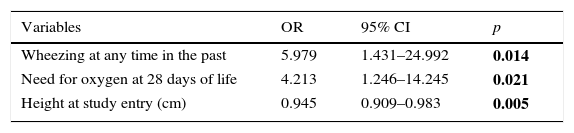
ResultsThe study included 84 children aged 9.3±2.3 years born at mean gestational age of 31.8±2.4 weeks. The prevalence of current asthma was 25%, more severe asthma was 15.5%; rhinitis was 38.1%; flexural eczema was 8.3%; and a positive skin-prick test was 69.6%. Frequencies of children with values <80% of predicted were: FVC (8.3%), FEV1 (22.6%), and FEV1/FVC ratio (16.7%). Prevalence of children with FEF25–75% <70% of the predicted value was 32.4%, positive bronchodilator response was observed in 20.5% of cases, and altered pulmonary function in 42.9%. Factors associated with altered pulmonary function were oxygen dependency at 28 days of life (OR: 4.213, p=0.021), the presence of wheezing in childhood (OR: 5.979, p=0.014) and infant's height (OR: 0.945, p=0.005).
ConclusionsThere was a high prevalence of severe asthma, allergic sensitisation, and altered pulmonary function among children and adolescents born prematurely. Bronchopulmonary dysplasia and a history of wheezing were risk factors for altered pulmonary function.
Bronchopulmonary dysplasia (BPD), mechanical ventilation, and oxygen therapy during neonatal intensive care unit hospitalisation are factors associated with bronchial hyperreactivity and asthma.1
Mai et al.2 observed higher prevalence of asthma at 12 years of age in children born prematurely, compared to those born at full term (22% vs. 9%, p=0.046), especially those who required mechanical ventilation (60% vs. 28%, p=0.050).
Few studies have assessed allergic sensitisation in children who were born prematurely with controversial results. Guimarães et al.3 observed a similar prevalence of positive skin prick tests (SPT) in very low birth weight preterm children aged 5–9 years with and without BPD (30.8% vs. 26.5%, p=0.742). However, Siltanen et al.4 observed that young adults that had been born prematurely had a lower chance of having a positive SPT compared to children born at full term (OR: 0.43; 95% CI: 0.23–0.79).
With regard to the pulmonary function, Broström et al.5 showed that children aged 6–8 years who were born at <32 weeks of gestation, with respiratory distress syndrome and BPD presented higher frequency of forced expiratory volume (FEV1) ≤80% of predicted value, compared to those without BPD. Even children who did not develop BPD could present with pulmonary function alterations resulting from premature birth, including expiratory flow limitations and decreased FEV1 and FEF25–75% values.5
In this context, the objective of this study was to analyse the prevalence of symptoms of asthma and atopic diseases, allergic sensitisation and altered pulmonary function and to determine the factors associated with altered pulmonary function in children and adolescents who were born prematurely.
MethodsThis cross-sectional study was approved by the institution's research ethics committee and each patient's parent provided written informed consent. Inclusion criteria were: children and adolescents aged 6–14 years who were born at <37 weeks of gestation and birth weight <2000g. These patients were in follow-up at the outpatient clinic for preterm infants of the Federal University of São Paulo, Brazil, from January 2008 to May 2011.
Patients with major congenital malformations or acute respiratory disease over the previous 15 days were excluded from the study. For each patient, the following steps were carried out: a parent questionnaire standardised by the International Study of Asthma and Allergies in Childhood (ISAAC)6 to determine the prevalence of symptoms of asthma, rhinitis, and flexural eczema; allergic sensitisation to aeroallergens performing SPT; spirometry; and collection of clinical and demographic data of the premature children by medical record review and parent questioning.
Skin prick test was performed employing standardised battery of standardised aeroallergens: Dermatophagoides pteronyssinus, Blomia tropicalis, cat and dog epithelia, fungal mix, and Blattella germanica, as well as a positive control (histamine chlorhydrate [1mg/mL]) and a negative control (diluent solution used in the extracts),7 according to that standardised by Pepys.8 A wheal with a mean diameter higher than 3mm identified SPT as positive, while the negative control was equal to zero and the positive control was ≥3mm.8
Current standardised pulmonary function testing was conducted according to the 1st Brazilian Consensus on Spirometry9 and ATS/ERS Task Force 200510 with Pony FX spirometer, Cosmed, after daily calibration. Each patient completed at least three reproducible flow volume curves before and 15min after the inhalation of salbutamol 400μg (Flumax® aerosol spacer). Forced vital capacity (FVC), FEV1, forced expiratory flow between 25% and 75% of FVC (FEF25–75%), FEV1/FVC ratio, and response to inhaled bronchodilator were assessed.
The spirometric values were analysed in relation to the percentage of predicted values by Polgar and Promadhat.11 Bronchodilator response was calculated as a percentage of increase in relation to the predicted FEV1 value as described by Pellegrino et al.,12 considering significant values ≥12% of predicted. Patients were defined as having normal pulmonary function when their FVC and FEV1 values and FEV1/FVC ratios were ≥80% of the predicted value and their FEF25–75% values were ≥70% of the predicted value. When an isolated FVC (pre and post bronchodilator) value was <80% of the predicted value, the patient was considered to have a restrictive disorder. When the FEV1 value and the FEV1/FVC ratio were <80% of the predicted value or the FEF25–75% value was <70% of the predicted value, the patient was considered to have an obstructive disorder. When the FVC and FEV1 and the FEV1/VFC ratios and/or FEF25–75% values were altered, the patient was considered to have a mixed obstructive and restrictive disorder.
The following data were collected for children and adolescents: gestational age with the best obstetric estimate or paediatric assessment13 birth weight, mode of delivery, gender, Apgar score, clinical complications in the neonatal unit, and need for medical procedures.
On the date of inclusion in the study, the following information was collected: chronological age, weight, height, body mass index, history of disease and hospitalisation occurrence after neonatal unit discharge, regular physical activity, and breastfeeding.
Statistical analysisA convenience sample of children and adolescents aged 6–14 who fit the eligible criteria was included. The numerical variables were expressed as mean and standard deviation or median and minimum and maximum values. These variables were compared using t-tests or Mann–Whitney tests. Categorical variables were expressed as number and percentage and compared by χ2 test or Fisher's exact test.
Factors associated with altered pulmonary function were studied by univariate logistic regression considering the clinical variables that may have interfered with pulmonary function. Then, variables with clinical interest and a statistical significance level of p<0.2 in the univariate analysis were included in the multiple logistic regression model. The statistical analyses were conducted using the SPSS for Win/v.17.0 (IBM SPSS Statistics, Somers, NY, USA), considering p<0.05 as significant.
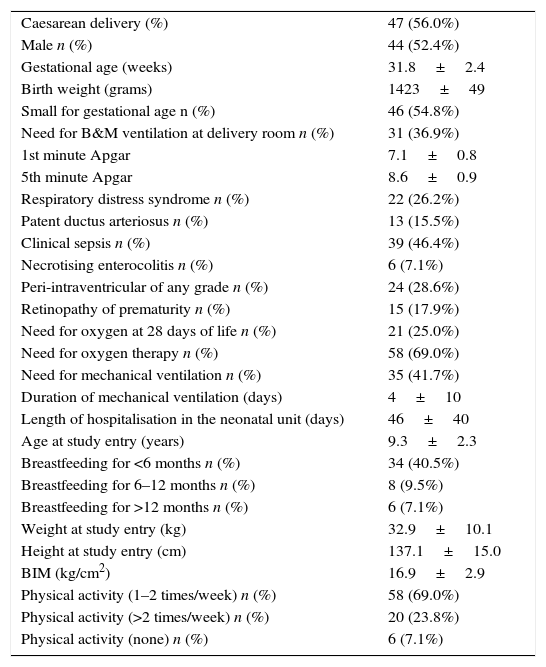
ResultsDuring the study period, a total of 166 children and adolescents were in follow-up at the premature out clinic of the institution. Of these, 48 (28.9%) children were excluded, 44 for moderate or severe neurological alterations, two with Down syndrome, and two with complex cardiopathy. Of the 118 eligible children, 14 (11.9%) did not agree to participate, two (1.7%) were excluded due to incomplete pulmonary function results, and 18 (15.3%) were excluded due to a technical fault in the spirometry manoeuvres. Therefore, 84 (71.2%) children and adolescents were ultimately studied. These children's demographic and clinical characteristics are presented in Table 1.
Children's demographic and clinical characteristics.
| Caesarean delivery (%) | 47 (56.0%) |
| Male n (%) | 44 (52.4%) |
| Gestational age (weeks) | 31.8±2.4 |
| Birth weight (grams) | 1423±49 |
| Small for gestational age n (%) | 46 (54.8%) |
| Need for B&M ventilation at delivery room n (%) | 31 (36.9%) |
| 1st minute Apgar | 7.1±0.8 |
| 5th minute Apgar | 8.6±0.9 |
| Respiratory distress syndrome n (%) | 22 (26.2%) |
| Patent ductus arteriosus n (%) | 13 (15.5%) |
| Clinical sepsis n (%) | 39 (46.4%) |
| Necrotising enterocolitis n (%) | 6 (7.1%) |
| Peri-intraventricular of any grade n (%) | 24 (28.6%) |
| Retinopathy of prematurity n (%) | 15 (17.9%) |
| Need for oxygen at 28 days of life n (%) | 21 (25.0%) |
| Need for oxygen therapy n (%) | 58 (69.0%) |
| Need for mechanical ventilation n (%) | 35 (41.7%) |
| Duration of mechanical ventilation (days) | 4±10 |
| Length of hospitalisation in the neonatal unit (days) | 46±40 |
| Age at study entry (years) | 9.3±2.3 |
| Breastfeeding for <6 months n (%) | 34 (40.5%) |
| Breastfeeding for 6–12 months n (%) | 8 (9.5%) |
| Breastfeeding for >12 months n (%) | 6 (7.1%) |
| Weight at study entry (kg) | 32.9±10.1 |
| Height at study entry (cm) | 137.1±15.0 |
| BIM (kg/cm2) | 16.9±2.9 |
| Physical activity (1–2 times/week) n (%) | 58 (69.0%) |
| Physical activity (>2 times/week) n (%) | 20 (23.8%) |
| Physical activity (none) n (%) | 6 (7.1%) |
B&M: bag and mask; BIM: body mass index.
Following discharge from the neonatal unit, 48 (57.1%) children were hospitalised, 22 (45.6%) for pneumonia, 19 (39.6%) for bronchospasm crisis, four (8.3%) for surgical inguinal hernia repair and two (4.4%) for tonsillectomy.
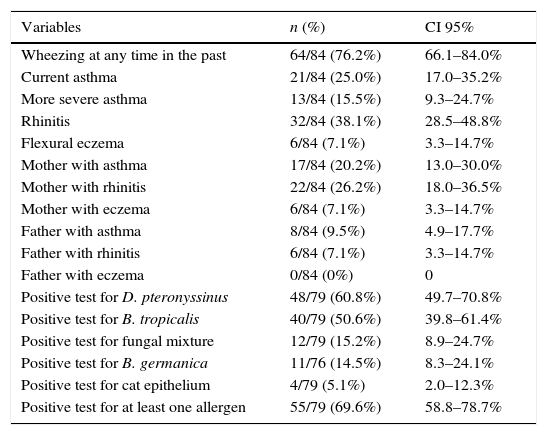
The prevalence of symptoms of asthma, rhinitis, flexural eczema and positive SPT in studied children and history of atopic diseases in their parents are shown in Table 2. Of 64 children who presented wheezing at any time in the past, 21 (32.8%) developed current asthma.
Prevalence of current asthma, rhinitis, flexural eczema and positive skin test among studied children and history of atopic diseases in their parents.
| Variables | n (%) | CI 95% |
|---|---|---|
| Wheezing at any time in the past | 64/84 (76.2%) | 66.1–84.0% |
| Current asthma | 21/84 (25.0%) | 17.0–35.2% |
| More severe asthma | 13/84 (15.5%) | 9.3–24.7% |
| Rhinitis | 32/84 (38.1%) | 28.5–48.8% |
| Flexural eczema | 6/84 (7.1%) | 3.3–14.7% |
| Mother with asthma | 17/84 (20.2%) | 13.0–30.0% |
| Mother with rhinitis | 22/84 (26.2%) | 18.0–36.5% |
| Mother with eczema | 6/84 (7.1%) | 3.3–14.7% |
| Father with asthma | 8/84 (9.5%) | 4.9–17.7% |
| Father with rhinitis | 6/84 (7.1%) | 3.3–14.7% |
| Father with eczema | 0/84 (0%) | 0 |
| Positive test for D. pteronyssinus | 48/79 (60.8%) | 49.7–70.8% |
| Positive test for B. tropicalis | 40/79 (50.6%) | 39.8–61.4% |
| Positive test for fungal mixture | 12/79 (15.2%) | 8.9–24.7% |
| Positive test for B. germanica | 11/76 (14.5%) | 8.3–24.1% |
| Positive test for cat epithelium | 4/79 (5.1%) | 2.0–12.3% |
| Positive test for at least one allergen | 55/79 (69.6%) | 58.8–78.7% |
No association was found between symptoms of atopy in children or parents and current asthma in children. Asthma, rhinitis and eczema were referred by 20.2%, 26.2% and 4.8% of mothers, respectively. Eight (9.6%) and six (7.1%) fathers referred a history of asthma and rhinitis, respectively. History of eczema was not found among fathers. The frequency of symptoms of rhinitis (52.4% vs. 33.3%, p=0.120) and eczema (9.5% vs. 7.9%, p=1.000) was similar between children with or without current asthma. Also, the prevalence of asthma in mother (14.3% vs. 22.2%, p=0.329), rhinitis in mother (33.3% vs. 23.8%, p=0.390), eczema in mother (0% vs. 6.3%, p=0.309), asthma in father (14.3% vs. 8.1%, p=0.325), rhinitis in father (4.8% vs. 8.1%, p=0.523) was similar in children with and without current asthma. The frequency of any positive SPT was similar regardless of the presence of current asthma (77.8% vs. 67.2%, p=0.392) or wheezing at any time in the past (72.1% vs. 61.1%, p=0.372) in children.
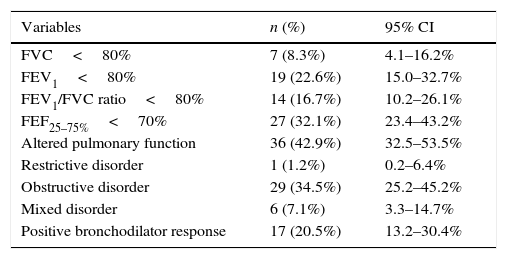
With regard to the pulmonary function of the 84 children, the median (minimum and maximum values) of the obtained values in relation to the expected values were: FVC, 93.0% (73.0–126.0%), FEV1, 87.5% (64.0–125.0%), FEV1/FVC ratio, 86.5% (66.0–98.0%), and FEF25–75, 79.0% (28.0–201.0%). The prevalence of altered parameters of pulmonary function is shown in Table 3.
Prevalence and 95% confidence interval (CI) of altered parameters of pulmonary function among included children (n=84).
| Variables | n (%) | 95% CI |
|---|---|---|
| FVC<80% | 7 (8.3%) | 4.1–16.2% |
| FEV1<80% | 19 (22.6%) | 15.0–32.7% |
| FEV1/FVC ratio<80% | 14 (16.7%) | 10.2–26.1% |
| FEF25–75%<70% | 27 (32.1%) | 23.4–43.2% |
| Altered pulmonary function | 36 (42.9%) | 32.5–53.5% |
| Restrictive disorder | 1 (1.2%) | 0.2–6.4% |
| Obstructive disorder | 29 (34.5%) | 25.2–45.2% |
| Mixed disorder | 6 (7.1%) | 3.3–14.7% |
| Positive bronchodilator response | 17 (20.5%) | 13.2–30.4% |
When specific parameters of the pulmonary function tests were analysed, we observed that the obtained values of FEV1 (84.2±10.0% vs. 90.0±11.7%; p=0.042) and FEF25–75% (75.0±24.9% vs. 88.7±31.6%; p=0.046) were lower in relation to the predicted values in premature who had respiratory distress syndrome in the neonatal period. These children more frequently presented with FEF25–75% values <70% of the predicted values (50.0% vs. 26.2%; p=0.041), compared with those who did not develop this syndrome.
The median FEV1/FVC ratios were significantly lower in the children with current asthma than in children without asthma. No associations were observed between rhinitis and flexural eczema or any other parameter of altered pulmonary function.
Predicted values of FEV1 (82.6±11.7% vs. 89.9±11.1%; p=0.019), FEV1/FVC ratios (80.7±7.0% vs. 86.2±6.5%; p=0.003) and FEF25–75% values (68.4±20.7% vs. 89.1±31.4%; p=0.012) were significantly lower in children who had a positive bronchodilator test, compared with those who had a negative response. In the same way, the percentage of children with FEV1/FVC ratio values <80% (58.8% vs. 26.2%; p=0.011) and FEF25–75% values <70% (35.3% vs. 12.1%; p=0.034) was higher in children with a positive bronchodilator test.
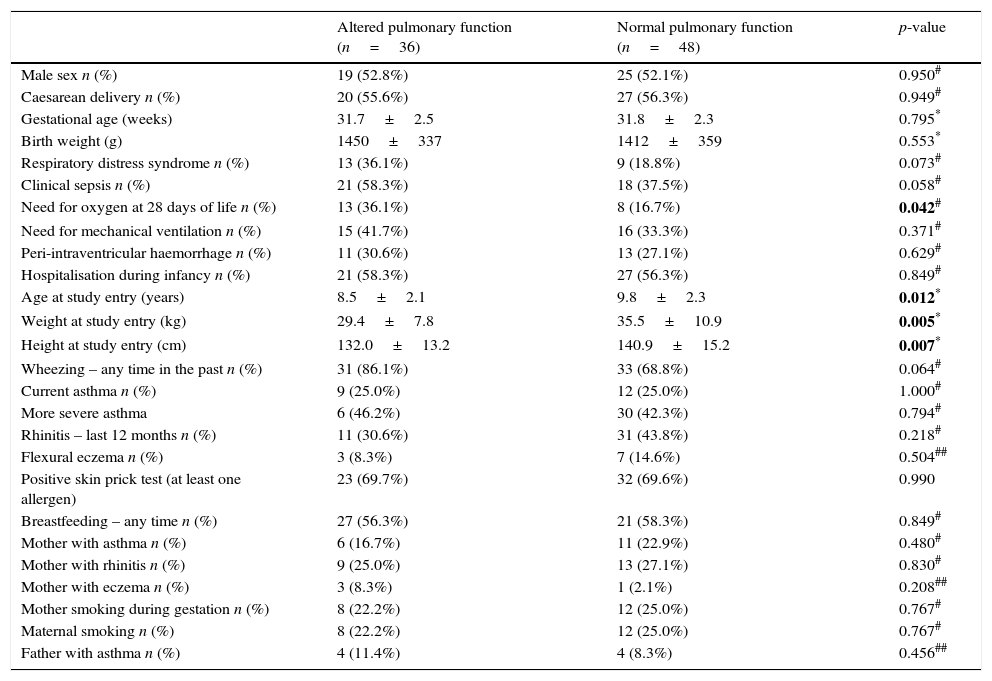
Comparisons of children's characteristics and parents’ history of atopy according to the result of pulmonary function are displayed in Table 4. Factors associated with altered pulmonary function assessed by logistic regression analysis are shown in Tables 5 and 6.
Children's characteristics and parents’ history of atopy according to the result of pulmonary function.
| Altered pulmonary function (n=36) | Normal pulmonary function (n=48) | p-value | |
|---|---|---|---|
| Male sex n (%) | 19 (52.8%) | 25 (52.1%) | 0.950# |
| Caesarean delivery n (%) | 20 (55.6%) | 27 (56.3%) | 0.949# |
| Gestational age (weeks) | 31.7±2.5 | 31.8±2.3 | 0.795* |
| Birth weight (g) | 1450±337 | 1412±359 | 0.553* |
| Respiratory distress syndrome n (%) | 13 (36.1%) | 9 (18.8%) | 0.073# |
| Clinical sepsis n (%) | 21 (58.3%) | 18 (37.5%) | 0.058# |
| Need for oxygen at 28 days of life n (%) | 13 (36.1%) | 8 (16.7%) | 0.042# |
| Need for mechanical ventilation n (%) | 15 (41.7%) | 16 (33.3%) | 0.371# |
| Peri-intraventricular haemorrhage n (%) | 11 (30.6%) | 13 (27.1%) | 0.629# |
| Hospitalisation during infancy n (%) | 21 (58.3%) | 27 (56.3%) | 0.849# |
| Age at study entry (years) | 8.5±2.1 | 9.8±2.3 | 0.012* |
| Weight at study entry (kg) | 29.4±7.8 | 35.5±10.9 | 0.005* |
| Height at study entry (cm) | 132.0±13.2 | 140.9±15.2 | 0.007* |
| Wheezing – any time in the past n (%) | 31 (86.1%) | 33 (68.8%) | 0.064# |
| Current asthma n (%) | 9 (25.0%) | 12 (25.0%) | 1.000# |
| More severe asthma | 6 (46.2%) | 30 (42.3%) | 0.794# |
| Rhinitis – last 12 months n (%) | 11 (30.6%) | 31 (43.8%) | 0.218# |
| Flexural eczema n (%) | 3 (8.3%) | 7 (14.6%) | 0.504## |
| Positive skin prick test (at least one allergen) | 23 (69.7%) | 32 (69.6%) | 0.990 |
| Breastfeeding – any time n (%) | 27 (56.3%) | 21 (58.3%) | 0.849# |
| Mother with asthma n (%) | 6 (16.7%) | 11 (22.9%) | 0.480# |
| Mother with rhinitis n (%) | 9 (25.0%) | 13 (27.1%) | 0.830# |
| Mother with eczema n (%) | 3 (8.3%) | 1 (2.1%) | 0.208## |
| Mother smoking during gestation n (%) | 8 (22.2%) | 12 (25.0%) | 0.767# |
| Maternal smoking n (%) | 8 (22.2%) | 12 (25.0%) | 0.767# |
| Father with asthma n (%) | 4 (11.4%) | 4 (8.3%) | 0.456## |
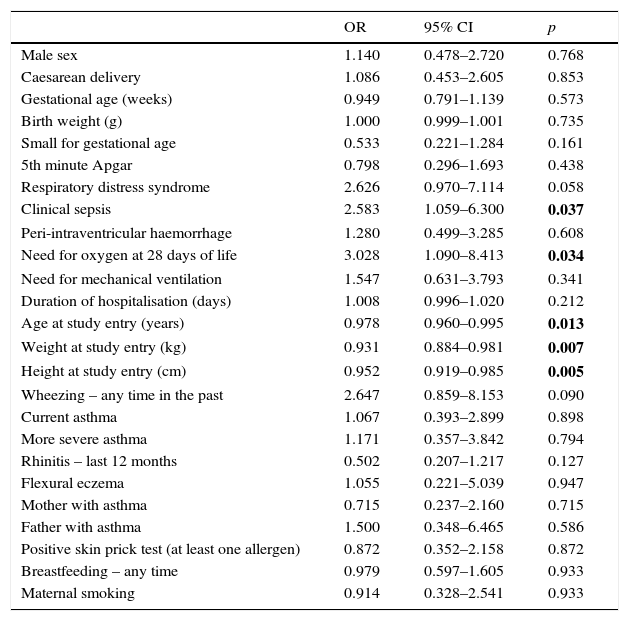
Univariate logistic regression analysis for factors associated with altered pulmonary function.
| OR | 95% CI | p | |
|---|---|---|---|
| Male sex | 1.140 | 0.478–2.720 | 0.768 |
| Caesarean delivery | 1.086 | 0.453–2.605 | 0.853 |
| Gestational age (weeks) | 0.949 | 0.791–1.139 | 0.573 |
| Birth weight (g) | 1.000 | 0.999–1.001 | 0.735 |
| Small for gestational age | 0.533 | 0.221–1.284 | 0.161 |
| 5th minute Apgar | 0.798 | 0.296–1.693 | 0.438 |
| Respiratory distress syndrome | 2.626 | 0.970–7.114 | 0.058 |
| Clinical sepsis | 2.583 | 1.059–6.300 | 0.037 |
| Peri-intraventricular haemorrhage | 1.280 | 0.499–3.285 | 0.608 |
| Need for oxygen at 28 days of life | 3.028 | 1.090–8.413 | 0.034 |
| Need for mechanical ventilation | 1.547 | 0.631–3.793 | 0.341 |
| Duration of hospitalisation (days) | 1.008 | 0.996–1.020 | 0.212 |
| Age at study entry (years) | 0.978 | 0.960–0.995 | 0.013 |
| Weight at study entry (kg) | 0.931 | 0.884–0.981 | 0.007 |
| Height at study entry (cm) | 0.952 | 0.919–0.985 | 0.005 |
| Wheezing – any time in the past | 2.647 | 0.859–8.153 | 0.090 |
| Current asthma | 1.067 | 0.393–2.899 | 0.898 |
| More severe asthma | 1.171 | 0.357–3.842 | 0.794 |
| Rhinitis – last 12 months | 0.502 | 0.207–1.217 | 0.127 |
| Flexural eczema | 1.055 | 0.221–5.039 | 0.947 |
| Mother with asthma | 0.715 | 0.237–2.160 | 0.715 |
| Father with asthma | 1.500 | 0.348–6.465 | 0.586 |
| Positive skin prick test (at least one allergen) | 0.872 | 0.352–2.158 | 0.872 |
| Breastfeeding – any time | 0.979 | 0.597–1.605 | 0.933 |
| Maternal smoking | 0.914 | 0.328–2.541 | 0.933 |
Final model of logistic regression analysis for factors associated with altered pulmonary function.
| Variables | OR | 95% CI | p |
|---|---|---|---|
| Wheezing at any time in the past | 5.979 | 1.431–24.992 | 0.014 |
| Need for oxygen at 28 days of life | 4.213 | 1.246–14.245 | 0.021 |
| Height at study entry (cm) | 0.945 | 0.909–0.983 | 0.005 |
p<0.001. Model adjusted for the following variables: small for gestational age, presence of respiratory distress syndrome, clinical sepsis and rhinitis in the last 12 months.
In this study, the prevalence of current asthma was 25%, similar to the finding of Mai et al.2 in children aged 12 years who were born prematurely with very low birth weight. The prevalence of current asthma in this study was similar in children with and without BPD, similar to that observed by Guimarães et al.3 This prevalence was also similar to that found in adolescents in Brazil,14 but higher than found by Oliveira-Santos15 in children and adolescents of northeast Brazil using the same ISAAC questionnaire.
The prevalence of more severe asthma in this study was 15.5% higher than that reported in the literature of 1–3% in general population.16 Another study showed a severe asthma prevalence of 0–20.3% in children and 0.1–16% in adolescents in India and Costa Rica, respectively.17 The higher prevalence of severe asthma found in our study could be explained by different diagnostic criteria used in these studies. The other alternative reason might be the high frequency of neonatal sepsis found in this study. The use of antibiotics in early life has been associated with asthma and atopic diseases, although conclusive research on this association is still missing.18,19
As described previously, in the current study, the frequency of wheezing at any time in the past was greater than the frequency of wheezing within the last 12 months. The higher prevalence of wheezing ever can be explained by the higher occurrence of wheezing symptoms in preterm infants,20 which could explain the high rate of re-hospitalisation of children born prematurely after delivery from the neonatal unit.21 Preterm infants are prone to acquire respiratory virus infection and develop bronchiolitis early in life. Prevention of these infections might protect against future asthma since one third of children with wheezing at any time in the past developed current asthma.
In the current study, the prevalence of rhinitis within the last 12 months (38.1%) was higher than that observed by Solé et al.22 in children (12.8%) and adolescents (18.0%) but similar to the 30.1% prevalence reported by Pastorino et al.23 in adolescents.
The association between asthma and rhinitis has been described with relative frequency.24,25 Bousquet et al.24 reported that 10–40% of patients with allergic rhinitis also had asthma. In the present study we also observed a higher frequency of asthma in children with rhinitis.
The prevalence of flexural eczema within the last 12 months was similar to that reported by a study of children and adolescents conducted in Latin American countries (11.3% in children aged 6–7 years and 10.6% in adolescents aged 13–14 years).26,27
The frequency of a positive SPT to at least one allergen was high, with the highest positive results for D. pteronyssinus. This prevalence was higher than that found in adolescents, from the same region of this study, born at term. Pastorino et al.23 studied 996 adolescents of São Paulo (the same city as the present study) added to adolescents from Rio de Janeiro and found 46.8% of positive test for at least one allergen. Sarinho et al.28 developed a case control study, with 200 adolescents from the Northeast region of Brazil and found a frequency of positive skin test for 38.5% of included adolescents, being higher in asthmatic adolescent (54%), compared to those non-asthmatic (33.3%), p=0.009. Similar to our study, D. pteronyssinus was the most frequent allergen found in SPT in both studies. These findings may suggest that preterm infants might develop symptoms of sensitisation more frequently.
The association between allergic sensitisation and asthma or rhinitis has been described with relative frequency.22 However, this association was not observed in this study, and the small sample size provides a possible explanation for it.
The prevalence of altered pulmonary function in this study was 42.9%, lower than the 56% prevalence described by Fawke et al.27 in children aged 11 years who were born at <25 weeks’ gestation. Doyle et al.29 observed a 30.3% frequency of FEV1 <75% in adolescents with a mean age of 18.9 years who were born prematurely with very low birth weight and who had developed BPD. Methodological differences between the two studies may explain these differences. Doyle et al.29 adopted a lower cut-off value for defining altered pulmonary function and included older patients as well as children born during the pre-surfactant era.
Studies have shown patterns of obstructive disorders in children and adolescents who were born prematurely, mainly in those who also developed BPD. They presented mean values of 60–80% of the predicted FEV1 and FEF25–75% and FEV1/FVC ratios,30 are similar to those found in this study.
Using FEV1 <80% of the predicted values, a frequency of obstructive disorders of 22.6% was found. When the FEV1/FVC ratio was used, the prevalence of the obstructive disorder was 16.7%, while that for FEF25–75% <70% was 32.4%. When the bronchodilator response was assessed, a positive response was observed in 20.5% of children. These data show that in regard to pulmonary function, the most compromised parameters indicated a predominance of obstructive disorder, a finding that was in accordance with those of other studies.5 Otherwise, the FVC, a marker of the restrictive process, was less pronounced but was similar to those observed by other researchers.31 It is possible that this parameter improves with age and lung growth, whereas changes in the small airways persist over a longer period of time. This finding suggests a diverse mechanism of lesions and repair of the pulmonary parenchyma and airways.1 This hypothesis is in accordance with the result of the present study, with the logistic regression analysis showing that the likelihood of altered pulmonary function decreased with children's growth.
In this study, we observed no association between allergic sensitisation or family history of atopy and altered pulmonary function. The risk factors associated with altered pulmonary function were wheezing at any time in the past and oxygen dependency at 28 days of life. This result highlights the role of premature birth, the development of lung disease during the neonatal period and early post-neonatal morbidity on lung function. As previously described, preterm-born children, especially those who develop BPD during neonatal period, are more likely to have lung function abnormalities in the childhood. Bolton et al.32 observed that children aged 11 years born before 25 weeks of gestation had worse pulmonary function and a significant difference in FEV1, FVC, FEV1/FVC, and FEF25–75% values, compared to children born at term. There was even a difference between the children who required oxygen and those who did not require oxygen at 36 weeks of corrected age. Also, Vom Hove et al.33 found that children aged 9.5 years with a history of BPD had significantly lower values for FEV1 (p=0.008), FVC (p=0.022), and FEF50% (p=0.048) compared with preterm children without previous BPD.
On the other hand, the contribution of age and adequate growth of the children on pulmonary function is highlighted by the result of our regression analysis. According to Bhandari and Panitch (2006),1 the development of the child with age may decrease the pulmonary restrictive lesions and improve pulmonary function, as seen in the present study.
One limitation of this study is the small sample size and the lack of a formal sample size calculation, which preclude definitive conclusions.
ConclusionsIn conclusion, the prevalence of severe asthma, allergic sensitisation, and altered pulmonary function in children and adolescents who are born prematurely were high. Risk factors associated with altered pulmonary function included a history of bronchopulmonary dysplasia and wheezing at any time in the past; infant's growth appears to play a protective role for pulmonary function.
Authors’ contributions- •
Cristiana Gonçalves contributed to the conception and design of the study, collected clinical data, performed the lung tests, drafted the article and approved the final version of the manuscript.
- •
Gustavo Wandalsen: contributed for the conception and design of the study, supervised and performed the lung tests, analysed the data and critically revised and approved the final version of the manuscript.
- •
Fernanda Lanza: supervised and performed lung tests, analysed the data and critically revised and approved the final version of the manuscript.
- •
Ana Lucia Goulart contributed to the conception of the study, collected clinical data, critically revised and approved the final version of the manuscript.
- •
Dirceu Solé contributed to the conception and design of the study, supervised the lung tests, analysed and interpreted the data and critically revised and approved the final version of the manuscript.
- •
Amélia Miyashiro Nunes dos Santos: contributed to the conception and design of the study, supervised the study, analysed and interpreted data, drafted the manuscript and critically revised it and approved the final version of the manuscript.
The authors declare that they have followed the protocols of their work centre on the publication of patient data and that all the patients included in the study have received sufficient information and have given their informed consent in writing to participate in that study.
Right to privacy and informed consentThe authors have obtained the informed consent of the patients and/or subjects mentioned in the article. The author for correspondence is in possession of this document.
Protection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the responsible Clinical Research Ethics Committee and in accordance with those of the World Medical Association and the Helsinki Declaration.
Conflict of interestAll authors declare that have no conflict of interest to declare.
