




A 69-year-old man with an history of liver cirrhosis complicated by hepatocellular carcinoma treated by chemoembolization, moderate mitral insufficiency and chronic atrial fibrillation presented with a rounded calcified opacity in right upper abdomen at chest radiography. Abdominal computed tomography scan showed an omogeneous and complete uptake of lipiodol within the hepatocellular carcinoma, without signs of viable tumor tissue. Since lipiodol is radiopaque when intensely concentrated within liver nodules, it can appear as calcification on abdominal or even thoracic plain-film radiograph, as in this case. The differential diagnosis of calcified hepatic lesions includes tubercular granuloma, Echinococcus cyst, large hemangioma, hepatocellular adenoma, fibrola-mellar carcinoma, intrahepatic cholangiocarcinoma, and liver metastases.
Case ReportA 69-year-old man presented for an outpatient follow-up visit. The patient had hepatitis B virus-related cirrhosis and had undergone chemoembolization three months before because of hepatocellular carcinoma of 6 cm of VIII segment. He had an history of moderate mitral insufficiency, chronic atrial fibrillation and benign prostatic hyperplasia. His medications included warfarin, carvedilol, furosemide, spironolactone, lamivudine, finasteride and rabepra-zole. He reported some episodes of nocturnal dyspnea and cough, but on physical examination showed no evidence of congestive heart failure. Laboratory tests revealed compensated cirrhosis in Child A status. Alpha fetoprotein was 1 ng/mL. A chest radiograph (Figure 1) showed cardiomegaly associated with an increased width of the vascular pedicle and a rounded calcified opacity in right upper abdomen.

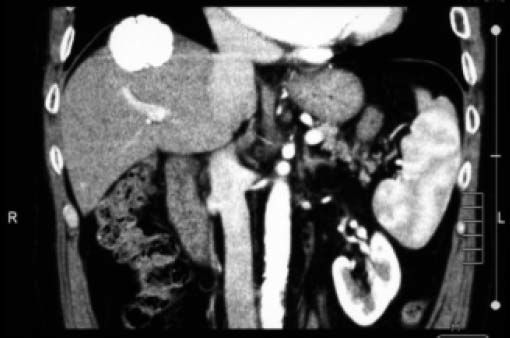
Abdominal computed tomography scan (Figure 2) showed an omogeneous and complete uptake of lipiodol within the hepatocellular carcinoma. In arterial phase, no viable tumor tissue was detected, suggesting a complete response. Since lipiodol is radiopaque when intensely concentrated within liver nodules, it can appear as calcification on abdominal or even thoracic plain-film radiograph, as in this case.

Although relatively uncommon in daily clinical practice, intrahepatic calcifications may be found in inflammatory and neoplastic diseases. The most common source of calcified hepatic lesions are tubercular granuloma (usually small and multiple), Echinococcus cyst (tipically as peripheral calcified rim), large hemangioma (central coarse calcifications), hepatocellular adenoma, fibrolamellar carcinoma, intrahepatic cholangio-carcinoma, and liver metastases, especially from colon carcinoma.1 When evaluating an intrahepatic calcification in patients treated with chemo-embolization, an intranodular lipiodol uptake should be keep in mind.



