










Background Cirrhosis remains the most frequent liver-related cause of death worldwide and we aimed to evaluate its burden in Brazil from 2000 to 2012.
Material and methods The Brazilian National Death Registry was analyzed from 2000 to 2012. Death by cirrhosis was defined by the presence of I85, K73 and/or K74 ICD-10 codes in contributing or underlying causes of death on the death certificate (DC). Crude mortality rates were calculated as the ratio of the absolute number of deaths and the estimated population. Mortality rates were age-adjusted by the direct standardization method using the WHO standard population
Results. A total of 265,180 deaths where cirrhosis was mentioned on the DC [77% male, aged 56 years] occurred from 2000 to 2012. Cirrhosis codes were present in 46% of liver-related deaths and 2% of all deaths in this period. Despite an increase in the absolute number of deaths (n = 18,245 to 22,340), the age-standardized mortality rates (95%CI) decreased from 13.32 (13.16-13.48) to 11.71 (11.59-11.83) per 100,000 inhabitants from 2000 to 2012 (p < 0.001). This trend was not uniform across the country, with decreases in death rates in the South [14.46 (14.07-14.87) to 10.89 (10.59-11.19)] and Southeast [15.85 (15.6-16.09) to 12.52 (12.34-12.70)] and increases in the North [8.84 (8.24-9.43) to 11.53 (11.08-11.99)] and Northeast [9.41 (9.13-9.69) to 10.93 (10.68-11.17)] (p < 0.001 for all)
Conclusion. Cirrhosis remains a major public health issue, despite the reduction in mortality rates in the last decade.
Identification of major public health issues is the first step in implementing programs to prevent, perform early diagnosis and treat high burden diseases. Chronic liver diseases have emerged as major causes of global health burden and have led to an increasing economic impact on health care systems.1 Direct and indirect costs for liver disease management have substantially increased nowadays, especially in the era of interferon-free treatment for hepatitis C.2
Liver-related mortality rates have been increasing worldwide. Several studies have described the burden of liver disease in the United States3,4 and Europe.5 This trend was followed in Latin America, where approxima-tively 2 million cases of chronic liver disease are expected in the next 40 years.6 Liver cirrhosis has been described as the most frequent liver-related cause of death worldwide.7
The top leading causes of cirrhosis are viral hepatitis, alcohol abuse and non-alcoholic fatty liver disease. Patients with cirrhosis have 3-fold higher risk of overall mortality than matched controls.8 However, few studies have evaluated the burden of liver disease in low- or middle-income countries, such as Brazil. The aim of this study was to estimate mortality rates associated with cirrhosis in Brazil from 2000 to 2012.
Material and MethodsThis is an analytic ecological study performed at the Evandro Chagas National Institute of Infectious Disease (INI/FIOCRUZ). The National Registry of Death database (SIM - Sistema de Informação sobre Mortalidade) from the Brazilian Unified Health System Information Technology Department (DATASUS) was analyzed to estimate the age-adjusted mortality rates associated with cirrhosis from 2000 to 2012.
The study protocol was conducted in accordance with the Helsinki Declaration and it was approved by the local Ethics Committee. SIM is an open-source and web available database (www.datasus.gov.br) published in a public domain and provided by the Brazilian Ministry of Health. This database contains anonymous data for all deaths in Brazil since 1979. Primary, secondary and contributing causes of death, based on the death certificate (DC) have been electronically registered in SIM since 1999. The underlying cause of death is determined as the “disease of injury which initiates the train of events leading directly to death”. If more than one cause or condition were listed on the DC, the underlying cause was determined by the sequence of conditions using standard algorithms.9 Causes of death have been classified according to the 10th revision of the International Classification of Diseases (ICD-10) since 1996. The Brazilian Institute of Geography and Statistics (IBGE) has provided estimation of population in Brazil and its macro-regions for the past four decades. So-cio-demographic statistics of the resident population were based on the 10-year interval census (1980, 1991, 2000 and 2010) and the annual inter-census projections performed by IBGE. Statistics of estimated Brazilian population are web available (www.ibge.gov.br) and can be stratified by age, gender and geographic localization.
Liver-related deaths were defined by the following ICD-10 codes: viral hepatitis [B15-B19]; hepatocellular or cholangiocarcinoma [C22.0, C22.1]; alcoholic liver disease [K70]; cirrhosis [I85, K73 and K74] and other liver diseases [K71, K72, K75, K76]. The presence of I85, K73 or K74 ICD-10 codes in any field of the DC defined cirrhosis. Deaths classified as R00-R99 [Symptoms, signs and abnormal clinical and laboratory findings, not classified elsewhere] were considered as ill-defined or of unknown cause of death as these codes do not give any information concerning the possible conditions that led to death.10 The number of deaths and the crude mortality rate due to ill-defined or unknown cause of death were used to estimate the quality of death registration.11 Macro-regions of Brazil were defined by IBGE as legally valid subnational units known as North, Northeast, Center-West, Southeast and South regions.
Brazilian mortality rates related to cirrhosis were analyzed from 2000 to 2012 (the latest year available at the time of the present analysis). Deaths due to cirrhosis were reported as absolute numbers and as crude mortality rates (expressed per 100,000 inhabitants). In addition, the crude mortality rates were adjusted for age using a standard population to define the age-standardized mortality rates (expressed per 100,000 inhabitants). Crude mortality rate was calculated as the ratio of the total number of deaths in a period to the estimated resident population in the same period. The age-standardized mortality rate was calculated using the direct standardization method which is the weighted average of the age-specific rates from the standard population.12,13 The World Standard population (2000-2025) reported by the World Health Organization (WHO) was used as the standard population to apply the direct standardization method in the study.14,15 Data management and mortality rate calculations (with 95% confidence interval) were performed using the software STATA (2012; StataCorp LP, College Station, TX, USA).
Annual trends in the mortality rates were assessed using Poisson regression models with deaths due to cirrhosis as the dependent variable, year as the continuous independent variable and log (population) as an offset to adjust for the population at risk by year. Models’ residuals were inspected graphically. These plots showed random dispersion of residuals as a function of time so the linear assumption was deemed valid. To explore the impact of ill-defined deaths on the observed trends, ill-defined deaths were proportionally redistributed according to the defined causes (i.e. cirrhosis and other causes) by age. After redistribution, trends were tested using the same methodology described above.
RESULTSA total of 13,672,446 deaths occurred in Brazil from 2000 to 2012. Cardiovascular disease, non-liver cancer and external causes were the top ranking causes of death. A total of 575,878 (4.2%) deaths had ICD-10 codes of liver diseases mentioned on their DC. Cirrhosis was the primary or the underlying cause for 265,180 deaths. Thus, cirrhosis was mentioned in any field of the DC in 46% of liver-related deaths and 2% of all deaths in this period. Deaths that have mention of liver diseases as well as those with mention of cirrhosis on their DC increased in absolute numbers from 2000 to 2012 (Table 1).
Absolute number of deaths from liver diseases and cirrhosis from 2000 to 2012 in Brazil.
| Year | Deaths (n) | |
|---|---|---|
| Liver-related | Cirrhosis-related | |
| 2000 | 36,404 | 18,245 |
| 2001 | 38,028 | 18,644 |
| 2002 | 38,760 | 18,816 |
| 2003 | 39,882 | 19,087 |
| 2004 | 41,983 | 19,833 |
| 2005 | 42,895 | 19,738 |
| 2006 | 43,878 | 20,215 |
| 2007 | 45,952 | 20,824 |
| 2008 | 47,772 | 21,514 |
| 2009 | 48,313 | 21,470 |
| 2010 | 50,111 | 21,973 |
| 2011 | 50,757 | 22,481 |
| 2012 | 51,143 | 22,340 |
| Total | 575,878 | 265,180 |
| % ▴ 2000 to 2012 | + 40.5 | + 22.4 |
The majority of individuals who had mention of cirrhosis on the DC were male (77%), aged > 40 years-old (90%) and self-declared ethnicity as Caucasian (54%). The median (IQR) age at time of death due to cirrhosis was 56 (47-67) years and most cases occurred in the Southeast region (52%), the most populated area corresponding to 42% of the Brazilian population. A total of 18% (n = 47,695) and 9% (n = 23,692) of cirrhosis-related deaths had mention of alcoholic liver disease [K70] and viral hepatitis [B15-B19] on their death certificates, respectively. Table 2 summarizes the demographic characteristics of individuals who have mention of cirrhosis in their DC in Brazil from 2000 to 2012.
Demographic characteristics of people who had mention of cirrhosis in their death certificate (ICD-10: I85/K73/K74) from 2000 to 2012 in Brazil.
| Cirrhosis-related deaths (n = 265,180) | |
|---|---|
| Gender; n (%) | |
| Male | 203,271 (76.65) |
| Female | 61,860 (23.33) |
| NA | 49 (0.02) |
| Age groups; n (%) | |
| < 20 years | 1,543 (0.58) |
| 20-29 years | 4,607 (1.74) |
| 30-39 years | 23,056 (8.69) |
| 40-49 years | 56,237 (21.21) |
| 50-59 years | 69,754 (26.30) |
| 60-69 years | 55,614 (20.97) |
| 70-79 years | 36,687 (13.83) |
| ≥ 80 years | 16,523 (6.23) |
| NA | 1,159 (0.44) |
| Ethnicity; n (%) | |
| Caucasian | 142,154 (53.61) |
| miscegination ("pardo") | 80,125 (30.22) |
| African-Black | 19,495 (7.35) |
| Asiatic | 1,398 (0.53) |
| Indigenous | 500 (0.19) |
| NA | 21,508 (8.11) |
| Education in years of study; n (%) | |
| < 1 year | 27,541 (10.39) |
| 1 to 3 years | 53,604 (20.21) |
| 4 to 7 years | 49,931 (18.83) |
| 8 to 11 years | 24,378 (9.19) |
| ≥ 12 years | 11,688 (4.41) |
| NA | 98,371 (36.97) |
| Geographic macro-regions; n (%) | |
| North | 12,678 (4.78) |
| Northeast | 57,265 (21.59) |
| Southeast | 138,259 (52.14) |
| South | 41,754 (15.75) |
| Center-West | 15,224 (5.74) |
In 2012 the age-standardized cirrhosis mortality rate (95% confidence interval) was 11.71 (11.59-11.83) deaths per 100,000 inhabitants in Brazil. The Southeast region [12.52 (12.34-12.70)] had the highest and the South region [10.89 (10.59-11.19)] the lowest age-standardized cirrhosis mortality rate in this year. From 2000 to 2012 the age-standardized cirrhosis mortality rate decreased by 12% [from 13.32 (13.16-13.48) to 11.71 (11.59-11.83)] among individuals living in Brazil; the decreasing trend was statistically significant (p < 0.001). However, this trend was not uniform across the country. Age-standardized cirrhosis mortality rates decreased by 25% and 21% from 2000 to 2012 in the South [14.46 (14.07-14.87) to 10.89 (10.59-11.19)] and Southeast [15.85 (15.6-16.09) to 12.52 (12.34-12.70)] regions, respectively; again, for both regions, the decreasing trend was statistically significant (p < 0.001). In contrast, mortality rates remained relatively stable (a reduction of 3.6%) in the Center-West region [11.72 (11.10-12.34) to 11.30 (10.83-11.77)] with a non-significant trend (p = 0.41). Additionally, mortality rates increased by 30% and 16% in the North [8.84 (8.24-9.43) to 11.53 (11.08-11.99)] and Northeast [9.41 (9.13-9.69) to 10.93 (10.68-11.17)] regions, respectively, (Table 3) with both regions showing statistically significant increasing trends (p < 0.001). The trends described above were also observed after ill-defined deaths were redistributed with the only change observed in the Center-West region for which a borderline significant increasing trend (p = 0.06) was obtained (Table 4). Figure 1 plots the evolution of the age-standardized cirrhosis mortality rates in Brazil and its macro-regions throughout the 13 years of analysis.
Age-standardized cirrhosis mortality rate [95% confidence interval] according to macro-regions in Brazil from 2000 to 2012.
| North | Northeast | Southeast | South | Center-West | Brazil | |
|---|---|---|---|---|---|---|
| 2000 | 8.84 | 9.41 | 15.85 | 14.46 | 11.72 | 13.32 |
| [8.24-9.43] | [9.13-9.69] | [15.6-16.09] | [14.07-14.87] | [11.10-12.34] | [13.16-13.48] | |
| 2001 | 11.19 | 10.30 | 15.40 | 13.50 | 11.56 | 13.30 |
| [10.56-11.82] | [10.02-10.59] | [15.17-15.63] | [13.12-13.89] | [10.95-12.16] | [13.15-13.45] | |
| 2002 | 10.68 | 10.52 | 14.77 | 13.86 | 11.07 | 13.07 |
| [10.08-11.27] | [10.24-10.81] | [14.54-15.0] | [13.48-14.24] | [10.49-11.66] | [12.92-13.22] | |
| 2003 | 9.68 | 10.04 | 15.17 | 13.27 | 10.33 | 12.94 |
| [9.12-10.25] | [9.77-10.31] | [14.95-15.40] | [12.90-13.64] | [9.77-10.89] | [12.79-13.09] | |
| 2004 | 11.09 | 10.37 | 15.00 | 13.14 | 10.79 | 13.03 |
| [10.51-11.67] | [10.10-10.64] | [14.78-15.22] | [12.79-13.51] | [10.23-11.34] | [12.88-13.17] | |
| 2005 | 10.90 | 10.52 | 14.42 | 12.46 | 10.64 | 12.68 |
| [10.33-11.45] | [10.25-10.79] | [14.21-14.64] | [12.12-12.81] | [10.09-11.18] | [12.53-12.82] | |
| 2006 | 11.03 | 10.80 | 14.09 | 12.38 | 11.13 | 12.62 |
| [10.48-11.58] | [10.54-11.07] | [13.88-14.30] | [12.04-12.73] | [10.60-11.66] | [12.48-12.76] | |
| 2007 | 10.80 | 11.10 | 14.06 | 12.04 | 10.92 | 12.60 |
| [10.27-11.33] | [10.84-11.37] | [13.86-14.27] | [11.70-12.38] | [10.40-11.44] | [12.47-12.74] | |
| 2008 | 11.37 | 11.45 | 13.68 | 12.36 | 11.93 | 12.66 |
| [10.85-11.89] | [11.18-11.71] | [13.48-13.88] | [12.03-12.70] | [11.41-12.45] | [12.52-12.79] | |
| 2009 | 10.57 | 11.20 | 13.53 | 11.35 | 11.41 | 12.29 |
| [10.06-11.08] | [10.95-11.46] | [13.34-13.73] | [11.04-11.68] | [10.91-11.92] | [12.16-12.43] | |
| 2010 | 11.26 | 10.98 | 13.30 | 11.73 | 10.89 | 12.20 |
| [10.76-11.77] | [10.73-11.24] | [13.11-13.50] | [11.41-12.05] | [10.40-11.39] | [12.07-12.33] | |
| 2011 | 11.50 | 11.09 | 13.11 | 11.38 | 11.58 | 12.13 |
| [11.03-11.98] | [10.85-11.35] | [12.93-13.30] | [11.07-11.69] | [11.09-12.06] | [12.01-12.26] | |
| 2012 | 11.53 | 10.93 | 12.52 | 10.89 | 11.30 | 11.71 |
| [11.08-11.99] | [10.68-11.17] | [12.34-12.70] | [10.59-11.19] | [10.83-11.77] | [11.59-11.83] | |
| % ▴ 2000 to 2012 | +30.4% | +16.2% | -21.0% | -24.7% | +3.6% | -12.1% |
| p value | < 0.001 | < 0.001 | < 0.001 | < 0.001 | 0.41 | < 0.001 |
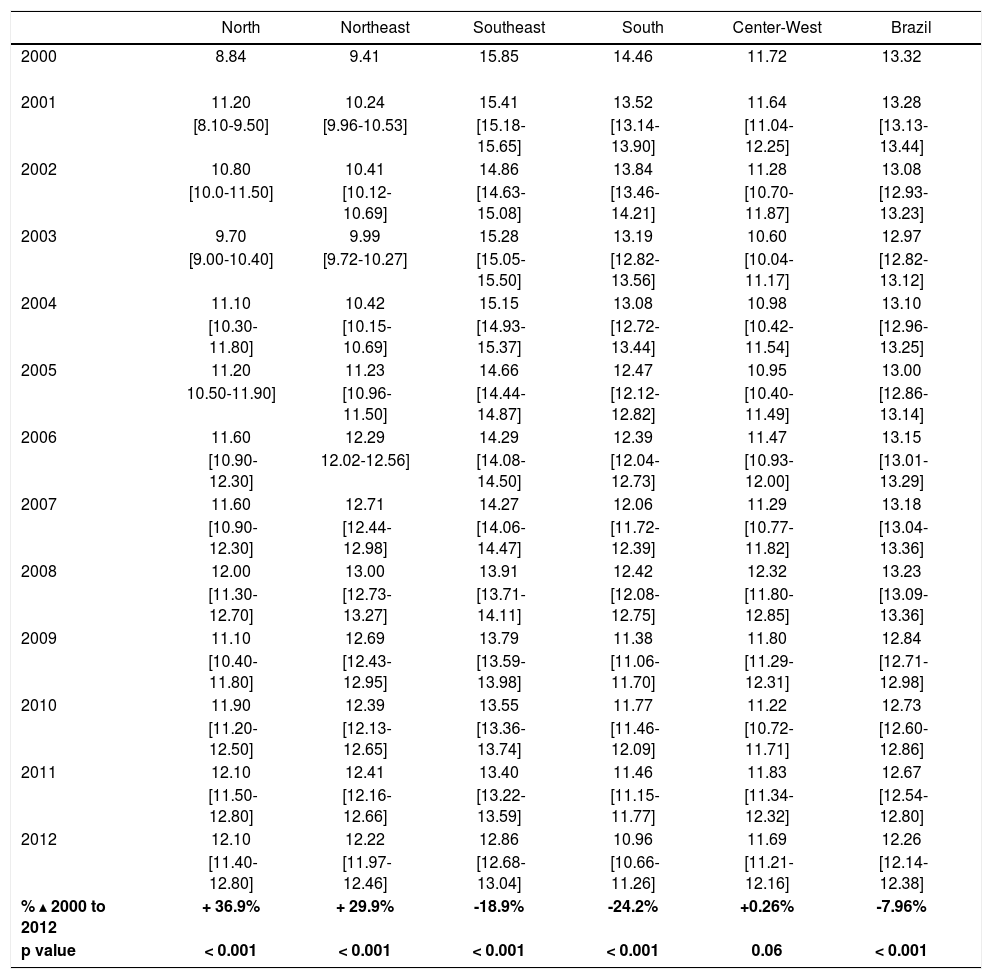
Age-standardized cirrhosis mortality rate [95% confidence interval] in Brazil and its macro-regions from 2000 to 2012 after proportional distribution of ill-defined deaths according to the defined causes (i.e. cirrhosis and other causes).
| North | Northeast | Southeast | South | Center-West | Brazil | |
|---|---|---|---|---|---|---|
| 2000 | 8.84 | 9.41 | 15.85 | 14.46 | 11.72 | 13.32 |
| 2001 | 11.20 | 10.24 | 15.41 | 13.52 | 11.64 | 13.28 |
| [8.10-9.50] | [9.96-10.53] | [15.18-15.65] | [13.14-13.90] | [11.04-12.25] | [13.13-13.44] | |
| 2002 | 10.80 | 10.41 | 14.86 | 13.84 | 11.28 | 13.08 |
| [10.0-11.50] | [10.12-10.69] | [14.63-15.08] | [13.46-14.21] | [10.70-11.87] | [12.93-13.23] | |
| 2003 | 9.70 | 9.99 | 15.28 | 13.19 | 10.60 | 12.97 |
| [9.00-10.40] | [9.72-10.27] | [15.05-15.50] | [12.82-13.56] | [10.04-11.17] | [12.82-13.12] | |
| 2004 | 11.10 | 10.42 | 15.15 | 13.08 | 10.98 | 13.10 |
| [10.30-11.80] | [10.15-10.69] | [14.93-15.37] | [12.72-13.44] | [10.42-11.54] | [12.96-13.25] | |
| 2005 | 11.20 | 11.23 | 14.66 | 12.47 | 10.95 | 13.00 |
| 10.50-11.90] | [10.96-11.50] | [14.44-14.87] | [12.12-12.82] | [10.40-11.49] | [12.86-13.14] | |
| 2006 | 11.60 | 12.29 | 14.29 | 12.39 | 11.47 | 13.15 |
| [10.90-12.30] | 12.02-12.56] | [14.08-14.50] | [12.04-12.73] | [10.93-12.00] | [13.01-13.29] | |
| 2007 | 11.60 | 12.71 | 14.27 | 12.06 | 11.29 | 13.18 |
| [10.90-12.30] | [12.44-12.98] | [14.06-14.47] | [11.72-12.39] | [10.77-11.82] | [13.04-13.36] | |
| 2008 | 12.00 | 13.00 | 13.91 | 12.42 | 12.32 | 13.23 |
| [11.30-12.70] | [12.73-13.27] | [13.71-14.11] | [12.08-12.75] | [11.80-12.85] | [13.09-13.36] | |
| 2009 | 11.10 | 12.69 | 13.79 | 11.38 | 11.80 | 12.84 |
| [10.40-11.80] | [12.43-12.95] | [13.59-13.98] | [11.06-11.70] | [11.29-12.31] | [12.71-12.98] | |
| 2010 | 11.90 | 12.39 | 13.55 | 11.77 | 11.22 | 12.73 |
| [11.20-12.50] | [12.13-12.65] | [13.36-13.74] | [11.46-12.09] | [10.72-11.71] | [12.60-12.86] | |
| 2011 | 12.10 | 12.41 | 13.40 | 11.46 | 11.83 | 12.67 |
| [11.50-12.80] | [12.16-12.66] | [13.22-13.59] | [11.15-11.77] | [11.34-12.32] | [12.54-12.80] | |
| 2012 | 12.10 | 12.22 | 12.86 | 10.96 | 11.69 | 12.26 |
| [11.40-12.80] | [11.97-12.46] | [12.68-13.04] | [10.66-11.26] | [11.21-12.16] | [12.14-12.38] | |
| % ▴ 2000 to 2012 | + 36.9% | + 29.9% | -18.9% | -24.2% | +0.26% | -7.96% |
| p value | < 0.001 | < 0.001 | < 0.001 | < 0.001 | 0.06 | < 0.001 |
 from 2000 to 2012 in Brazil and its macro-regions. Brazil: statistically significant decreasing trend (p < 0.001). North: statistically significant increasing trend (p < 0.001). Northeast: statistically significant increasing trend (p < 0.001). Southeast: statistically significant decreasing trend (p < 0.001), South: statistically significant decreasing trend (p < 0.001). Center-West: non-significant trend (p = 0.41).")
Age-standardized mortality rates associated with cirrhosis (deaths per 100,000 inhabitants) from 2000 to 2012 in Brazil and its macro-regions. Brazil: statistically significant decreasing trend (p < 0.001). North: statistically significant increasing trend (p < 0.001). Northeast: statistically significant increasing trend (p < 0.001). Southeast: statistically significant decreasing trend (p < 0.001), South: statistically significant decreasing trend (p < 0.001). Center-West: non-significant trend (p = 0.41).
The age-standardized cirrhosis mortality rate (per 100,000 inhabitants) decreased in both genders from 2000 to 2012 [in men from 21.63 to 18.95 and in women from 5.75 to 5.32]. Males presented 4-fold higher age-standardized cirrhosis mortality rate compared to females (Table 5). In stratification by age groups, the crude cirrhosis mortality rate starts to become expressive (> 10 deaths per 100,000 inhabitants) in persons older than 40 years of age. In 2012 the crude cirrhosis mortality rate remained very high in individuals aged 50-59 years in all of Brazil’s macro-regions [North = 25.16; Northeast = 26.57; Southeast = 33.96; South = 30.69 and Center-West = 28.83 deaths per 100,000 inhabitants] (Table 6).
Description of crude and age-standardized cirrhosis mortality rate by gender from 2000 to 2012 according to macro-regions in Brazil.
| Mortality Rate | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| North crude | M | 7.26 | 9.64 | 9.22 | 8.07 | 9.46 | 9.46 | 9.74 | 9.52 | 10.10 | 9.74 | 10.57 | 10.39 | 10.82 |
| F | 2.72 | 2.97 | 2.70 | 2.72 | 3.09 | 3.04 | 2.98 | 3.26 | 3.58 | 3.11 | 3.48 | 4.00 | 3.61 | |
| age-standarized | M | 12.61 | 16.85 | 16.25 | 14.21 | 16.37 | 16.36 | 16.65 | 16.15 | 16.59 | 16.08 | 16.72 | 16.55 | 17.23 |
| F | 4.81 | 5.24 | 4.87 | 4.99 | 5.62 | 5.29 | 5.25 | 5.38 | 6.08 | 5.03 | 5.72 | 6.44 | 5.84 | |
| Northeast crude | M | 10.33 | 11.54 | 12.06 | 11.29 | 12.00 | 12.45 | 12.90 | 13.45 | 14.00 | 14.20 | 13.88 | 14.57 | 14.50 |
| F | 3.34 | 3.55 | 3.60 | 3.72 | 3.72 | 3.64 | 3.93 | 4.15 | 4.46 | 4.12 | 4.44 | 4.31 | 4.46 | |
| age-standarized | M | 15.03 | 16.62 | 17.07 | 15.98 | 16.77 | 17.37 | 17.67 | 18.14 | 18.52 | 18.60 | 17.78 | 18.34 | 17.97 |
| F | 4.37 | 4.63 | 4.65 | 4.74 | 4.69 | 4.52 | 4.78 | 4.96 | 5.25 | 4.77 | 5.04 | 4.79 | 4.86 | |
| Southeast crude | M | 21.36 | 21.09 | 20.48 | 21.26 | 21.50 | 20.76 | 20.31 | 20.88 | 20.38 | 20.50 | 20.62 | 20.55 | 20.15 |
| F | 5.95 | 5.72 | 5.61 | 5.96 | 5.93 | 6.04 | 6.23 | 6.18 | 6.42 | 6.54 | 6.49 | 6.72 | 6.42 | |
| age-standarized | M | 26.10 | 25.65 | 24.61 | 25.09 | 24.91 | 23.67 | 22.93 | 23.12 | 22.19 | 21.91 | 21.64 | 21.10 | 20.35 |
| F | 6.71 | 6.36 | 6.15 | 6.44 | 6.25 | 6.27 | 6.34 | 6.13 | 6.25 | 6.21 | 6.03 | 6.10 | 5.67 | |
| South crude | M | 19.52 | 17.99 | 19.32 | 18.69 | 18.98 | 18.02 | 18.14 | 18.24 | 18.97 | 17.73 | 18.71 | 18.49 | 17.86 |
| F | 5.16 | 5.39 | 5.11 | 5.13 | 5.03 | 5.13 | 5.37 | 5.17 | 5.53 | 5.26 | 5.59 | 5.55 | 5.67 | |
| age-standarized | M | 23.97 | 21.82 | 23.04 | 21.90 | 21.94 | 20.48 | 20.11 | 19.81 | 20.21 | 18.52 | 19.04 | 18.51 | 17.50 |
| F | 5.90 | 6.05 | 5.63 | 5.56 | 5.33 | 5.33 | 5.46 | 5.13 | 5.36 | 4.97 | 5.15 | 5.01 | 4.98 | |
| Center-West crude | M | 13.22 | 12.97 | 12.30 | 11.72 | 12.44 | 12.49 | 13.49 | 13.20 | 14.84 | 14.88 | 14.26 | 15.80 | 15.36 |
| F | 3.08 | 3.33 | 3.64 | 3.34 | 3.62 | 3.50 | 3.71 | 3.85 | 4.31 | 3.84 | 4.19 | 4.03 | 4.41 | |
| age-standarized | M | 18.85 | 18.47 | 16.95 | 16.08 | 16.77 | 16.72 | 17.72 | 17.12 | 18.74 | 18.40 | 17.18 | 18.92 | 18.00 |
| F | 4.59 | 4.74 | 5.28 | 4.70 | 4.99 | 4.76 | 4.83 | 4.99 | 5.44 | 4.78 | 4.94 | 4.68 | 5.02 | |
| Brazil crude | M | 16.31 | 16.48 | 16.47 | 16.35 | 16.85 | 16.52 | 16.56 | 16.92 | 17.13 | 17.02 | 17.15 | 17.37 | 17.09 |
| F | 4.66 | 4.69 | 4.62 | 4.78 | 4.80 | 4.83 | 5.03 | 5.07 | 5.37 | 4.25 | 5.38 | 5.46 | 5.39 | |
| age-standarized | M | 21.63 | 21.69 | 21.40 | 21.01 | 21.32 | 20.67 | 20.44 | 20.53 | 20.39 | 19.96 | 19.68 | 19.58 | 18.95 |
| F | 5.75 | 5.72 | 5.56 | 5.68 | 5.60 | 5.54 | 5.66 | 5.58 | 5.79 | 4.47 | 5.56 | 5.51 | 5.32 |
Mortality rate due to cirrhosis in age groups according to macro-regions from 2000 to 2012 in Brazil.
| Age (years) | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| North | < 20 | 0.41 | 0.50 | 0.31 | 0.24 | 0.30 | 0.28 | 0.23 | 0.41 | 0.29 | 0.22 | 0.17 | 0.14 | 0.20 |
| 20-29 | 1.77 | 1.95 | 1.46 | 1.23 | 1.19 | 1.34 | 1.00 | 1.11 | 1.33 | 1.38 | 1.33 | 1.25 | 0.57 | |
| 30-39 | 5.11 | 5.12 | 5.18 | 4.55 | 4.56 | 4.47 | 4.52 | 4.61 | 4.11 | 3.68 | 3.68 | 3.16 | 2.70 | |
| 40-49 | 10.82 | 15.03 | 14.36 | 11.84 | 13.80 | 13.38 | 12.99 | 12.43 | 15.12 | 11.34 | 13.06 | 12.77 | 11.21 | |
| 50-59 | 21.76 | 26.73 | 23.91 | 21.50 | 27.29 | 25.64 | 25.29 | 23.24 | 23.36 | 23.93 | 27.64 | 25.69 | 25.16 | |
| 60-69 | 28.02 | 40.92 | 31.99 | 29.82 | 38.28 | 36.56 | 40.51 | 36.97 | 37.50 | 40.33 | 40.83 | 40.61 | 43.82 | |
| 70-79 | 39.68 | 49.55 | 59.18 | 56.35 | 50.97 | 54.24 | 56.75 | 63.64 | 62.00 | 55.68 | 52.17 | 66.25 | 70.46 | |
| ≤ 80 | 50.16 | 52.91 | 67.29 | 65.10 | 79.00 | 80.28 | 75.42 | 70.39 | 91.94 | 75.22 | 90.55 | 94.47 | 98.62 | |
| Northeast | < 20 | 0.18 | 0.16 | 0.13 | 0.18 | 0.16 | 0.16 | 0.18 | 0.16 | 0.14 | 0.12 | 0.10 | 0.14 | 0.12 |
| 20-29 | 1.14 | 1.21 | 1.44 | 1.02 | 1.00 | 1.01 | 1.04 | 1.21 | 1.10 | 0.93 | 1.02 | 1.03 | 0.93 | |
| 30-39 | 6.11 | 6.57 | 7.52 | 5.98 | 6.06 | 5.55 | 5.81 | 6.12 | 6.52 | 5.87 | 5.34 | 5.42 | 5.28 | |
| 40-49 | 15.97 | 17.41 | 17.16 | 15.76 | 16.63 | 15.00 | 15.87 | 16.28 | 16.86 | 15.88 | 16.20 | 15.91 | 15.71 | |
| 50-59 | 23.87 | 26.97 | 26.58 | 25.36 | 25.86 | 26.57 | 27.67 | 27.65 | 28.69 | 26.22 | 27.70 | 28.27 | 26.57 | |
| 60-69 | 28.76 | 31.50 | 33.14 | 33.17 | 34.08 | 34.69 | 34.59 | 34.81 | 36.76 | 40.56 | 36.61 | 37.08 | 37.77 | |
| 70-79 | 35.99 | 38.98 | 39.79 | 39.24 | 41.09 | 47.86 | 46.27 | 49.99 | 50.42 | 50.28 | 47.43 | 48.16 | 48.32 | |
| ≥ 80 | 40.83 | 42.94 | 41.88 | 48.91 | 51.58 | 56.11 | 61.20 | 63.32 | 62.38 | 63.26 | 65.35 | 65.86 | 66.66 | |
| Southeast | < 20 | 0.23 | 0.21 | 0.19 | 0.23 | 0.21 | 0.14 | 0.15 | 0.13 | 0.15 | 0.16 | 0.13 | 0.13 | 0.11 |
| 20-29 | 1.80 | 1.55 | 1.30 | 1.30 | 1.34 | 1.10 | 0.90 | 0.84 | 1.00 | 0.82 | 0.73 | 0.65 | 0.70 | |
| 30-39 | 10.24 | 9.42 | 8.65 | 8.63 | 8.44 | 7.57 | 7.25 | 6.30 | 5.97 | 5.44 | 5.26 | 5.01 | 4.43 | |
| 40-49 | 28.05 | 25.72 | 24.41 | 24.25 | 24.37 | 23.09 | 20.51 | 21.33 | 19.91 | 19.24 | 18.14 | 17.70 | 16.17 | |
| 50-59 | 41.63 | 41.46 | 39.15 | 40.62 | 40.11 | 39.33 | 38.11 | 39.17 | 37.41 | 38.32 | 37.28 | 36.07 | 33.96 | |
| 60-69 | 50.60 | 50.35 | 48.56 | 52.55 | 51.41 | 50.17 | 51.51 | 50.20 | 49.04 | 49.44 | 50.64 | 51.64 | 48.81 | |
| 70-79 | 56.72 | 55.21 | 57.53 | 59.08 | 57.59 | 56.27 | 57.76 | 57.98 | 59.74 | 58.65 | 57.53 | 55.94 | 58.03 | |
| ≥ 80 | 52.55 | 59.74 | 56.85 | 52.94 | 54.40 | 53.61 | 56.84 | 56.96 | 56.72 | 54.40 | 56.21 | 57.85 | 57.93 | |
| South | < 20 | 0.25 | 0.28 | 0.11 | 0.17 | 0.14 | 0.09 | 0.17 | 0.19 | 0.18 | 0.12 | 0.14 | 0.19 | 0.09 |
| 20-29 | 1.33 | 1.15 | 1.15 | 0.78 | 0.92 | 0.75 | 0.70 | 0.84 | 0.67 | 0.69 | 0.71 | 0.73 | 0.60 | |
| 30-39 | 8.04 | 7.60 | 7.67 | 6.81 | 6.67 | 6.17 | 5.10 | 5.54 | 5.87 | 4.33 | 3.89 | 3.93 | 3.85 | |
| 40-49 | 22.07 | 20.05 | 20.30 | 20.07 | 18.58 | 16.75 | 17.30 | 16.96 | 17.37 | 15.15 | 16.76 | 14.80 | 14.91 | |
| 50-59 | 40.75 | 35.84 | 38.23 | 35.42 | 34.89 | 33.45 | 33.98 | 33.86 | 33.44 | 32.66 | 33.72 | 31.71 | 30.69 | |
| 60-69 | 48.19 | 48.34 | 49.28 | 49.21 | 50.70 | 47.24 | 48.65 | 43.80 | 46.53 | 42.80 | 43.48 | 44.50 | 41.23 | |
| 70-79 | 57.55 | 52.51 | 54.56 | 51.98 | 54.89 | 54.22 | 52.40 | 49.64 | 50.91 | 47.30 | 50.80 | 51.22 | 48.97 | |
| ≥ 80 | 51.56 | 54.11 | 54.22 | 53.30 | 47.82 | 52.20 | 45.99 | 48.94 | 53.24 | 51.98 | 48.24 | 47.52 | 45.09 | |
| Center-West | < 20 | 0.21 | 0.35 | 0.10 | 0.22 | 0.12 | 0.12 | 0.24 | 0.12 | 0.16 | 0.22 | 0.14 | 0.08 | 0.16 |
| 20-29 | 1.62 | 1.24 | 1.13 | 0.74 | 0.84 | 0.91 | 0.86 | 0.88 | 0.95 | 0.83 | 0.60 | 0.63 | 0.82 | |
| 30-39 | 6.78 | 6.51 | 6.68 | 5.60 | 5.97 | 5.65 | 5.99 | 5.36 | 5.86 | 5.55 | 5.94 | 5.30 | 4.37 | |
| 40-49 | 19.85 | 18.37 | 17.42 | 16.66 | 17.64 | 15.58 | 17.04 | 15.32 | 17.33 | 16.72 | 17.34 | 17.48 | 17.39 | |
| 50-59 | 26.95 | 27.42 | 28.09 | 24.30 | 26.29 | 26.94 | 28.56 | 27.99 | 31.36 | 29.31 | 27.47 | 28.73 | 28.83 | |
| 60-69 | 37.71 | 38.78 | 36.51 | 38.44 | 36.41 | 34.98 | 33.04 | 35.97 | 39.33 | 37.86 | 38.22 | 43.44 | 38.64 | |
| 70-79 | 49.21 | 49.25 | 51.34 | 42.58 | 45.28 | 49.03 | 51.55 | 55.63 | 55.36 | 52.66 | 44.74 | 52.30 | 51.83 | |
| ≥ 80 | 55.15 | 52.67 | 33.99 | 41.41 | 50.07 | 52.77 | 59.65 | 49.34 | 56.83 | 56.91 | 47.75 | 49.44 | 58.90 |
A total of 1,327,364 deaths were classified as ill-defined causes of death from 2000 to 2012 in Brazil. The crude mortality rate of ill-defined or unknown causes of death remained very high in 2012 in Brazil: 38.63 deaths per 100,000 inhabitants, with the North region having the highest (46.42) and Center-West the lowest (16.92) rates. However, absolute number of deaths and the mortality rate by ill-defined causes decreased from 135,749 to 74,935 (-45%) and from 79.95 to 38.63 (-52%) per 100,000 inhabitants from 2000 to 2012 in Brazil, respectively. In addition, the absolute number of deaths and crude mortality rate of ill-defined or unknown causes of death also reduced in all of Brazil’s macro-regions in the same period. The higher percentage of reduction in these parameters was observed in the North and Northeast regions reflecting a possible improvement in data quality in the last decade (Table 7).
Evolution of number of deaths and mortality rates of ill-defined or unknown causes of deaths [Symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified (R00-R99)] from 2000 to 2012 according to the macro-regions in Brazil.
| North | Northeast | Southeast | South | Center-West | Brazil | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Deaths | Mortality rate | Deaths | Mortality rate | Deaths | Mortality rate | Deaths | Mortality rate | Deaths | Mortality rate | Deaths | Mortality rate | % | |
| 2000 | 11,396 | 88.34 | 64,850 | 135.84 | 45,276 | 62.53 | 9,622 | 38.32 | 4,605 | 39.57 | 135,749 | 79.95 | 14.34 |
| 2001 | 11,489 | 86.74 | 65,546 | 135.62 | 44,867 | 61.07 | 9,492 | 37.29 | 4,372 | 36.78 | 135,766 | 78.76 | 14.12 |
| 2002 | 10,873 | 80.51 | 66,653 | 136.46 | 43,019 | 57.78 | 9,790 | 38.04 | 3,841 | 31.74 | 134,176 | 76.83 | 13.65 |
| 2003 | 11,190 | 81.18 | 65,488 | 132.68 | 42,889 | 56.89 | 10,508 | 40.38 | 3,359 | 27.27 | 133,434 | 75.44 | 13.31 |
| 2004 | 11,270 | 80.13 | 60,702 | 121.74 | 41,250 | 54.04 | 10,072 | 38.27 | 3,628 | 28.95 | 126,922 | 70.86 | 12.39 |
| 2005 | 9,715 | 66.09 | 43,743 | 85.74 | 38,552 | 49.13 | 9,246 | 34.28 | 3,199 | 24.57 | 104,455 | 56.71 | 10.37 |
| 2006 | 8,391 | 55.86 | 24,275 | 47.04 | 40,372 | 50.74 | 9,424 | 34.51 | 3,081 | 23.22 | 85,543 | 45.80 | 8.29 |
| 2007 | 7,250 | 47.25 | 21,147 | 40.52 | 39,747 | 49.29 | 9,347 | 33.82 | 2,753 | 20.37 | 80,244 | 42.38 | 7.66 |
| 2008 | 7,755 | 51.21 | 21,586 | 40.66 | 38,372 | 47.85 | 8,700 | 31.64 | 2,748 | 20.06 | 79,161 | 41.75 | 7.35 |
| 2009 | 7,920 | 51.56 | 21,696 | 40.48 | 37,680 | 46.57 | 9,050 | 32.65 | 2,648 | 19.06 | 78,994 | 41.25 | 7.16 |
| 2010 | 7,732 | 48.74 | 22,196 | 41.81 | 38,047 | 47.34 | 8,743 | 31.92 | 2,904 | 20.66 | 79,622 | 41.74 | 7.00 |
| 2011 | 7,473 | 46.43 | 23,256 | 43.47 | 35,962 | 44.41 | 8,389 | 30.44 | 3,283 | 23.05 | 78,363 | 40.73 | 6.69 |
| 2012 | 7,589 | 46.42 | 22,723 | 42.15 | 33,803 | 41.44 | 8,379 | 30.21 | 2,441 | 16.92 | 74,935 | 38.63 | 6.34 |
| % ▴ from 2000 to 2012 | -33% | -48% | -65% | -69% | -25% | -34% | -12% | -21% | -47% | -57% | -45% | -52% | -56% |
The present study highlights the burden of mortality due to cirrhosis in Brazil from 2000 to 2012. The analysis of a nationwide death registry database showed a decrease in age-standardized mortality rate associated with cirrhosis from 2000 to 2012 in Brazil. Despite this favorable evolution, cirrhosis still causes approximately 20,000 deaths per year and remains a major public health issue in Brazil.
Cirrhosis remains the most frequent liver-related cause of death worldwide.7 Cirrhosis mortality rates seem to be higher in individuals with lower levels of education and in areas with lower socioeconomic status.16 Globally, mortality rates associated with cirrhosis decreased from 20.0 (95%CI 13.5-29.4) to 15.8 (10.2-23.6) deaths per 100,000 persons per year from 1980 to 2010, probably driven by a 60% mortality reduction in East Asian countries. Despite the decrease in mortality rates, absolute number of deaths due to cirrhosis had a significant increase in the same peri-od.17 The Global Burden of Disease study, an overview of national trends in cause-specific mortality in 187 countries, reported a 16% worldwide decrease in age-standardized cirrhosis mortality rates from 1990 to 2010 (from 18.6 (95%CI 15.8-20.7) to 15.6 (13.2-17.6) deaths per 100,000 in-habitants).17
In Europe, cirrhosis mortality has been following a strong “East-to-West” gradient.18 An expressive decline in cirrhosis mortality was observed in Mediterranean countries such as France, Italy, Spain and Portugal.5 Despite the decrease in mortality rates, cirrhosis continues to be related to 170,000 deaths in 2013 leading the European health authorities to launch programs that aim to significantly reduce liver mortality and decrease the burden of liver diseases with evidence-based policy measures. In Portugal, hospitalization due to alcoholic cirrhosis increased by up to 30% in males and 45% in individuals aged between 40 and 54 years from 1993 to 2008.19
In Latin American countries, the trend of cirrhosis mortality varies widely: mortality rates increased in Paraguay and decreased in Chile and Argentine.17 In addition, mortality rates have been increasing in recent years in Mexico, one of the countries with the highest mortality rates due to liver diseases worldwide.20 In a Brazilian study, Nader, et al. reported more than 800,000 hospitali-zations due to liver disease from 2001 to 2010, most due to cirrhosis (~30,000 admissions per year).21
In the present study, we reported similar trends for age-standardized cirrhosis mortality rates in Brazil compared to those globally described in recent years. In our analysis, age-standardized cirrhosis mortality rates (deaths per 100,000 inhabitants) has been statistically significant decreasing from 2000 to 2012 (p < 0.001). This worldwide decrease in cirrhosis mortality rates is probably associated with screening transfused blood for viral hepatitis, implementation of hepatitis B vaccination programs, access to hepatitis C treatments and effective health policies to prevent alcoholic liver disease.22 In our study, the proportional mortality rate from cirrhosis decreased from 50.1% to 43.7% from 2000 to 2012 (Table 1). We hypothesize this was likely driven by a better quality of data registration and an 2-fold increase in proportional mortality rates from liver cancer (from 2.97% to 5.55%) in this period.
Brazilian age-standardized cirrhosis mortality rates (per 100,000 inhabitants) in 2010 were similar to France (11.2) and Germany (12.4) in Western-Europe; Paraguay (12.5) and Argentina (14.0) in Latin America. We have higher mortality rates than Scandinavian countries (Sweden with 5.4 and Norway with 4.2 deaths per 100,000 inhabitants) and lower rates than Mexico (38.3), Chile (21.8), North African countries, such as Egypt (72.7), Sub-Saharan Africa and most countries in Asia.5,17 Sub-Saharan Africa has high rates of liver disease burden and low funds of global health spending.23 However, comparison of mortality rates due to cirrhosis among countries has been challenged by different death report processes and methodologies used in data analysis across the studies. There is no consensus on which ICD-10 codes should be included to consider death by cirrhosis. Mendez-Sanchez, et al. defined cirrhosis by a strict list of ICD-10 codes (K74.0-K74.6).20 On the other hand, Mokdad, et al. opted for a broader definition of cirrhosis including ICD codes from chronic hepatitis, alcoholic liver disease and hepatic failure.17 Studies using data from death certificates have estimated around 30,000 deaths per year due to cirrhosis in the United States.3 However, if codes for viral hepatitis and alcoholic liver disease had been included in these estimates this number would increase to 60,000 deaths per year.4 In addition, the crude or unadjusted mortality rate should not be used to compare trends of mortality among different countries. The different age distribution of populations can lead to a misunderstanding in comparisons and interpretation of data. If a country has a higher proportion of an ageing population, people will have an inherently greater risk of dying compared to a country with a younger population.24 Thus, comparisons of mortality rates between regions or countries should be interpreted with caution due to the considerable variability in death report processes worldwide and methodologies used in data analysis. In the present study, death due to cirrhosis was defined by the presence of I85 or K73 or K74 in the primary, secondary or contributing causes of death on the DC; mortality rates were age-adjusted using the direct method and the standard population proposed by WHO which has an average world population age-structure constructed for the period 2000-2025.
We acknowledge that our findings are subject to several limitations, mainly associated with the lack of high quality cause of death registration in some Brazilian regions. The proportion of deaths from ill-defined or unknown conditions has been commonly used as an indicator of the quality of cause-of-death data.25 However, a low absolute number or mortality rate of this condition does not necessarily mean a high quality in cause-of-death information, as it does not exclude other forms of misclassification.26 Death count coverage in Brazil has increased from 80% in 1980-1991 to more than 95% in 2000-2010.27 Improvement in data quality seems to be closely associated with investments in the public health care system and death reporting processes.28 Beyond the satisfactory national death count coverage in the last 10 years, there are still large regional differences in mortality reports in Brazil: data quality seems to be better in the South and Southeast compared to other regions.29 Taken together, these observations suggest that the decreasing mortality rate observed for the country likely accurately reflects the changing patterns of mortality due to cirrhosis. The analysis within the major regions, on the other hand, should be interpreted with a grain of salt. The better data quality in the South and Southeast regions suggests the observed decreasing trends might be real while the important increase in cirrhosis-related mortality rates in the North and Northeast might be true or an artifact due to a better quality of data registration in these regions in the more recent years. In a sensitive analysis, we reported similar trends on cirrhosis-related mortality in Brazil and its regions when ill-defined deaths were proportionally redistributed according to the defined causes (i.e. cirrhosis and other causes) by age (Table 4).
The proportion of ill-defined causes of death is variable across European countries with very low rates (< 1%) in Finland, United Kingdom, Austria and Italy.10 In our study, ill-defined or unknown causes of death represented 9.7% of all deaths in the analyzed period. However, this proportion decreased from 14.3% to 6.3% (a reduction of 56%) from 2000 to 2012 in Brazil (Table 6). A study of França, et al., reported that 20% of ill-defined or unknown causes of death [R00-R99] in Brazil in 2010 were reclassified after investigation. The top ranking death causes reclassified were endocrine diseases, mental disorders, nervous system and cardiovascular diseases and maternal causes.30 Thus, liver diseases do not seem to be highly implicated in the reclassification of unknown causes of death. Since 2005, the Brazilian Ministry of Health has initiated a project to upgrade the mortality information, reducing the proportion of ill-defined deaths.31 We confirmed that the absolute number of deaths and mortality rates from ill-defined causes of death (R00-R99) decreased by 50% in Brazil and up to 70% in some macro-regions from 2000 to 2012 reflecting a higher quality in mortality data reporting (Table 6).
Another potential limitation of our study could be the low rate of definition of etiology of cirrhosis-related deaths: only 18% (n = 47,695) and 9% (n = 23,692) of cirrhosis-related deaths had mention of alcoholic liver disease and/or viral hepatitis on their death certificates, respectively. Prevention programs and health policies are strongly dependent on the etiology of liver disease to be tackled. These rates are probably underestimated and it might be related to quality of data registration. The introduction of ICD-10 coding added a more detailed information on the etiology of liver diseases and cirrhosis-related deaths. However, the ICD-10 categories do not match well to current clinical diagnoses and in many cases etiology remains unclear. Sheron et al described that a half of liver-related deaths do not have an etiology recorded when analyzing raw data files from the WHO mortality database since 2000.32 Therefore, it is difficult to estimate with accuracy the percentage of liver deaths that occur as a result of viral hepatitis, non-alcoholic fatty liver disease or excessive alcohol consumption.
The major strength of this study was the estimation of the burden of cirrhosis mortality by analyzing individual data from a nationwide database (SIM) provided by the Brazilian Ministry of Health. SIM has registered causes of death based on DC classified by ICD codes since 1979 (ICD-9 from 1979 to 1995 and ICD-10 from 1996 to today). Since 1999, primary, secondary and contributing causes of death have been available on the database. Mortality data has been systematically updated by the Brazilian Unified Health System Information Technology Department. Death by cirrhosis was defined as the presence of the specific ICD-10 in any field of the DC to avoid underestimation of mortality rates. In addition, mortality rates were adjusted for age using the WHO World standard population that allows comparison of our data with different countries worldwide. This analysis of the Brazilian general population may contribute to a better understanding of the burden of liver diseases worldwide. In terms of territory and population, Brazil is the largest country in Latin America and the fifth largest country in the world. In addition, the description of the burden of cirrhosis mortality in Brazil would emphasize the need of prioritization of the development of preventive health policies in chronic liver diseases.
ConclusionAge-standardized cirrhosis mortality rates progressively decreased from 2000 to 2012 in the Brazilian population. However, cirrhosis remains a major public health issue, responsible for more than 20,000 deaths in 2012. This study paves the way for further urgent research to identify major public health concerns permitting to prioritize health policies for the implementation of cost-effective prevention programs and novel treatments for the most frequent liver diseases in Latin American countries and especially in low-income Brazilian regions.
Abbreviations- •
CI: confidence interval.
- •
DATASUS: Brazilian Unified Health System Information Technology Department.
- •
DC: death certificate.
- •
EU: European Union.
- •
IBGE: Brazilian Institute of Geography and Statistics.
- •
ICD: International Classification of Diseases.
- •
SIM: Sistema de Informação sobre Mortalidade - National Registry of Death database.
- •
WHO: World Health Organization.
- •
HP: study concept and design; analysis and interpretation of data; statistical analysis; drafting and critical revision of the manuscript.
- •
AGP: acquisition of data; analysis and interpretation of data and critical revision of the manuscript.
- •
RDB, PML, JF and SWC: interpretation of data and critical revision of the manuscript.
- •
VGV and BG: study supervision, interpretation of data and critical revision of the manuscript.
The authors have no conflict of interest to disclose related to this topic.
GRANTS/FINANCIAL SUPPORTThis work was supported by funding from:Conselho Nacional de Desenvolvimento Cientifico e Tecnologico (CNPq) / Bolsa Jovem Talento (BJT) - Programa Ciên-cias Sem Fronteiras under grant 301520/2014-3; from Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ) and Fundação para Desenvolvimento Cientifico e Tecnologico em Saude (FioTec) under grant IPEC-010-PPE-13.



