



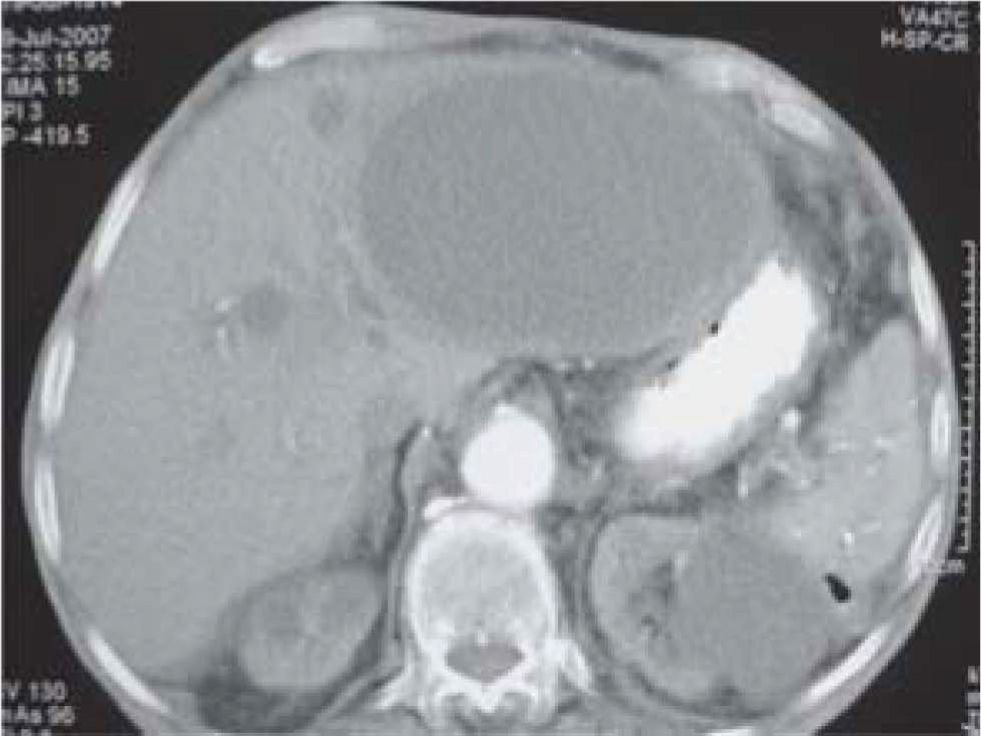
A 93 year-old man was admitted to our Department with fatigue, loss of weight during the last few months and fever up to 38 °C of 5 days duration until one day prior to his admission being treated with antipyretics. The patient had been admitted with similar symptoms 3 months ago to another hospital and the ultrasound of the abdomen had revealed polycystic disease of the liver-kidney-pancreas, but without any other abnormal findings. The patient had become afebrile 2 days after his admission and he was discharged with no established diagnosis. The patient was free from any other medical problems, except from atrial fibrillation, which had been diagnosed 3 years ago and was being treated with acenocoumarol 1 mg/day. On admission, the patient was afebrile and the clinical examination revealed enlarged liver. Laboratory findings included: Hematocrit: 35.2%, WBC: 18,910/mm3, INR: 1.8, C-re-active protein: 91mg/L. An ultrasound of the upper abdomen showed multiple small cysts in the liver, pancreas and the kidneys, but there was also a large cyst of 10 cm diameter in the left lobe of the liver with different characteristics compared to the other cysts (differential diagnosis: haematoma or abscess). Due to the inconclusive results of the ultrasound and the fact that the patient became again febrile on the 3rd day after his admission, a CT of the abdomen was performed. The latter revealed that the large cyst had a thick enhancing wall and perilesional edema, findings compatible with a liver abscess (Figure 1). Serological test for Echinococcus granulosus was negative, but indirect hemagglutination (IHA) test was positive for Entamoeba histolytica (titer: 1/250, normal value: < 1/50). The patient received metronidazole 500 mg tid intravenously for 10 days and then iodoquinol 650 mg orally three times daily for 30 days, with good response and, 6 months after his discharge, uneventful follow up in the clinic.

To our knowledge, this is the first report of amebic liver abscess in a patient with polycystic disease. Amebic liver abscess is the most common extraintestinal manifestation of amebiasis, which is caused by the protozoan Entamoeba histolytica.1 For unknown reasons, amebic liver abscess is more common in adult men. Our patient had not a positive travel history and he was not immunocompromized, but he was living in an endemic area for amebiasis.1 Patients with amebic liver abscess usually present acutely with one to two weeks of fever (38.5 to 39.5 °C) and right upper quadrant pain, with or without concurrent diarrhea.1 However, older patients, similarly to our case, may have a more subacute and insidious presentation with months of intermittent fever, weight loss and hepatomegaly.1,2 Clinical features combined with the radiological findings are usually sufficient to distinguish simple cysts from other cystic lesions, such as liver abscess.2,3 However, in our case, the initial assessment was inconclusive due to the presence of polycystic disease, which causes diagnostic dilemmas and the non-typical clinical history. These difficulties led to a significant delay in diagnosis of the amebic liver abscess, which was finally established based on the CT of the abdomen and the positive serologic test for Entamoeba histolytica.



