



Pulmonary arterial hypertension (PAH) represents a particular subgroup of patients within the wide clinical spectrum of pulmonary hypertension (PH) increasing population, which is characterized by progressive elevation of pulmonary arterial pressures leading to right ventricular failure and death.1 The PH nomenclature and classification deserves always a particular section when scientists and clinicians intent to review this topic, and has been revised several times, most recently during the 2008 World Symposium of PH at Dana Point, California.2
I think this symposium clarified several issues in terms of the previous misuse and misinterpretation while using old abbreviations and nomenclature regarding the heterogeneous group of patients including under the clinical spectrum of PH. Primary pulmonary hypertension (PPH), in our days, means unexplained PH or, in better words, idiopathic pulmonary arterial hypertension (IPAH). This entity has been subject of great interest among pulmonologists, cardiologists, rheumatologists, even some gastroenterologists/ hepatologists, in terms of exploring more through clinical and basic (molecular biology) research nowadays. With the term PPH on board before the Venice and Dana Point meetings in 2003 and 2008, respectively, the term “secondary PH” started to growth in the clinical setting, encompassing very heterogeneous group of diseases including other intrinsic pulmonary vascular diseases similar to PPH as well as disorders that affected the pulmonary venous circulation and conditions that affected the pulmonary circulation by altering lung parenchyma by anatomical and physiological means.
Thus, one of the most important facts during the world Venice symposium was to completely eliminate the term PPH has had been remained during the world PH Evian convention in 1998,3 by proposing to abandon such nomenclature and, thus, by those modifications on board, the PAH group or Group 1 according to the Venice revised classification included the following: 1) idiopathic pulmonary arterial hypertension (IPAH), 2) familial pulmonary arterial hypertension (FPAH), and 3) pulmonary arterial hypertension related to risk factors or associated conditions (APAH) in which portal hypertension has been included in the latter one. Despite the Venice modification to the PH clinical classification, the Dana Point (2008) meeting also introduced even more modifications (Table 1).
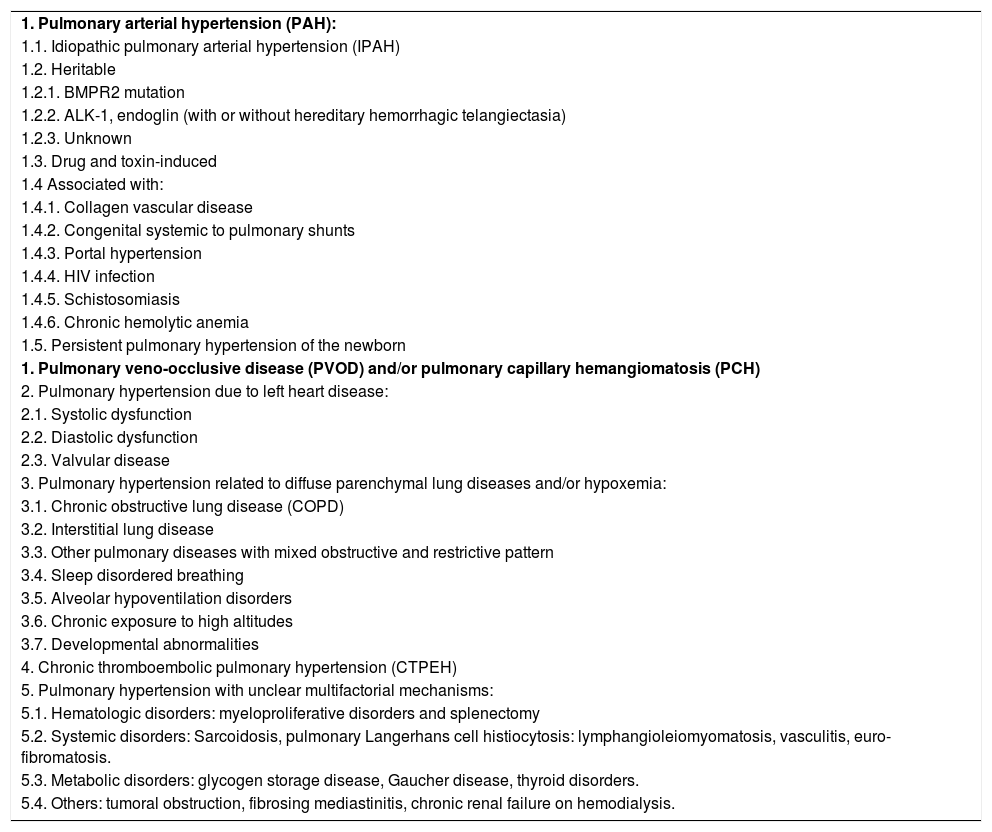
Updated clinical classification of pulmonary hypertension (dana point 2008).
| 1. Pulmonary arterial hypertension (PAH): |
| 1.1. Idiopathic pulmonary arterial hypertension (IPAH) |
| 1.2. Heritable |
| 1.2.1. BMPR2 mutation |
| 1.2.2. ALK-1, endoglin (with or without hereditary hemorrhagic telangiectasia) |
| 1.2.3. Unknown |
| 1.3. Drug and toxin-induced |
| 1.4 Associated with: |
| 1.4.1. Collagen vascular disease |
| 1.4.2. Congenital systemic to pulmonary shunts |
| 1.4.3. Portal hypertension |
| 1.4.4. HIV infection |
| 1.4.5. Schistosomiasis |
| 1.4.6. Chronic hemolytic anemia |
| 1.5. Persistent pulmonary hypertension of the newborn |
| 1. Pulmonary veno-occlusive disease (PVOD) and/or pulmonary capillary hemangiomatosis (PCH) |
| 2. Pulmonary hypertension due to left heart disease: |
| 2.1. Systolic dysfunction |
| 2.2. Diastolic dysfunction |
| 2.3. Valvular disease |
| 3. Pulmonary hypertension related to diffuse parenchymal lung diseases and/or hypoxemia: |
| 3.1. Chronic obstructive lung disease (COPD) |
| 3.2. Interstitial lung disease |
| 3.3. Other pulmonary diseases with mixed obstructive and restrictive pattern |
| 3.4. Sleep disordered breathing |
| 3.5. Alveolar hypoventilation disorders |
| 3.6. Chronic exposure to high altitudes |
| 3.7. Developmental abnormalities |
| 4. Chronic thromboembolic pulmonary hypertension (CTPEH) |
| 5. Pulmonary hypertension with unclear multifactorial mechanisms: |
| 5.1. Hematologic disorders: myeloproliferative disorders and splenectomy |
| 5.2. Systemic disorders: Sarcoidosis, pulmonary Langerhans cell histiocytosis: lymphangioleiomyomatosis, vasculitis, euro-fibromatosis. |
| 5.3. Metabolic disorders: glycogen storage disease, Gaucher disease, thyroid disorders. |
| 5.4. Others: tumoral obstruction, fibrosing mediastinitis, chronic renal failure on hemodialysis. |
Main modifications to the Venice classification have been marked in bold. ALK-1: activin receptor-like kinase-1. BMPR2: bone morphogenetic protein receptor type 2. HIV: Human Immunodeficiency Virus. Reproduced from: 2. Simonneau G, et al. J Am Coll Cardiol 2009;54 (Suppl):S43-54, with permission from the publisher.
Based on the most updated classification of PH, the case report recently published by Cadden etal.4 in Annals of Hepatology represents case of PAH related to portal hypertension with underlying chronic hepatitis C infection; however is the author’s personal opinion that the authors of the case report misuse the PH nomenclature by abbreviating portopulmonary hypertension as “PPH”. I think that using this abbreviations can cause some confusions and could be misleading, since the Dana Point 2008 classification was intended to identify subgroup of patients that can benefit from specific novel therapies, also in terms of including or enroll them in current placebo, double-blind multicenter, randomized controlled clinical trials while investigating the response of certain therapies in a more homogeneous group of patients, and also very important, in order to avoid miscommunication and confusion between our patients. Nowadays, most of the articles written in the medical literature have been adopted specific abbreviations for portopulmonary hypertension (e.g., POPH), that could avoid confusion among clinicians and researchers,2,5 helping to be familiar with the increasing terminology and nomenclature among this relatively unknown but important entity that has been gaining interest among pulmonary vascular disease clinicians and researchers.
Disclosure of financial support: None
Statement of proprietary interest: None
Institutional review board approval: N/A



