



Patients with Hepatitis B viral (HBV) infection harbor eight genotypes (A-H) with distinct geographical distributions.1 Information on the prevalence of HBV genotypes in India remains scanty as are the concerned clinical registries.2 Genotypes D and A are considered as the more prevalent genotypes, along with reports on equitable distribution of genotype D and A in certain populations of India.2,3 The D genotype was also identified as the most predominant form of HBV in north, east and south India.4-6Association of genotype C with higher viral load and elevated serum alanine transaminase (ALT) levels has also been reported.7 In comparison, there are no reports on the incidence of the B genotype of HBV from India. We identified the genotype B among HBV infected patients and report this incidence from India for the first time.
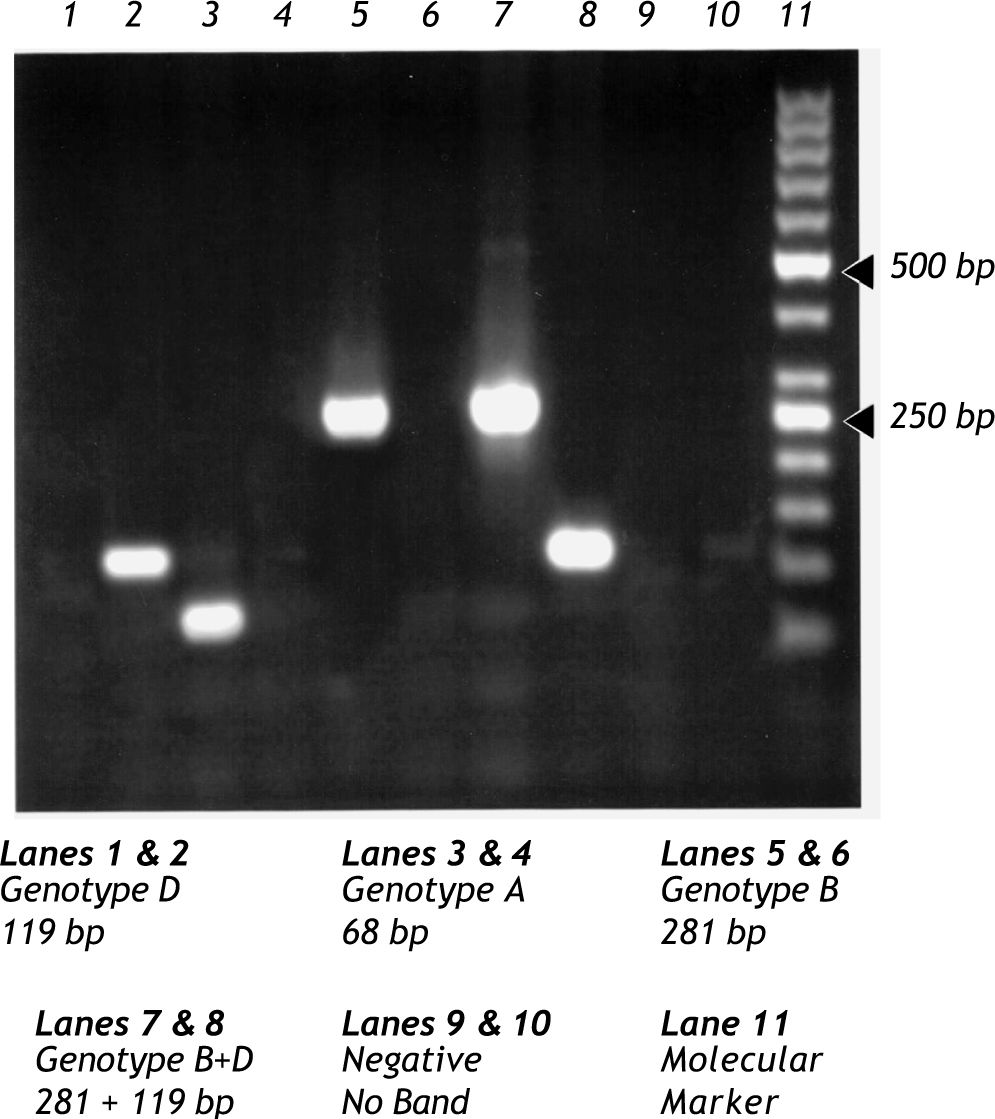
Blood samples were taken from patients (N = 96; Age = 38.5 ± 12.5; seropositive for HBsAg for > 6 months) reporting to Asian Institute of Gastroenterology, a tertiary care hospital at Hyderabad, India. HBV genotyping of the patients involved extraction of viral DNA from 500 pL of serum, using an in house, type specific primer based nested PCR assay employing primers designed on the basis of conserved nature of nucleotide sequences in regions of the pre-S1 through S genes of HBV.8 Extracted DNA was subjected to first round PCR involving universal primers and using an Eppendorf thermocycler (Eppendorf, Germany) for forty cycles. The derived amplicons were further amplified for two rounds of separate PCR of forty cycles each using type-specific (Mix-A and Mix-B) primers.8 HBV genotypes were determined by identifying the genotype-specific DNA bands upon electrophoresis on 3% agarose gels stained with ethidium bromide and evaluated in comparison to the migration pattern of a 50bp DNA ladder under UV light8 (Figure 1) using a gel documentation system (Vilber Lourmat, France). HBV genotyping was noted to be in the order of D (N = 80; 69.5%) > A (N =10; 8.6%) > B (N = 3; 2.6%) or B+ D (N = 3; 2.6%). Quantification of HBV DNA was performed upon amplification by real-time PCR using 5’ nuclease technology (Cobas® Taqman® HBV Kit employing COBAS® Taqman® 48 analyzer) as per the manufacturer’s (Roche Molecular Systems, USA) instructions. Higher viral load (7.68 × 108 copies/mL) was associated in patients with elevated serum ALT activity (> 64 IU/L), as compared to those with much lesser viral load (0.74× 106 copies/mL) with lesser serum ALT activity (< 64 IU/L). Majority of the patients (86.3%) also tested negative for HBeAg upon serological analysis (Amar-EASE BN-96; General Biological, Taiwan).
 and one mixed type (B+D).")
While HBV genotype B is reported to be predominantly occurring in Far East and Southeast Asia, its incidence is not so far reported from India. Interestingly, about 2% of the examined patients also harbored mixed infections of genotypes B and D in the present study, which was hitherto unknown in India. The observed high prevalence of genotype D in chronic hepatitis patients is in accord with similar reports from this part of the country.6 A majority of our study subjects also tested negative for HBeAg, indicating close association of precore stop codon mutations more often with genotype D as suggested earlier.7 Our results also confirmed the notion of association of higher HBV DNA levels with elevated ALT, bilirubin and international normalized ratio (INR) values. Even though the present study is limited by inadequate population, detection of genotype B for the first time in India as well as its coexistence with common genotype D are of relevance in determining demographic transmission patterns in the Indian scenario. However, this preliminary findings of identification of genotype B by type specific PCR will be further confirmed by direct sequencing of the target amplicons. Long-term follow-up studies, investigating host factors at various phases of viral infection with different viral genotypes should help to unravel the pathogenic process and outcome of HBV induced liver disease in India.



