




Hepatitis C virus is one of the most common causes of chronic liver disease and one of the principal indications for liver transplantation. The prevalence and incidence worldwide is variable, although there may be some similarities among different regions. Worldwide prevalence has been estimated around 3.1% or 170 million infected people.
The Latin America region has one of the lowest prevalence around the world with an overall prevalence estimated around 1.23%, nevertheless it varies from country to country and even between regions of the same country. Although the principal route of transmission continues being blood transfusion, the epidemiological change around the world is affecting our region, increasing the virus transmission among intravenous drugs users. Also in Latin America the most prevalent genotype is 1 different from other regions like Africa and Asia.
The knowledge of epidemiology of Hepatitis C in our region is basic for the prevention and treatment of this arising disease, and further research with greater general population based studies must be carried out.
The most frequent agent responsible for the parentally transmitted cases of hepatitis non A non B is the hepatitis C virus (HCV), a spherical single stranded ribonucleic acid (RNA) virus, member of the Flaviviridae family, Hepadnavirus, discovered by Choo et al in 1989.1,2 According to the World Health Organization (WHO), over 170 million people is infected with HCV worldwide, corresponding nowadays to a 3% of the world’s population impacting importantly public health all over the world.3 The infection with this virus may predispose to more serious problems. Some studies have shown that HCV can conduct to liver cirrhosis in almost 20% of the patients infected (enhanced potentially with the alcohol in-take)4,5 and 1 to 4% of those cirrhotic patients, may develop hepatocellular carcinoma (HCC).5,6
Some studies carried out in Latin-American countries showed HCC has a poor prognosis since most of the time is diagnosed too late: whether the tumor is significantly large or cirrhosis is too advanced. This explains why the life expectancy of HCC is measured only in weeks or months.7
On the other side, many routes of transmission have been described; the most important is the transmission through blood transfusions and intravenous drug users (IVDU), although the sexual and perinatal transmissions have an important impact too.8 The contaminated-blood transfusion was the most common route until some decades ago when a stricter control was implemented.8,9 Furthermore the increasing amount of intravenous drug users and the individuals that practice unprotected sex has shown a parallel increment in the incidence of diseases like HIV and HCV.10 Meanwhile, the perinatal transmission is the most important route of dissemination in children.11 There is also reported the occupational factor of contracting this infection; the risk of being infected by stick from an infected patient in the high risk population (health care workers, principally) is about 1%, although some specialists have a higher possibility of almost 5% in a 30-year career. Nevertheless the incidence of this last form of transmission is of approximately 1:10,000.12
The prevalence and incidence worldwide is variable, although there are some similarities. All across the world, the prevalence tends to be higher in men than in women, and the most prevalent age group is of individuals over 40. In developing countries the main risk factor continues to be the transfusions while in developed countries the use of intravenous drugs is the most important means of transmission.
In Europe the prevalence is about 1% with an overall incidence of 6.7 cases per 100,000 inhabitants with the higher rates in Ireland, Finland and Sweden; finding an increase in the overall rate. Although the gender-related affection is like in other regions of the world, in Europe was found that the virus affected most commonly a younger group of age (25 to 44 years old).13
Interestingly, the highest prevalence of the HCV infection is found in Africa with a prevalence of 5.3% or 31.9 million inhabitants. The most endemic is Central Africa (Burundi, Cameroon) and the lowest is the south and east of the continent. Again, the IV drug users and the unsafe injection practices were the most common means of transmission.13 Moreover, Egypt has the highest reservoir of HCV in the world showing a prevalence of 11% to 14% or approximately 10 million inhabitants. Even though in Cairo and Alexandria the prevalence of infection is low, the Eastern Mediterranean has a 4.6% or 21.3 million inhabitants infected, second only to Africa with a very similar distribution among gender and age.14 In South-East Asia the prevalence is of 2.5% or 32.3 million individuals, while in the rest of the continent and the western pacific is of 3.9% or 62.2 million people.13
Regarding to the Americas, in Canada the prevalence is 0.8% approximately and in the United States is 1.3% or 3.2 million inhabitants, being the non-Hispanic black people the most affected, rather than non-Hispanic whites or Mexican Americans. The incidence in this region has diminished in the last decades; although is estimated that the infection still causes from 8,000 to 10,000 deaths per year as liver complications or HCC.13
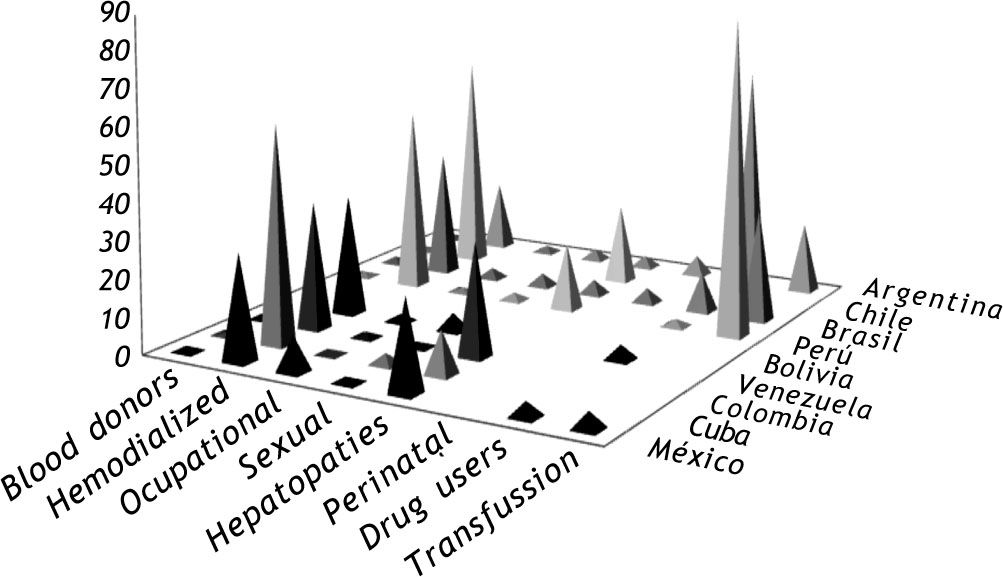
In Latin America the overall prevalence is about 1.23%,13,15 however it varies from country to country. While in the south-east of Brazil is from 0.8% to 2.8% and in the north-east of the country is from 1.7% to 3.4%, with a distribution similar to other regions of the world,2,13 in Chile is considered to be from 0.2% to 0.3%,13 even though a recent study reports a prevalence of 1.15% and an incidence of 15 per 100,000 per year16 and in Mexico is of 1.6%, though recent research have found a prevalence of 0.4%17 and 0.47% to 1.2%.5 Interestingly in a cohort study in Peru involving risk population a seroprevalence rate of 11.7% to 15.6% and a higher prevalence among females were found.18(Figure 1) In Colombia it is estimated that 400,000 to 500,000 people is infected. 15 In a consensus that took place in 2007, Argentina was concluded to have an overall prevalence of 2.2% and 5.8% and was mostly attributable to IV drug use (54%) and transfusions before 1994.19(Figure 2) Some other countries show a much lower incidence: in Venezuela, Monsalve-Castillo, et al. reported an incidence among drug users of 1%20 and in Cuba a prevalence of 0.6% in a group of blood donators was reported. 21 León et al found an overall prevalence of 0.5% in a study carried out in Boli-via22(Figure 1).


There have been described 11 HCV genotypes (from 1 to 11), many subtypes (a, b, c and so forth), and approximately 100 different strains based on the virus genome heterogeneity. It has been found that genotypes 1 and 3 are worldwide distributed. 1a is mostly found in northern Europe and North America, while 1b is predominantly found in Southern and Eastern Europe and Japan finding that this genotype is the most common of all, which is consistent within several studies.13,23 Genotype 2 has a similar distribution but in less proportion than genotype 1. Genotype 3 is endemic in South-East Asia while genotype 4 is characteristically prevalent in Middle East, Egypt and central Africa. Genotype 5 is almost exclusively found in South Africa, while genotypes 6 to 11 are less common and most of them are distributed in Asia.13
In conclusion, through the last decades, the incidence of HCV infection and its complications have been increasing despite the technology and knowledge acquired. The chronic nature of this infection constitutes a serious threat to the world’s public health now and all through the next century18, therefore closely attention and accurate preventive actions have to be taken.
The information previously described demonstrates the impact of this infection; however it is underestimated since the results reported were concluded from specific risk groups or small samples of the general population. Therefore, they are not entirely reliable for describing the whole population. Some countries in Latin-America still need more studies about this.



