



A 51-year-old man with end-stage renal failure presented with 24 hours history of abdominal pain and fever. Initial clinical examination revealed muscular resistance and generalized abdominal tenderness. A secondary bacterial peritonitis was suspected.
The patient was treated conservatively with intravenous antibiotics but his clinical status deteriorated and he became hypotensive.
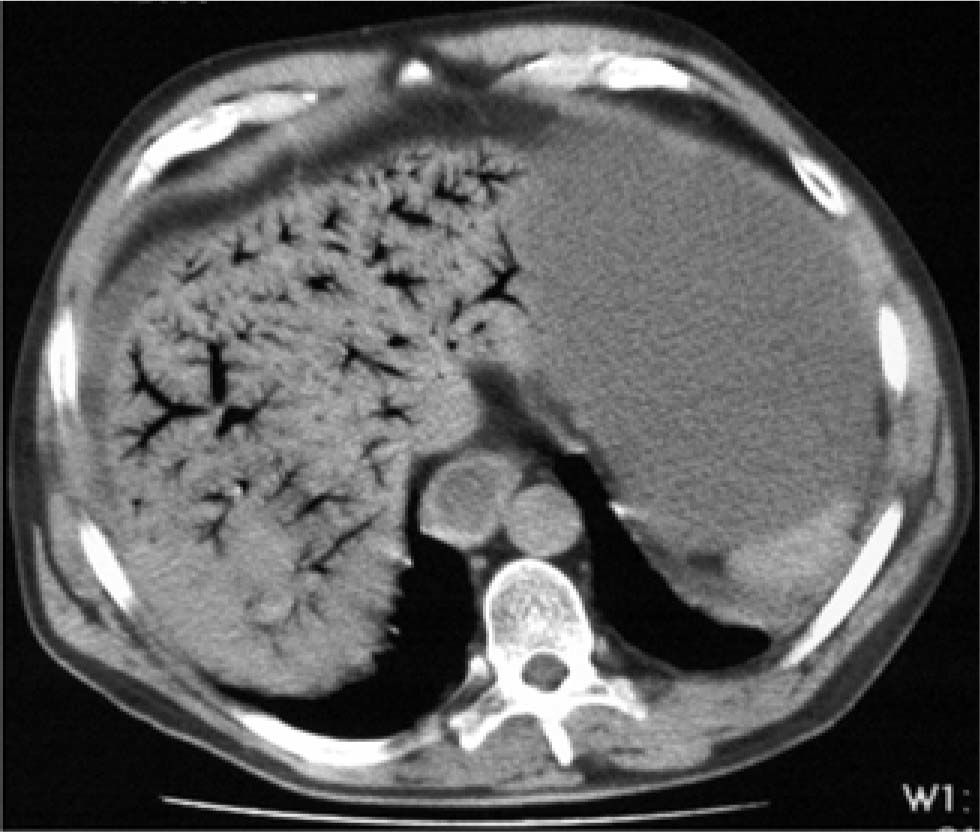
Blood-test revealed pH 7.23 and WCC 20 × 103. CT scan demonstrated distended small-bowel loops, pneumatosis intestinalis and hepatic portal venous gas (HPVG). A large venous thrombus involving superior mesenteric and splenic veins and hepatic portal vein was described (Figure 1). Mesenteric ischemia was diagnosed.
.")
The patient died an hour after the diagnosis was done and it was impossible any other treatment.
HPVG is usually associated with a guarded prognosis and mortality rate approaching 75%. Usually, HPVG is due to intestinal necrosis(72%), although more recent literature has reported a decreased mortality rate(25%) due to early diagnosis.1
Iannitti et al. reported 26 patients with gas in the portal venous system as imaged by CT. HPVG on CT is associated with a wide range of pathologies that no necessarily warrant surgical management. Clinical presentation should be correlated with the presence of HPVG and other associated CT finding prior to deciding whether surgery should be performed.2



