






Background. Liver stiffness measurement (LSM) using Fibroscan® is an increasingly popular non-invasive me¬thod for quantifying liver fibrosis in patients with chronic viral hepatitis. We aimed to explore potential im¬pact of Fibroscan® on clinical management.
Material and methods. 133 patients with chronic hepatitis B (HBV, n = 75) or C (HCV, n = 58) underwent Fibroscan® measurement. LSM results were compared with li-ver biopsy results, ultrasound, and APRI-scores, and the impact of LSM on clinical management was evalua¬ted.
Results. LSM results indicated fibrosis stage F0-F1 in 84 patients (63%), F2 in 28 (21%), F3 in 8 (6%), and F4 in 13 patients (10%). Nineteen patients had liver biopsies within one year of LSM. In ten patients, LSM and biopsy showed the same fibrosis stage, in 8 there was one stage difference, and in 1 three stages di¬fference. Ultrasound only showed cirrhosis in three patients, who all exhibited advanced cirrhosis at LSM. There was a statistically significant, but weak correlation between LSM results and APRI scores (r = 0.31, p-value < 0.001). LSM results changed clinical management in 39% of patients (55 cases): in 15 patients antivi¬ral treatment was indicated, in 21 patients surveillance for hepatocellular carcinoma was indicated, and 19 successfully treated hepatitis C patients could be discharged from clinical follow-up in absence of severe fibrosis or cirrhosis.
Conclusion. LSM appears to be a valuable non-invasive tool to manage patients with chronic viral hepatitis in clinical practice.
Hepatitis B and C are among the most important causes of liver cirrhosis worldwide. During the last decade, there have been dramatic developments in the treatment of viral hepatitis. Hepatitis C (HCV) can be cured with current standard-of-care treat-ment (pegylated interferon plus ribavirin) in about 50% of patients with virus genotypes 1 or 4, and in 80-90% of patients with genotypes 2 or 3.1–3 Al¬though the results of hepatitis B (HBV) treatment are less satisfying, significant progress has also been made in this field. To treat hepatitis B, one can choose between treatment with pegylated interferon (usually for one year)4,5 or suppression of HBV DNA by long-term treatment with powerful nucleos(t)ide analogues like entecavir or tenofovir.6–8
The extent of liver fibrosis often plays an impor¬tant role in the decision to start treatment in pa-tients with viral hepatitis. Moreover, patients with viral hepatitis and severe liver fibrosis or cirrhosis should have ultrasonographic surveillance for hepa-tocellular carcinoma (HCC).9 Liver biopsy still has a central role in the assessment of the extent of liver fi-brosis. Disadvantages of liver biopsies are a (small) risk of complications and mortality, and the risk of underestimating the extent of fibrosis because of sam¬pling error, depending on biopsy length.10 A relative¬ly new alternative for the assessment of liver fibrosis is liver stiffness measurement (LSM) using Fibros-can,® which determines the stiffness of the liver as a parameter of the extent of fibrosis or cirrhosis.11,12 Another possibility is to assess the extent of fibrosis using a combination of serum markers, for example APRI (the AST to Platelet Ratio Index).13
Currently, Fibroscan® devices are not widely available, but their use is expected to increase. The reliability of liver stiffness measurements has been demonstrated in patients with viral hepatitis and with the cholestatic liver diseases primary biliary ci-rrhosis or primary sclerosing cholangitis.14,15 An ad¬vantage of Fibroscan® is that measurements can easily be repeated, to monitor progression of fibro-sis. We expect that physicians from various discipli¬nes will be confronted with LSM with increasing frequency. Virtually no data are available on the im¬pact of Fibroscan® on patient management in clini¬cal practice. Fibroscan® could affect patient management by indicating need for antiviral therapy based on presence of significant fibrosis, need for he-patocellular cancer surveillance based on presence of severe fibrosis or cirrhosis or allowing patient dis-charge from further follow up after successful anti¬viral therapy based on absence of severe fibrosis. We therefore report our experiences with liver stiffness measurements using Fibroscan® in patient manage¬ment in 133 patients with chronic viral hepatitis.
Material and MethodsBetween 2006 and 2008, 142 patients with chro¬nic hepatitis B or C from the University Medical Center Utrecht underwent liver stiffness measure¬ments. In nine patients (6%) no reliable LSM resul¬ts could be obtained. The remaining 133 patients were included in this study. Antiviral treatment was recommended after LSM based on AASL and EASL guidelines.16–19 LSM results indicating significant fi¬brosis (> stage F2), in combination with significant viral load (> 2 x 103 IU/mL or > 2 x 104 IU/mL, de¬pending on HBeAg status) signified a treatment in¬dication for hepatitis B. In case of hepatitis C genotypes 2 or 3, antiviral treatment was advised regardless of LSM results. For genotypes 1 and 4, treatment was recommended in case of fibrosis stage > F2. Surveillance for hepatocellular carcinoma was advised in case of fibrosis stage > F3 (severe fibrosis or cirrhosis).9 Hepatitis C patients who had sustai¬ned virological response after antiviral treatment and LSM results < F2 could be discharged from cli¬nical follow-up.
Liver stiffness measurementsIndication to perform Fibroscan® was need to ob¬tain non-invasive information on extent of fibrosis in patients with chronic viral hepatitis. This infor¬mation was either not present from other investiga¬tions or alternatively, served as baseline measurement for future follow up. Liver stiffness measure¬ments were performed by one experienced investiga¬tor, who was not informed about clinical patient data, using a Fibroscan® device (Echosens, Paris, France). The Fibroscan® is a mobile device, which sends an elastic shear wave through the liver. The velocity of propagation of this wave is assessed as a measure of the elasticity, or the stiffness, of the liver tissue. Higher liver stiffness, indicating more fibro-sis, causes the shear wave to move faster.11 Liver stiffness is expressed in kilopascals (kPa). More in¬formation about Fibroscan® can be found at www.echosens.com. Before each liver stiffness mea¬surement, ultrasound examination was performed to exclude ascites, vascular structures, cysts, and other abnormalities that could influence the reliabi¬lity of the measurements. Liver stiffness measure¬ments were performed on the right lobe of the liver, in an intercostal space, with the patient positioned on his back with the right arm in maximal abduc¬tion. Measurement depths were 25 to 65 mm below the skin surface. The median value of ten successful measurements was considered representative for the stiffness of the liver. Only results with at least ten successful measurements and a success percentage (defined as the number of successful measurements divided by the total number of measurements) of at least 60% were considered reliable and included in the analyses. Results were categorized according to the criteria by Castera, et al.:20
- •
< 7.1 kPa no or minimal fibrosis (F0-F1).
- •
7.1–9.4 kPa moderate fibrosis (F2).
- •
9.5–12.4 kPa severe fibrosis (F3).
- •
≥ 12.5 kPa cirrhosis (F4).
Serum levels of AST, ALT, γ-GT, total bilirubin, alkaline phosphatase, albumin, platelet counts, and prothrombin times were measured by standard as¬says at our hospital laboratory, within 6 months‘ time of liver stiffness measurements. APRI scores were calculated for all patients as (AST/upper level of normal range for AST)/platelet count x 100. The APRI score can be used as a predictive measure for the extent of liver fibrosis.21 Normal scores are bet¬ween 0 and 0.5. Scores above 0.5 indicate significant fibrosis (> F2), while scores higher than 1 suggest cirrhosis (F4).13,21
Liver biopsiesIn several patients liver biopsies had been perfor¬med as part of standard care. Decision to perform liver biopsy had been taken by the treating physi¬cian, based on clinical indications such as increased transaminase values, increased age or other risk factors for significant fibrosis. Fibrosis was scored by an experienced pathologist using the METAVIR classification.22 Results of liver biopsies performed within one year of liver stiffness measurements were included in the analyses.
Ultrasound examinationsAbdominal ultrasound examinations evaluated by an experienced radiologist and performed within six months of liver stiffness measurements were used in this study.
Statistical analysesFor continuous variables medians, ranges and in¬terquartile ranges were calculated. Categorical va¬riables were reported as proportions. A statistically significant difference in LSM results between HBV and HCV patients was assumed when the 95% confi¬dence intervals of the proportions of patients with a specific fibrosis stage in either group did not over¬lap. Spearman’s correlation coefficient was used to assess the correlation between LSM results and APRI scores. A p-value < 0.05 was considered sta¬tistically significant. There is no absolute gold standard for staging liver fibrosis in clinical practice, since liver biopsies may underestimate degree of fibrosis due to sampling error. In the current work, sensitivity, specificity, positive and negative predic¬tive values of LSM to predict significant fibrosis, severe fibrosis or cirrhosis with liver biopsies are gi¬ven in those patients who had liver biopsy within 1 year from LSM measurement. We also calculated sensitivity, specificity and predictive values of ab¬dominal ultrasoundation and APRI score to predict ci¬rrhosis as measured with LSM. Data were analyzed using SPSS version 16.0 (SPSS Inc, Chicago IL, USA).
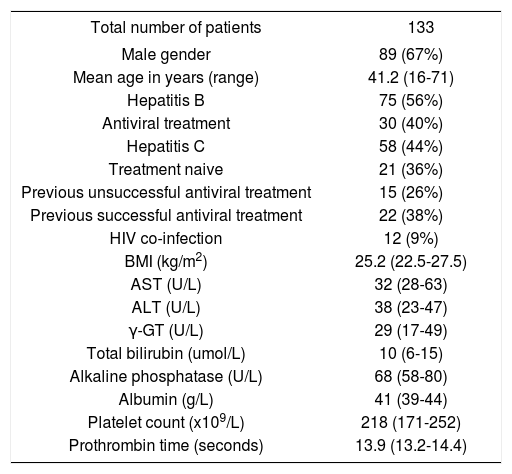
ResultsBaseline characteristicsLiver stiffness measurements were not successful in nine of 142 patients (6%), because of obesity (n = 3), or a success percentage below 60% (n = 6). Baseline characteristics and laboratory parameters of the remaining 133 patients are given in table 1. Seven¬ty-five patients had chronic hepatitis B (30 of whom were on long-term antiviral treatment with nucleos(t)ide analogues at time of LSM), and 58 had chronic hepatitis C. Of the latter group, 37 patients had undergone antiviral treatment before LSM, with sustained virological response in 22 patients (59%). Twelve patients (9%) were co-infected with HIV.
Baseline characteristics of 133 patients with chronic hepatitis B or C.
| Total number of patients | 133 |
|---|---|
| Male gender | 89 (67%) |
| Mean age in years (range) | 41.2 (16-71) |
| Hepatitis B | 75 (56%) |
| Antiviral treatment | 30 (40%) |
| Hepatitis C | 58 (44%) |
| Treatment naive | 21 (36%) |
| Previous unsuccessful antiviral treatment | 15 (26%) |
| Previous successful antiviral treatment | 22 (38%) |
| HIV co-infection | 12 (9%) |
| BMI (kg/m2) | 25.2 (22.5-27.5) |
| AST (U/L) | 32 (28-63) |
| ALT (U/L) | 38 (23-47) |
| γ-GT (U/L) | 29 (17-49) |
| Total bilirubin (umol/L) | 10 (6-15) |
| Alkaline phosphatase (U/L) | 68 (58-80) |
| Albumin (g/L) | 41 (39-44) |
| Platelet count (x109/L) | 218 (171-252) |
| Prothrombin time (seconds) | 13.9 (13.2-14.4) |
Values are medians (interquartile range) or numbers (proportion). LSM: Liver stiffness measurement. AST: Aspartate aminotransferase. ALT: Alanine aminotransferase. γ-GT: γ-glutamyl-transpeptidase.
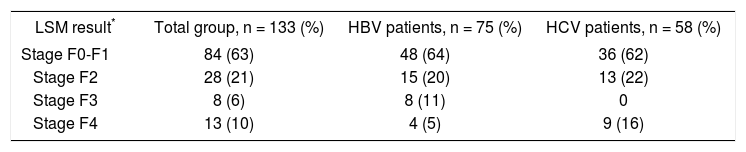
Table 2 shows LSM results for the total group and according to type of viral hepatitis. Eighty-four patients (63%) had no to minimal fibrosis (F0-F1) on LSM, 28 patients (21%) had moderate fibrosis (F2), 8 patients (6%) had severe fibrosis (F3), and 13 patients (10%) had cirrhosis (F4). No significant differences were seen between HBV and HCV pa¬tients. Fourteen patients had two successful liver stiffness measurements, with a median interval of 21 months (range 5–30 months). In 11 patients (79%) the results of the first and second measure¬ments indicated the same fibrosis stage (F0-F1 in 10 patients and F4 in one patient). One HBV pa¬tient went from stage F0–F1 (5.7 kPa) to stage F3 (10.2 kPa) in 8 months. Two HCV patients went from stage F2 (7.1 and 8.7 kPa, respectively) to sta¬ge F0-F1 (5.4 and 6.7 kPa) in 30 and 29 months, respectively. Both had relatively small absolute de¬creases in LSM results (1.7 and 2.0 kPa), and both underwent unsuccessful treatment with pegylated interferon and ribavirin before the first LSM.
LSM results for the total group and according to type of hepatitis virus.
| LSM result* | Total group, n = 133 (%) | HBV patients, n = 75 (%) | HCV patients, n = 58 (%) |
|---|---|---|---|
| Stage F0-F1 | 84 (63) | 48 (64) | 36 (62) |
| Stage F2 | 28 (21) | 15 (20) | 13 (22) |
| Stage F3 | 8 (6) | 8 (11) | 0 |
| Stage F4 | 13 (10) | 4 (5) | 9 (16) |
LSM result classified according to criteria by Castera, et al.: F0-F1 < 7.1 kPa, F2 7.1-9.4 kPa, F3 9.5-12.4 kPa, and F4 > 12.5 kPa.20 LSM: Liver stiffness measurement. HBV: Hepatitis B virus. HCV: Hepatitis C virus.
In figure 1, liver biopsy results are compared with LSM results for the 19 patients in whom these investigations were performed within one year of each other. LSM and liver biopsy showed the same stage of liver fibrosis in 10 patients (53%), while LSM results were one fibrosis stage higher than biopsy results in 5 patients, three stages higher in one patient, and one stage lower in three patients. In only three pa¬tients the difference in kPa between their LSM results and the nearest limit of their liver biopsy fibrosis sta¬ge was > 2 kPa. Discrepancies between LSM and biopsy results were not related to ALT levels or biop¬sy lengths. Sensitivity, specificity, positive and nega¬tive predictive values of LSM to predict significant fibrosis (F0-F1 vs. > F2) on liver biosy were 0.60, 0.64, 0.38 and 0.82, respectively, and to predict severe fibrosis (F0-F2 vs. > F3) 1.0, 0.94, 0.75 and 1.0, res¬pectively. Since numbers are limited, these data should be regarded with caution. Nevertheless, they are in line with previous reports, and suggest that Fi-broscan® is more reliable to predict severe fibrosis or cirrhosis with indication for hepatocellular carcino¬ma surveillance than to predict significant fibrosis with indication for antiviral therapy.
 and liver biopsies.")
In 65 patients (49%) abdominal ultrasound exa¬minations were performed within six months of LSM. In three patients, all with LSM result stage F4 (13.9, 21.8 and 54.8 kPa, respectively), ultra¬sound results indicated liver cirrhosis. Further in¬vestigation showed thrombocytopenia in the patient with LSM result 21.8 kPa, and both thrombocytope-nia and esophageal varices in the patient with LSM result 54.8 kPa. Both these patients had APRI-sco-res higher than 1.0 (1.04 and 1.33, respectively), while in the third patient the APRI-score was 0.46. In 13 of the remaining 62 patients LSM results indi¬cated severe fibrosis (n = 3) or cirrhosis (n = 9) without any abnormalities at abdominal ultrasound investigation. Sensitivity, specificity, positive and negative predictive values of ultrasound to predict cirrhosis on Fibroscan® (F0-F3 vs. F4) were 0.25, 1.0, 1.0 and 0.85, respectively. Similar results were obtained for prediction of severe fibrosis (F0-F2 vs. > F3: results not shown). These data suggest that ultrasound is quite specific but not very sensitive to predict cirrhosis.
For 127 patients (95%) APRI scores could be calculated within six months of liver stiffness mea¬surements (Table 3)). The six patients for whom no APRI scores were available all had LSM result F0-F1. Median APRI score was 0.41 (range 0.14–3.51). APRI scores were 0-0.49 in 82 patients (65%), 0.50– 0.99 in 33 patients (26%), and > 1.00 in 12 patients (9%). Correlation between LSM results and APRI scores was statistically significant, but not very strong (Spearman’s correlation coefficient 0.31, p-value < 0.001). Strong discrepancies were seen in 11 patients with LSM results F3 or F4 and APRI scores below 0.50, and in 6 patients with LSM results F0-F1 or F2 and APRI scores > 1.00. Sensitivity, speci¬ficity, positive and negative predictive values of APRI score to predict significant fibrosis (F0-F1 vs. ≥ F2) on Fibroscan® were all below 0.5, and to pre¬dict cirrhosis (F0-F3 vs. F4) 0.38, 0.94, 0.42 and 0.93, respectively. Similar results were obtained for prediction of severe fibrosis (F0-F2 vs. ≥ F3: results not shown). These data suggest that APRI score could be of some help to indicate low probability of cirrhosis, but is of no value to predict moderate fi-brosis.
Comparison of LSM results and APRI scores in 127 patients with chronic viral hepatitis.
| APRI score | LSM result | |||
|---|---|---|---|---|
| F0-F1, n = 78 (%) | F2, n = 28 (%) | F3, n = 8 (%) | F4, n = 13 (%) | |
| 0-0.49 | 59 (76) | 12 (43) | 5 (63) | 6 (46) |
| 0.50-0.99 | 17 (22) | 12 (43) | 2 (25) | 2 (15) |
| > 1.00 | 2 (2) | 4 (14) | 1 (12) | 5 (39) |
APRI: AST to platelet ratio index. LSM: Liver stiffness measurement.
Figure 2 summarizes the impact of liver stiffness measurement on clinical practice. LSM results did not change decisions regarding antiviral treatment in 54 of 58 HCV patients (93%). In these patients LSM results were F0-F1, they had already undergo¬ne state of the art HCV treatment, antiviral treat¬ment was already indicated based on a favorable HCV genotype, or abdominal ultrasound examina¬tion had already shown cirrhosis. Of the four remai¬ning HCV patients, three had LSM result F2 (all HCV genotype 1 and previously untreated) and one F4 (genotype 1, previous unsuccessful pegylated in-terferon monotherapy), indicating need for antiviral treatment with pegylated interferon and ribavirin.
 with Fibroscan® on clinical management in 133 patients with chronic viral hepatitis. HCC: Hepatocellular carcinoma.")
Thirty HBV patients were already on long-term antiviral treatment at time of LSM. Of the 45 treat¬ment naive patients, 34 had LSM results F0-F1 and no indication for treatment based on normal transa-minase levels. Of the remaining 11 patients, 8 had LSM result F2, one F3, and two F4, all with signifi¬cant viral loads, indicating need for antiviral thera¬py. One additional HBV patient, who had two liver stiffness measurements in 8 months, and an increase in LSM results of 4.5 kPa during this period, star¬ted entecavir treatment after his second LSM.
In 21 patients (16%) HCC surveillance was initia¬ted based on the presence of previously unknown se¬vere fibrosis (n = 8) or cirrhosis (n = 13) on their LSM results.
Nineteen HCV patients could be discharged from further follow-up, because they underwent successful antiviral treatment and had LSM results < F2, without previously known fibrosis stage.
DiscussionDetermining the extent of liver fibrosis provides important prognostic information in patients with chronic liver disease. Moreover, in viral hepatitis the extent of liver damage often is an important reason to either start or postpone antiviral treat¬ment. Patients with viral hepatitis who have severe fibrosis or cirrhosis should also have surveillance for hepatocellular carcinoma.9 Liver biopsies still have a central role in the assessment of the extent of liver fibrosis. They also provide information about infla¬mmation severity and, occasionally, unexpected diagnoses can be made. Disadvantages of liver biop¬sies are complication risks and the risk of sampling error with underestimation of fibrosis.10,23,24 Mo¬reover, it is not feasible to frequently repeat liver biopsies, while the extent of liver damage can in¬crease at relatively fast rates, especially in hepatitis B. In this paper we discuss our experience in clinical practice with liver stiffness measurements using Fi-broscan® as a non-invasive alternative for liver biopsies in 133 patients with chronic viral hepatitis.
LSM results indicated no or minimal fibrosis (F0-F1) in 84 patients (63%), and cirrhosis (F4) in 13 patients (10%). In 19 patients liver biopsies were performed within six months of LSM. Our compari¬son of LSM with biopsies could be biased: liver biop¬sies could have been performed in those patients because treating physicians did not trust the LSM results, or the other way around. In 9 patients liver biopsies were performed before LSM, and in 10 pa¬tients after LSM. In 10 patients LSM and biopsy showed corresponding results, while in 8 other pa¬tients only one fibrosis stage difference was seen (of¬ten with very small differences in kPa between LSM result and the nearest limit of the biopsy fibrosis stage). Increased ALT levels have been reported to reduce the reliability of LSM, although results in this area are conflicting.12,20,25–27 ALT levels did not appear to be associated with the discrepancies bet¬ween LSM and biopsy results in our patients. Howe¬ver, in only a few patients ALT levels were increased above 100 U/L. Variation in biopsy lengths could not explain discrepancies between LSM and biopsies either. Whether such discrepancies are a result of li¬mitations of LSM or of liver biopsy remains to be determined. Our data on sensitivity, specificity, and positive or negative predicitive value are in line with previous reports, and suggest that Fibroscan® is more reliable to predict severe fibrosis with indica¬tion for hepatocellular carcinoma surveillance than to predict significant fibrosis with indication for an¬tiviral therapy. Nevertheless, our patient numbers are limited, and these data should be viewed with caution.
In 65 patients abdominal ultrasound examinatio¬ns were performed within six months of LSM. Ultra¬sound was found to be highly specific, but not very sensitive to predict cirrhosis. As a consequence, no further investigations are necessary when cirrhosis is found on ultrasound, but further investigations may be considered if ultrasound is normal, depen¬ding on clinical judgement.
APRI scores are easy to calculate, and showed a sig¬nificant, but not very strong correlation with LSM re¬sults (r = 0.31, p-value < 0.001), with large discrepancies between LSM results and APRI scores in 17 patients (13%). In our patients, APRI score was not a good parameter for significant fibrosis, but could be of some value to indicate low probability of cirrhosis.
Liver stiffness measurements had consequences for treatment policies in 39% of patients. In 15 un¬treated patients antiviral treatment was indicated based on increased LSM results, and HCC survei¬llance was indicated in 21 patients. Nineteen other patients with sustained virological response after treatment for HCV could be discharged from further follow-up based on their favorable LSM results.
A limitation of our study is the relatively low number of patients, especially for the comparison of LSM results with liver biopsy results. However, our study population will probably be representative for patient populations in many clinical practices world¬wide, and our experience could aid other clinicians who are dealing with similar situations. Larger, prospective studies will have to clarify the use of both single and longitudinal LSM to assess the ex¬tent and progression of fibrosis in clinical practice.
ConclusionBased on the experiences described in this paper, we conclude that liver stiffness measurement using Fibroscan® appears to be a valuable non-invasive addition to clinical practice in patients with chronic viral hepatitis.
Abbreviations- •
HCV: Hepatitis C virus.
- •
HBV: Hepatitis B virus.
- •
ULN: Upper limit of normal.
- •
HCC: Hepatocellular carcinoma.
- •
LSM: Liver stiffness measurement.
- •
APRI: AST to Platelet Ratio Index.
- •
kPa: Kilopascal.
- •
AST: Aspartate aminotransferase.
- •
ALT: Alanine aminotransferase.
- •
γ-GT: γ-glutamyl-transpeptidase.
- •
HIV: Human immunodeficiency virus.



