



Multiple biliary hamartomas are rare benign malformations of the intrahepatic bile ducts first described by von Meyenburg in 1918. They originate from embryonic bile ducts that fail to involute. These are generally asymptomatic and usually encountered as an incidental finding at imaging, laparotomy or autopsy.
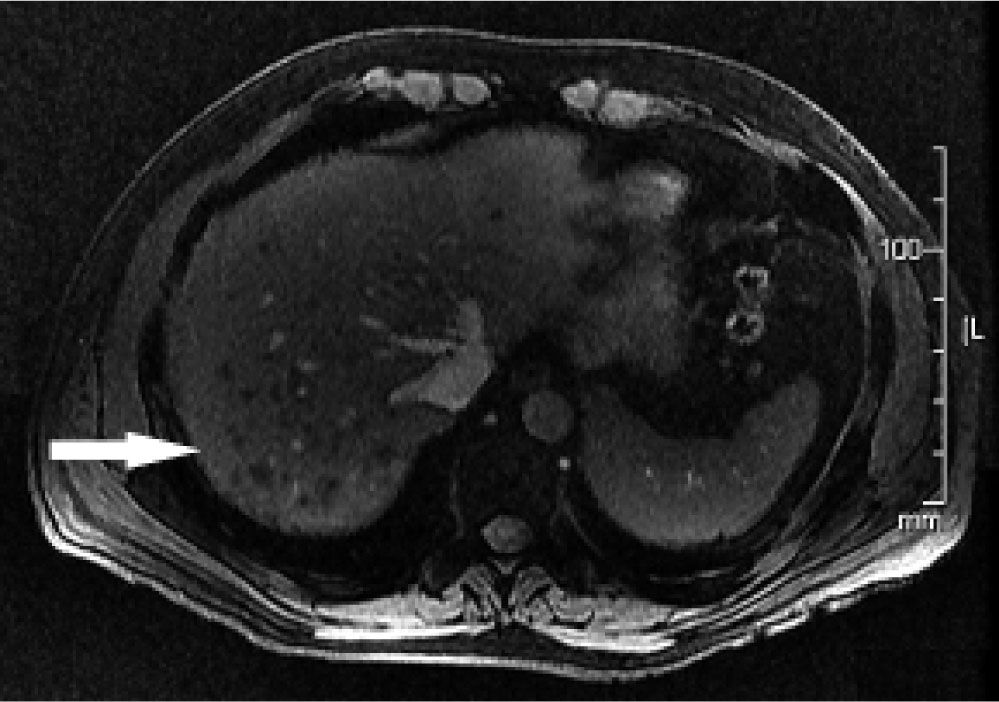
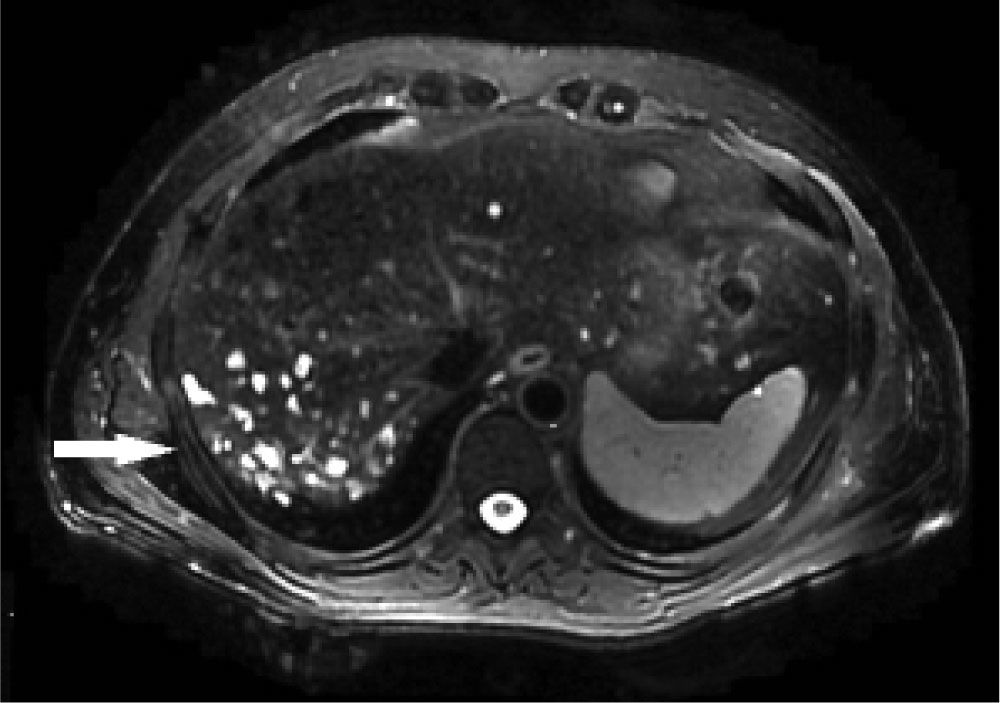
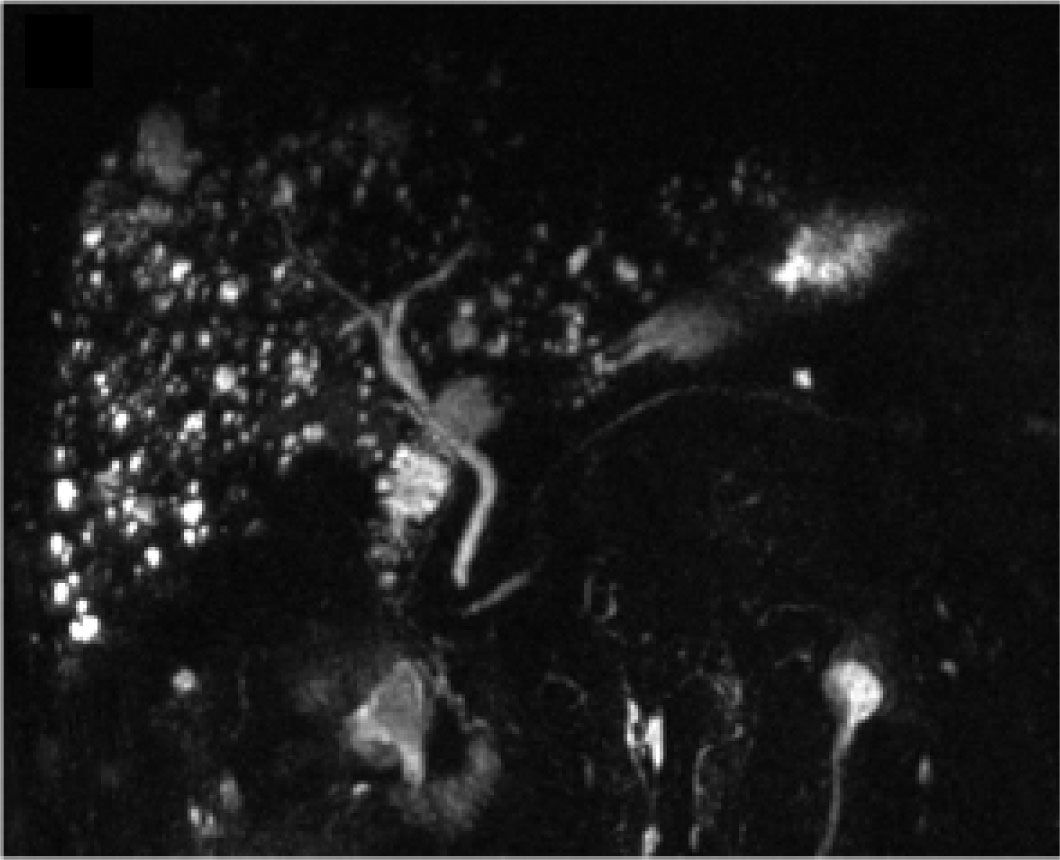
50-year-old man with no medical history was referred due to abnormal liver function tests. Aspartate aminotrans-ferase was 61 IU/L (normal, 0 to 38) and gamma-glutamyl transpeptidase 90 IU/L (normal, 12 to 64). Abdominal ultrasound showed multiple hyper and hypoechoic areas in the liver. Magnetic resonance cholangiopancreatography (MRCP) was also performed. A T1-weighted MR image (Figure 1) revealed multiple hypointense diffuse liver lesions of variable size (< 15 mm). A T2-weighted MR image (Figure 2) revealed these lesions as hyperintense, with MRCP (Figure 3) not showing communication between the cystic lesions and the biliary tract.

.")

These findings were consistent with multiple biliary hamartomas or “von Meyenburg complexes”,1,2 which are a variety of benign cystic lesions of the liver that consist of focal collections of ductlike structures embedded in a fibrous stroma resulting from ductal plate malformation involving the small interlobular bile ducts.1 Biliary hamartomas are rare, clinically asymptomatic, and diagnosis is usually incidental.1-3 Technical advances in radiology have made them easily detectable, providing a more accurate diagnosis to avoid biopsy, which should be performed for confirmation of diagnosis when in doubt.3,4 CT scans can detect multiple, nodular and irregular cystic liver lesions, smaller than 15 mm, with low attenuation and no enhancement on contrast injection.5,6 MRCP can also help in the differentiation of von Meyenburg complexes from liver metastases, polycystic disease and Caroli's disease,2 requiring the administration of intravenous gadolinium. Contrast enhancement is seen in metastatic lesions and Caroli's disease,6 and a lack of communication with the biliary tree can be observed in the latter.4 Even though prevalence of this entity has been reported to be low at autopsy, ranging from 0.69% and as high as 5.6%,5,7 when its diagnosed patients require monitoring because some reports have shown malignant transformation to intrahepatic cholangiocarcinoma.6-8 The use of Ca 19-9 to diagnose malignant transformation should be discouraged, since persistent elevation of this tumor marker has been described in patients with multiple biliary hamartomas without ma-lignancy.9,10
We suggest periodic clinical monitoring and determination of Ca 19-9, and in case of alarm symptoms or elevation of tumor marker, perform MRCP with gadolinium. If a suspicious lesion is found, consider confirming diagnosis with a biopsy.
Conflict of InterestNo conflict of interest statement.



