





Alcoholic Liver Disease (ALD) is a major cause of morbidity and mortality both in the United States and worldwide. In the United States, it is projected that over 2,000,000 persons have ALD, and the mortality for cirrhosis with superimposed alcoholic hepatitis is much worse than that of many common types of cancer. Unfortunately, there is no FDA approved therapy for ALD. We have made major strides in the last decade in identifying mechanisms for the development of liver injury in ALD, and therapies are evolving directed at specific mechanisms. It is clear that life style modification with abstinence, cessation of smoking and weight loss (if overweight) are beneficial. It is also clear that most patients with advanced liver disease have some form of malnutrition, and nutritional supplementation is of benefit. Patients with alcoholic hepatitis that is relatively severe in nature, but not complicated by issues such as infection or GI bleeding, appear to benefit from steroids. A drop in bilirubin should be monitored in steroid treated patients. Pentoxifylline appears to be beneficial in patients with alcoholic hepatitis, especially those with early hepatorenal syndrome. A variety of other agents such as PTU, lecithin, colchicine, and anabolic steroids are probably not effective. Complementary and alternative medicine agents such as zinc, milk thistle, and SAM have great therapeutic rationale. Results of ongoing NIH studies evaluating agents such as specific anti-TNF’s, SAM and Milk Thistle are eagerly awaited. Transplantation is clearly an option for end stage ALD in patients who are abstinent.
Alcoholic liver disease (ALD) is a major cause of morbidity and mortality. Two billion people worldwide consume alcoholic beverages and 76.3 million are estimated by the World Health Organization to have diagnosable alcohol use disorders.1 In the United States, it is estimated that about two thirds of Americans consume alcohol and about 14 million meet the diagnostic criteria for alcohol abuse. The total yearly cost of alcohol abuse in the United State is nearly $ 185 billion, most of it due to lost productivity and motor vehicle accidents.2,3 The prevalence of ALD in the US in conservatively estimated at about 2 million persons. Alcohol remains a critical cause of liver disease in the western world. Approximately 40% - 90% of patients with cirrhosis have a history of alcohol abuse.2 Up to thirty percent of hepatocellular carcinoma cases are attributable to ALD.4 Although the per capita alcohol consumption has declined in the US and Europe, it has increased in Latin America and Asia. The World Health Organization estimates that 14.2% of all adults in Mexico fall into the category of heavy drinkers.1 Thus, alcoholism and ALD remain important health problems facing the developed and developing world.
There appears to be a threshold amount and duration of alcohol intake necessary for the development of ALD. Daily intake of alcohol for 10 to 12 years with doses in excess of 40 to 80 g/d for males and of 20 to 40 g/d for females is generally required to cause alcoholic hepatitis/cirrhosis. Among heavy, long-term alcohol drinkers, approximately 90 to 100% develop fatty liver but only 20 to 35% develop alcoholic hepatitis, and 8 to 20% develop alcoholic cirrhosis. The mechanisms for the development of ALD are multiple (figure 1).5 Alcohol acts as a “potential hepatotoxin”, with the development of liver disease depending on the balance of host attributes and coexisting external factors, such as gender, polymorphisms of alcohol-metabolizing enzymes, immunologic factors, exposures to other substances/drugs, hepatic viral infections, nutritional deficiencies, obesity, etc.5
.")
Unfortunately there is no FDA approved treatment for ALD. Hence, this is an area of ongoing research involving human as well as animal studies. As our knowledge of ALD increases we will better understand the mechanistic basis of presently used treatment modalities. Advances made in the conceptual understanding of alcohol mediated liver injury are being translated into clinical trials. Moreover, as additional mechanisms of liver injury are elucidated, compounds may become available that target novel pathways.5 In this review we mainly present treatment strategies based on results of large randomized human studies, but also touch upon therapeutic options suggested by selected basic research. Therapies reviewed in this article include: lifestyle modification, nutrition, drug therapy and transplantation.
Lifestyle modifications including abstinenceEstablishment and maintenance of abstinence is probably the most important treatment modality in ALD. Abstinence leads to resolution of steatosis and prevents further ongoing liver injury, fibrosis and possibly hepatocellular carcinoma. Only limited studies are available evaluating the effects of abstinence from alcohol on the progression of ALD, but virtually every one of them shows a beneficial effect on patient survival including patients with decompensated cirrhosis.6 Even reducing alcohol consumption has been shown to improve projected survival in ALD.7,8 The so-called “brief interventions” are a simple form of psychological therapy for alcohol abuse which can be performed by non-psychiatric personnel like the patient’s nurse, primary care physician or gastroenterologist. These interventions which involve educating and informing patients about the nature of their problem and providing them with advice regarding how to change their behavior have been shown to effectively reduce alcohol consumption (16 drinks/day to 2.5 drinks/day over 6 yrs in one study).8 Drugs like Naltrexone and Acamprosate also have been shown to reduce or eliminate drinking in some chronic alcoholics but they have not been extensively tested on patients with ALD.
Obesity, like alcohol, is associated with the development of steatosis, steatohepatitis and cirrhosis and may be a major risk factor for progression of ALD.9,10 Hence, it is important for obese patients with ALD to lose weight. Moreover, smoking is a risk factor for more severe ALD and patients are encouraged to quit smoking.11 Cigarette smoking is known to produce oxidative stress, which may be an important underlying mechanism of accelerated liver disease in smokers with ALD.
In summary, therapeutic lifestyle changes in ALD include: ideally, abstinence from alcohol or at least significant reduction in alcohol consumption, weight control and quitting smoking.
Nutritional supportMalnutrition is prevalent in liver disease, and more severe liver disease generally has more severe malnutrition. This was conclusively documented in two large VA Cooperative Studies which evaluated hospitalized patients with alcoholic hepatitis. The first of these studies demonstrated that virtually every patient with alcoholic hepatitis has some degree of malnutrition. The more than 280 patients studied underwent complete nutritional assessments which showed that patients derived almost 50% of their total caloric intake from consumption of alcohol, a substance with little nutritional value. Similar data were generated in the follow up study by the same group.12 In both studies, patients were given a balanced 2500 Kcal hospital diet carefully monitored by a dietician and were encouraged to eat the diet. But only about one third of the patients achieved this objective. In the second study, the patients in the therapy arm of the protocol also received an enteral nutrition support product high in branched chain amino acids as well as the anabolic steroid oxandrolone. Patients were not fed by a feeding tube even if voluntary oral intake was inadequate in either study (probably a study design flaw, in retrospect). Of importance is the fact that an inverse relation was noted between the energy intake and mortality rate. Moreover the degree of malnutrition correlated with the development of serious complications such as encephalopahy, ascites and hepatorenal syndrome.
Initial interest in nutrition therapy was stimulated in 1948 by Patek and colleagues who demonstrated that a “nutritious diet” improved the 5-year outcome of patients with alcoholic cirrhosis compared with historical controls.13 Subsequent studies further supported nutritional support in hospitalized patients with ALD. In one trial, nutritional supplementation through a feeding tube significantly improved liver function as assessed by serum bilirubin levels and antipyrine clearance compared to inpatients that ate a hospital diet.14 Probably the most compelling data in favor of nutrition therapy come from a multicenter study by Cabre and co-workers who randomized severe alcoholic hepatitis patients to receive either Prednisone, 40 mg daily or a liver specific formula containing 2000 calories per day through a feeding tube.15 The 1 month mortality was the same in both groups but the 1 year mortality was significantly lower in the enteral nutrition group compared to the glucocorticoid group mainly due to fewer infectious complications. This study demonstrates the importance of enteral nutrition in severe alcoholic hepatitis. We do not hesitate to place a nasogastric feeding tube as soon as alcoholic hepatitis patients are admitted to the hospital if it is necessary to ensure adequate enteral nutrition.
Limited studies of nutritional support in liver patients are available in the outpatient setting. Hirsch and colleagues demonstrated that outpatients from a liver clinic taking an enteral nutrition supplement (1000 Kcal and 34 gm of protein) had significantly improved protein intake and fewer hospitalizations in comparison with those not receiving the supplements.16 The same group later showed that enteral supplements improved nutritional status and immune function in outpatients with alcoholic cirrhosis.
In summary, nutritional supplementation clearly improves nutritional status and may enhance liver function and decrease morbidity and mortality in some patients. Assessment of nutritional status and nutritional supplementation should be aggressively pursued in both inpatients and outpatients with ALD, especially in patients with more severe disease such as severe alcoholic hepatitis or cirrhosis.
Drug TherapyGlucocorticoidsCorticosteroids have been the most extensively studied (and possibly the most controversial) treatment for patients with alcoholic hepatitis/cirrhosis. Over a dozen randomized controlled trials and a number of meta-analyses of corticosteroid therapy in patients with alcoholic hepatitis have reported variable results with reference to short term and long term survival.17-21 In a recent published clinical trial from the UK, Phillips and colleagues randomized 101 acute alcoholic hepatitis patients to corticosteroids (prednisone 30 mg tab daily or methylprednisone 24 mg intravenously) or an antioxidant cocktail (8 antioxidants). At 30 days, survival was 70% in corticosteroid group (37/53), whereas the antioxidant group (24/46) had a 54% survival.22
Mathurin, et al. reanalyzed the individual data of three recent randomized placebo controlled, double blind trials of corticosteroids in severe AH to evaluate the efficacy of corticosteroid therapy in a group of patients with Discriminant Function (DF) ***entity***32 (102 placebo, and 113 corticosteroid patients). A higher short term survival benefit was observed at 28 days in the corticosteroid group than in the placebo group 84.6 ± 3.4% vs 65.1 ± 4.8% (p = 0.001).18
Importantly, it appears that there is no long term mortality/morbidity benefit of corticosteroid in patients with AH. Initial studies demonstrated continued survival benefit for up to 6 months after treatment with corticosteroids.23 Additional follow-up of these patients revealed that the survival benefit of corticosteroid therapy persisted for one, but not two years after treatment.23,24 There were no major complications associated with corticosteroid therapy in these studies, but patients were highly selected.
For more than two decades, the Maddrey Discriminant Function (DF) [4.6 (prothrombin time prolongation (seconds) - control value (seconds) + bilirubin (mg/dL)] has been used to stratify patients at high risk for short term mortality that may benefit from corticosteroid therapy.5 Patients with DF of ***entity***32 have an extremely poor prognosis, with 1 month mortality rates of 40-50%. In contrast, patients with lower DF values have short term survival rates of 90-100%. More recently, studies from France reported that an early decline in serum bilirubin at day 7 of treatment [early change in bilirubin levels (ECBL)] is a strong prognostic factor for response to corticosteroids and higher survival rate at 6 months after treatment.25 In a cohort of 238 patients with DF ***entity***32, 73% (153/209) of patients at day 7 on prednisone 40 mg/ day or intravenous infusion of methylprednisone 32 mg/ day showed a decrease in bilirubin levels (4.94 ± 4.40 mg/dL). After 28 days of corticosteroid treatment, 93% of these patients had improved liver function, and 96% survived as compared to 59% survival in patients without ECBL; moreover at 6 months, survival of patients with ECBL was 82.8% ± 3.3 % vs 23% ± 5.8% in patients without ECBL. Hozo and colleagues had noted similar improvement in bilirubin level with shorter hospital stay in a group of patients with alcoholic liver cirrhosis and refractory hyperbilirubinemia when treated with methyl- prednisolone (1 mg/kg/day i.m. over 3 days).26
In summary, glucocorticoids may be useful in the treatment of severe alcoholic hepatitis with DF ***entity***32 or hepatic encephalopathy but should not be used in patients with gastrointestinal bleeding requiring transfusion, active infection and probably in hepatorenal syndrome. Patients should be monitored to determine whether they have a drop in their bilirubin by day 7 (if no decrease, stop steroids). Steroids have well documented side effects, including enhancing the risk of infection which is already substantial in patients with alcoholic hepatitis, and may not be effective for hepatorenal syndrome. Thus, a major disadvantage of glucocorticoids is their lack of applicability in many patients with alcoholic hepatitis.
PentoxifyllinePentoxifylline (PTX) is a nonselective phosphodi- esterase inhibitor which increases intracellular concentrations of adenosine 3’, 5’-cyclic monophosphate (cAMP), and increased cAMP decreases production of proinflammatory chemokines/cytokines such as TNF. Potentially beneficial effects of pentoxifylline include downregulation of chemokine/cytokine (TNF-***entity***, IL-8, MCP-1, macrophage inflammatory protein [MIP] - 1***entity***) synthesis, decreased expression of adhesion molecules, decreased neutrophil activation, inhibition of lymphocyte and monocyte proliferation and decreased leukocyte transmigration.27 Pentoxifylline has attenuated liver injury and fibrosis in several animal models of liver disease.28 A major research focus of our laboratory has been the role of TNF-***entity*** nn ALD.29 We previously reported that monocytes from alcoholic patients show enhanced constitutive as well as LPS-inducible NF-• B activation and TNF-***entity***production.29,30 Studies in monocytes have shown that cAMP plays an important role in regulating TNF-***entity*** expression, and elevation of cellular cAMP suppresses TNF-a production. We recently showed that chronic etha- nol exposure significantly decreased cellular cAMP levels in both LPS stimulated and un-stimulated monocytes.31 Consistent with the decrease in cAMP levels, ethanol led to an increase in LPS-inducible TNF-***entity***production by affecting NF-***entity***B activation and induction of TNF mRNA expression. Enhancement of cellular cAMP with dibutyryl cyclic AMP (dbcAMP) abrogated LPS mediated TNF-***entity***expression in ethanol treated cells. Our recent research strongly suggests that ethanol can synergize with LPS to up-regulate the induction of TNF gene expression and consequent TNF overproduction by decreasing the cellular cAMP levels in monocytes/macrophages. These data further support the notion that cAMP elevating agents could constitute an effective therapeutic approach in attenuating or preventing the progression of liver disease in alcoholic patients.
Akriviadis and colleagues performed a prospective, randomized, double blind clinical trial of pentoxifylline in severe alcoholic hepatitis patients with DF ***entity***32.32 Forty-nine patients received 400 mg of PTX orally three times daily and 52 received placebo (Vitamin B12) for four weeks. PTX treatment improved survival. 12 patients (24.5%) on PTX died compared to 24 patients (46%) on placebo. PTX also decreased the risk of hepatorenal syndrome as a cause of death. Six of the 12 (50%) PTX-treated patients who died did so of renal failure while 22 of 24 (92%) deaths in the placebo group were from renal failure. Multivariate analysis revealed age, serum creatinine at randomization, and treatment with PTX as independent factors associated with survival. Due to its excellent safety profile, anti-inflammatory properties and protective effect against hepatorenal syndrome based on the trial noted above, PTX appears to be a viable alternative to corticosteroid therapy in ALD. Our group routinely uses PTX (400 mg orally three times daily) not only in patients with alcoholic hepatitis but also in patients with alcoholic cirrhosis.
Anti-TNF therapyCytokine dysregulation is central to the pathogenesis of ALD and was described in alcoholic hepatitis long before it was recognized in inflammatory bowel disease and rheumatoid arthritis. Anti-TNF therapy has been a highly effective, FDA approved treatment for IBD and RA for several years, but its role in ALD is yet to be clarified. Dysregulated TNF***entity*** metabolism has been well documented in ALD through cell culture experiments was well as animal and human studies.29-31 In fact the late Ron Thurman’s laboratory has successfully shown that liver injury in alcohol-fed rats can be blocked using anti-TNF-***entity*** antibody.33 An initial concern about using anti-TNF antibody in humans arose from the observation that low ‘basal’ levels of TNF-***entity***are needed for liver regeneration.34 Hence, many investigators approached the problem by attempting to down-regulate TNF activity rather than completely blocking it. Indeed, many therapies used in ALD (glucocorticoids, PTX, S-adenosylmethionine, etc.) decrease but do not abolish TNF activity. Tilg and co-workers in Europe, carried out a small clinical trial involving 12 patients with moderate to severe alcoholic hepatitis who were given Infliximab (anti-TNF antibody) 5 mg/kg as a single 2-hour infusion. Ten of the 12 patients were alive at a median of 15 months.35 Pilot data from a small US open-label trial of etanercept (recombinant soluble TNF receptor), also showed safety in patients with less severe AH, and a multicenter trial studying this agent is being funded by the National Institutes of Health.36 On the other hand, a large double-blind randomized trial from France using either prednisone treatment or prednisone treatment plus high-dose Infliximab in patients with acute AH was terminated due to increased infectious complications in the combined therapy group.37 Thus, etanercept may be more appropriate in ALD than Infliximab because of its shorter duration of action. However, increased risk of infection and impaired liver regeneration continue to be a theoretical concern when completely blocking TNF activity over a long duration. Furthermore, whether anti-TNF antibody therapy has any role in alcoholic cirrhosis (separate from alcoholic hepatitis) remains to be determined. Until more data are available, specific anti-TNF therapy should optimally be performed only in the context of a clinical trial.
Drugs with unlikely benefitPropylthiouracilChronic alcohol feeding in animals models can induce a hypermetabolic state with increased oxygen consumption, and relative hepatic hypoxia, especially in the centrilobular area of the liver. Propylthiouracil has been postulated to attenuate this hypermetabolic state, to function as an antioxidant, and to improve portal blood flow. However, a recent Cochrane review of six randomized trials of over 700 patients in which propylthiouracil therapy was evaluated in patients with alcoholic liver disease, showed no benefit.38
Polyenylphosphatidylcholine (Lecithin)Polyenylphosphatidylcholine, or lecithin, is a lipid extract from soybeans. It prevents fibrosis in alcohol fed baboons, stimulates the release of collagenase activity by cultured hepatic stellate cells, has antioxidant effects, and decreases TNF production.39,40 Multiple positive studies of polyenylphosphatidylcholine in animal models of liver disease led to a VA Cooperative Study, which evaluated the effects of this drug in humans with alcoholic liver disease.41 This study showed no significant benefit, but patients decreased their alcohol use during the trial, making a beneficial effect of polyenylphosphatidylcholine more difficult to determine. Another negative aspect of this agent is the multiple large pills that must be consumed, making compliance difficult.
ColchicineColchicine has many potential therapeutic mechanisms of action including inhibition of collagen production, enhancement of collagenase activity, and anti-inflammatory functions.42 Unfortunately, a large VA Cooperative Study of colchicine therapy in patients with alcoholic cirrhosis which showed no beneficial effects on either overall mortality or liver related mortality.43
Anabolic steroidsAnabolic steroids decrease fatty infiltration in the liver and may be hepatoprotective. Patients with end stage liver disease frequently have malnutrition and have low levels of the anabolic hormone, insulin-like growth factor-1. Based on these findings, a large VA Cooperative Study was performed which generally demonstrated no significant benefit.44 A recent Cochrane review also was not able to document efficacy for this therapy in patients with alcoholic liver disease, but the drug did appear to be safe.45 It is important to note that the correct study design for this agent has not been employed: anabolic hormone therapy plus enforced enteral nutrition.
CAM Agents/nutritional supplementsSilymarinSilymarin, the active ingredient extracted from Silybium marianum (also known as milk thistle) has been shown in experimental animals to protect against multiple hepatotoxins including carbon tetrachloride, acetaminophen, and iron overload and mushroom poisoning.46 It has antioxidant properties, protects against lipid peroxidation, and has antiinflammatory and anti-fibrotic effects. Large controlled trials of Silymarin have been performed in Europe, with varying results. Ferenci and co-workers evaluated 170 patients with cirrhosis in a treatment program 40 mg silymarin t.i.d. with a mean duration of 41 months. They observed a positive beneficial effect, especially in patients with alcoholic cirrhosis and in those with milder disease (CTP A disease).47 On the other hand, Pares, et al. found no beneficial effects of 150 mg silymarin t.i.d. in 200 patients with alcoholic cirrhosis, some of whom also had hepatitis C.48 In spite of inconsistent results, silymarin has become the most popular form of complementary and alternative medicine therapy for liver disease because it has a good safety profile. Results from large multicenter studies of silymarin in Hepatitis C and NASH should provide insights into the effectiveness of this agent in liver fibrosis.
S-adenosylmethionine/BetaineAbnormal methionine metabolism is well documented in ALD, with patients frequently having elevated plasma methionine concentrations and regularly having decreased clearance of intravenously or orally administered methionine. Methionine adenosyltransferase (MAT), the enzyme that is responsible for the initial conversion of methionine to S-adenosylmethionine (SAM), is decreased in ALD, and SAM levels also are decreased.49 Studies from Spain have shown that oxidative stress and depletion of glutathione play a role in MAT inactivation.50 Hepatic hypoxia can also cause a decrease in MAT activity.51 Both oxidative stress and hepatic hypoxia are prominent features of ALD and may contribute to the observed low MAT activity. SAM has been reported to protect against a variety of forms of experimental liver injury including that caused by alcohol, acetaminophen, carbon tetrachloride, galactosamine, and others.52,53 SAM has multiple theoretic benefits in ALD including antioxidant properties, serving as a critical methyl donor, maintaining mitochondrial function, decreasing TNF, playing a role in glutathionine production, and others. A multicenter clinical study from Mato’s group reported that SAM supplementation (1200 mg) significantly improved mortality and decreased need for liver transplantation in ALD.54 SAM also has been used in other clinical liver diseases in Europe (especially cholestatic liver disease), and it appears to have a very good safety profile.
Betaine (trimethylglycine) was initially discovered in the juice of sugar beets. Betaine functions as an organic osmolyte to protect cells from stress, and it also functions as a major methyl donor in the methionine cycle figure 2.55 Thus, it is appropriate to discuss SAM and betaine together. In the transmethylation pathway, SAM is converted to S-adenosylhomocysteine (SAH). While SAM levels tend to be low in most forms of liver disease, SAH levels are elevated, as are homocysteine levels.56 SAH can sensitize hepatocytes to TNF-induced hepatotoxicity, and homocysteine is a major inducer of fatty liver.56 Thus, it is important to be able to remove excess levels of both SAH and homocysteine from the liver. Betaine facilitates the conversion of homocysteine back to methionine and helps remove both SAH and homocysteine (Figure 2). Animals injected with betaine demonstrate a dose-dependent increase in red blood cell SAM, again documenting the potential overlapping roles of SAM and betaine in therapy of different forms of liver disease.
 and homocysteine are increased. Homocysteine can be recycled back to methionine or ultimately converted to the antioxidant glutathione. A buildup of homocysteine is thought to cause fatty liver, and a buildup of SAH sensitizes to TNF killing.")
There are marked alterations in methionine metabolism in ALD. The first product of methionine metabolism, S-adenosylmethionine - SAM - is decreased whereas S-adenosylhomocysteine (SAH) and homocysteine are increased. Homocysteine can be recycled back to methionine or ultimately converted to the antioxidant glutathione. A buildup of homocysteine is thought to cause fatty liver, and a buildup of SAH sensitizes to TNF killing.
Betaine is known to be protective against a variety of forms of experimental hepatotoxicity such as those induced by endotoxin, carbon-tetrachloride, chloroform, alcohol and others.57-58 As noted previously, low levels of SAM are observed in most forms of liver disease and SAM serves as a hepatoprotective agent. Betaine functions by removing SAH and homocysteine from the liver, as well as regenerating SAM. While betaine is highly effective in animal models of ALD, no large human trials have been reported. It is also important to note that while there is substantial scientific support for the use of SAM in ALD, a recent Cochrane report could not support or refute the use of SAM based on current clinical trials.59
AntioxidantsVitamin E deficiency has been well documented in ALD.60 Vitamin E has been shown to have hepatoprotective effects in experimental models of liver injury such as that induced by carbon tetrachloride or ischemia. Vitamin E has multiple potential beneficial effects including membrane stabilization, reduced NFkB activation and TNF production, and inhibition of hepatic stellate cell activation and collagen production.60-63 A randomized study of vitamin E in alcoholic cirrhosis did not show significant benefit. Similarly, a more recent trial of vitamin E in alcoholic hepatitis did not show benefit.64
Glutathione is part of the natural anti-oxidant system of the cell. It is a tripeptide consisting of glutamate, cysteine and glycine. It is synthesized in the cytoplasm and transported in to the mitochondria where it plays a pivotal role as an anti-oxidant.65,66 Glutathione prodrugs have produced beneficial effects in virtually every known experimental model of hepatotoxicity.65 Glutathione prodrug N-acetylcysteine (NAC) is the gold standard in the treatment of acute acetaminophen poisoning. Glutathione prodrugs also have been shown to inhibit TNF, IL-6 and IL-8 in alcoholic cirrhosis.66 However, large randomized studies of glutathione prodrugs with death as an outcome have not been performed in patients with ALD.
As noted previously, a recent trial of multiple antioxidants versus steroids in AH demonstrated benefit in the steroid group.22 It is important to note that in no human antioxidant study has an “antioxidant effect” been documented. Thus, it is important for future antioxidant studies to confirm that the antioxidant given has an in vivo antioxidant effect.
ZincZinc deficiency was documented in alcoholic liver disease approximately a half-century ago with the observation that patients with severe alcoholic cirrhosis had marked hypozincemia. Hypozincemia has subsequently been confirmed by multiple investigators, as has decreased tissue stores of zinc. Moreover, rats fed alcohol in their water supply and rats with experimentally-induced liver injury also have depressed plasma and tissue zinc concentrations.67,68
The mechanisms for zinc deficiency in alcoholic liver disease are multiple. Dietary zinc intake is often depressed, with alcohol frequently making up over 50% of caloric intake (with alcohol being devoid of zinc). There is usually a direct correlation between protein intake and zinc intake in humans, and protein intake is often depressed in alcoholic cirrhotics. Patients with alcoholic liver disease may have impaired zinc absorption. This is somewhat of a paradoxical situation in that zinc deficiency normally is associated with enhanced zinc absorption. Patients not only have decreased absorption of zinc but they have increased urinary excretion of zinc. While renal excretion is normally a minor route of zinc loss (usually less than 500 mcg/24 hours), patients with liver disease may lose 1-4 mg zinc per day in their urine. Albumin from decompensated cirrhotics has less affinity for zinc than albumin from normal subjects. This could influence plasma-zinc concentration, the amount of ultrafilterable zinc available to the kidney, and the bio-availability and tissue distribution of zinc. Lastly, cytokines such as tumor necrosis factor and interleukin-6, which are elevated in alcoholic liver disease, may induce an internal redistribution of zinc and play a role in the low plasma/serum zinc levels seen in alcoholic liver disease.
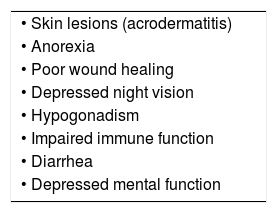
The zinc deficiency/altered zinc status observed in alcoholic liver disease may lead to many metabolic abnormalities (Table I). Early studies have documented that zinc supplementation will reverse these zinc deficiency signs and symptoms. More recent studies in animals show that zinc protects against ALD by multiple mechanisms including stabilization of gut barrier function, decreasing endotoxemia, decreasing TNF, decreasing oxidative stress and others.69,70 We regularly give zinc 220 mg/day of zinc (sulfate) to our patients with ALD, as it corrects a nutritional deficiency and may improve their liver disease.
Liver transplantationCurrently, ALD ranks In a recent study, Gottardi reported.71,72 Overall only 5% of alcoholic cirrhotics receive a liver transplant.73 This fact illustrates the complexity of evaluating and transplanting these patients. Since Starzl’s 1988 report of 68% survival at 3 years in this patient population, ALD has accounted for 10 to 20% of all liver transplants in the US.74,75
Liver transplantation in alcoholic cirrhotics remains a highly controversial and sensitive issue. With the growing disparity between organ donors and those awaiting transplantation, the judicious use of the scarce resource has become imperative. The philosophical basis for selection is utilitarian i.e. dependent on likely outcome rather than on right to an organ or personal responsibility.76 Convincing an already skeptic public, which views alcoholism as a ‘self inflicted ailment’, that transplanting patients with alcoholic cirrhosis is worthwhile is no easy task. Despite the variation in selection criteria amongst the different centers, it has been conclusively shown that the outcome of liver transplantation in alcoholic cirrhosis is equivalent to those transplanted for other indications.77
Pre-operative evaluationAlcohol abuse leads to impairment of cerebral and cardiac function in addition to cirrhosis. These patients also have significant psychosocial co-morbidities. An extensive evaluation is needed to optimize these conditions. The timing of transplantation seems important in these patients. Poynard has shown that when transplanted with a Child’s score of 11 or greater these patients have an improved 5 year survival.78 In this study there was no benefit in transplanting when the score was less than 11. Active alcohol abuse and alcoholic hepatitis are contraindications to liver transplantation.79
Alcohol is thought to have direct depressant effect on the myocardium and may result in dilated cardiomyopathy.80 Additionally, myofibroblastic proliferation of mitral valve chordae tendinaeae has been described in Laennec’s cirrhosis. These factors mandate a thorough cardiac evaluation in these patients prior to transplantation. Cirrhotics have a high prevalence of global brain dysfunction manifesting as cognitive deficits and a wide range of neuropsy-chiatric symptoms including movement disorders, mood and anxiety disorders and circadian disturbances. Miller showed that alcoholics had a lower score on the Raven’s progressive matrices test and Walton established a correlation between the number of years of alcohol consumption and digit test results.81,82 More recent studies have, however, suggested no differences in cognitive dysfunction between alcohol and other etiologies.83
A period of alcohol abstinence is considered essential before these patients can be listed for liver transplantation. This serves two purposes. By allowing the liver and non-hepatic co-morbidities to recover, it improves the fitness of the patients. This measure often improves liver function so as to obviate or postpone the need for a transplant. The second important benefit is that it provides reassurance to the public that donated organs are being used with appropriate care. Although most centers use the “6 month rule” of abstinence as a pre-requisite for listing alcoholic cirrhotics, there are other important factors such as social stability, alcohol problems in partner or first degree relatives, repeated alcohol treatment failures, compliance with medical care, polydrug abuse, coexisting psychiatric disorder and lack of insight about diagnosis.84 These factors have been shown to have a major impact on relapse after liver transplantation.
Post-operative careOwing to the preoperative debilitated state, alcoholic cirrhotics often need longer ICU stay and a longer stay in rehabilitation facilities. There is scant evidence, however, that these patients have increased post-operative complications or consume greater resources.
A recent cost analysis from France concluded that the post-transplant hospital stay depended on the severity of liver dysfunction rather than etiology. This study however, did show that the need for consultation with other specialists was higher in alcoholic cirrhotics.85
Long term resultsThe 7 year survival rate after liver transplant for alcohol-induced liver disease has been reported as 60%, comparable to the rates for primary biliary cirrhosis (76%) and chronic hepatitis C (57%).72
There have been numerous studies on alcohol recidivism following liver transplantation. There is a wide variation (12-95%) in the reported relapse rates largely due to the criteria used to define relapse – any drinking versus problem drinking.86,87 Graft dysfunction secondary to relapse is uncommon (0 – 17%) and mortality is rare (0.5%).86,88 In a recent study, Gottardi reported a 11.9% relapse rate of harmful alcohol consumption. Factors associated with relapse were a pre-transplant abstinence of less than 6 months, psychiatric co-morbidities and a HRAR (High Risk Alcohol Relapse) score of greater than 3.89
Reintegration into society to lead active and productive lives is equivalent in alcohol-related and non-alcohol related liver transplant recipients. However, alcohol related recipients were less likely to be involved in structured social activities and routine volunteer work than non-alcohol related liver recipients.90 One of the other main concerns on long term follow-up of liver transplant recipients is the development of de novo cancers. An increased incidence of malignancies, particularly aero-digestive cancers (esophageal and lung), has been documented in alcohol-related liver transplant recipients. A significant decline in survival rates after 10 years has been linked to cancers – a greater cause of morbidity and mortality than recurrent alcoholism.91 This is related to the combined alcohol and tobacco exposure both before and after transplantation. Males seem to be more prone to develop these lesions. Hence pre-transplant cessation of both smoking and alcohol as early as possible is to be obtained. Additionally, yearly upper gastrointestinal endoscopy with lugol coloration, pharyngolaryngeal examination and chest X-rays have been suggested as surveillance measures.91
ConclusionsThe optimal management of ALD begins with therapeutic lifestyle changes, in which abstinence or dramatic reduction in alcohol use is crucial. Towards this goal, «brief interventions» carried out by the patient’s nurse, primary care physician or gastroenterologist can often be successful. Abstinence has a profound beneficial effect on survival at all stages of the disease. The next step is to eliminate other factors that enhance disease progression such as cigarette smoking and obesity or inappropriate drug use (e.g., excess acetaminophen). If the patient has other liver diseases such as iron overload or Hepatitis C, then treating them, if feasible, becomes an important step in management.
For patients who present with alcoholic hepatitis, the importance of starting enteral nutrition early to ensure adequate protein and caloric intake cannot be overemphasized. In severely ill alcoholic hepatitis patients (DF ***entity***32) or those with hepatic encephalopathy who do not have a significant gastrointestinal bleed or infection, a short course of steroids should be considered. A decrease in bilirubin by the end of 1 week is an important treatment milestone. Pentoxifylline is an excellent alternative to glucocorticoid therapy particularly in patients who are at risk for hepatorenal syndrome (worsening creatinine, infection, hyponatremia).
No drugs with documented efficacy are available for alcoholic cirrhosis. Many patients are already taking milk thistle or SAM, which may be of benefit. Because of the risk of decompensation with superimposed infection, all patients with alcoholic cirrhosis should be vaccinated against hepatitis A, hepatitis B and against influenza annually. Patients with cirrhosis should undergo screening and regular surveillance for hepatocellular carcinoma (ultrasound every six months). This is particularly important for older cirrhotics who have been abstinent for a long time. Finally, liver transplant should be considered in these patients when appropriate, since it has been shown to be very effective in carefully selected patients who have discontinued drinking.



