








The arrival of a new-born baby drastically changes the parents’ lives. Several authors have reached the conclusion that this vital event can even lead to a post-traumatic stress disorder. This fact is especially relevant when it comes to correctly coping with this situation. The role played by the emotions involved in this process as well as the stress suffered by parents experiencing such a change are recognized by previous studies. In this paper, we carried out a comparative study between the emotions and stressful situations experienced by preterm and term babies’ progenitors. The results show how the group of parents of preterm babies is more affected by stress and negative emotions. In this sense, the spectrum widens to an almost unprecedented relevant field in psychological research that allows us to see how the parents of premature children experience this circumstance.
La llegada de un nuevo hijo cambia drásticamente la vida de los padres. Algunos autores han llegado a la conclusión de que estos eventos vitales incluso pueden llegar a producir un trastorno de estrés postraumático. Este hecho es especialmente relevante para afrontar correctamente la situación. Está reconocido el papel que tienen las emociones involucradas en este proceso así como el estrés que sufren los padres que experimentan este cambio. En este trabajo desarrollamos un estudio comparativo entre las emociones y las situaciones de estrés experimentadas en padres con niños que han nacido a término frente a padres de niños que han nacido prematuros. Los resultados muestran cómo el grupo de padres de niños nacidos prematuros sufre más estrés y emociones negativas que el grupo de padres de niños que nacen a término. En este estudio se abre la puerta a un campo relevante casi inédito en la investigación psicológica que nos permite ver cómo los padres de niños prematuros viven esta circunstancia.
The phase of pregnancy is a vital event in people's lives, both for future mothers and also fathers. Therefore, the moment of birth as well as the caring of the baby define a period of crucial change for progenitors. In this sense, emotions reflect what happens to us; they are signs and symptoms which provide feedback concerning the way we confront different situations. The events lived during the perinatal stage (especially during the first hours after birth) bear great relevance in order to understand the process of changes experienced by progenitors of full-term babies. But what about the parents of premature infants? Prematurity increases the biological and psychological risk factors in babies and parents. The study of preterm birth will allow us to observe the psycho-emotional consequences (disorders of early interaction, exercise of parental roles, the ability to cope with stress, amongst others) that are generated by the biological risk factors (neurodevelopmental problems). This will make it possible to design procedures of intervention adapted to the needs of children and parents (Karen, Tyano, & Sirota, 2000).
It is estimated that nearly 15 million premature babies (that is to say, those who are born with less than 37 weeks of gestation) are born in the world each year (Platt, 2014). In 2015, WHO reported that the rate of preterm births fluctuated between 5% and 18% (WHO, 2015). In Europe, this rate varies between 5% and 11% depending on the country (Zeitlin, Mohangoo, & Delnor, 2010). According to the National Institute of Statistics (Instituto Nacional de Estadística, INE), each year during the last decade, more than 30,000 children were born prematurely in Spain and more than 1000 of them in the Canary Islands. This represented 6.5% and 6.8% of the population, respectively in 2014 (INE, 2014). There is broad consensus that, at birth, age is more important than the weight, because the former is what really determines the maturity of the major organs. The immature child has a greater risk of not successfully completing the process of adaptation to external and autonomous life, so this critical phase can have medical and psychological sequelae for the rest of the baby's life (Horbar et al., 2002).
The emotional situation of preterm babies’ parents is subject to high levels of uncertainty and ambiguity. In a couple of hours, the preterm baby's situation can change, whether with a positive or tragic end, or it can continue in an imprecise and uncertain way. How do parents react to this experience of uncertainty, stress and fear? Is it advisable to proceed with a professional psychological plan? How should this plan deal with this situation? Currently, there is little empirical evidence that helps to answer these questions.
Psychological stress is considered as “a particular relationship between the person and environment that is appraised by the person as taxing or exceeding his or her resources and endangering his or her well being” (Lazarus & Folkman, 1984). When a person considers that he/she does not have enough resources to face the situation, his/her well-being can be negatively affected. Also, if this psychological tension is not dispelled appropriately, it can lead to mental diseases related to anxiety and depression (Boullosa, 2004). Besides, it is likely that the birth of a baby (especially when it is a preterm birth) increases the stress levels and the negative emotional status of the parents, thus making the development of a post-traumatic stress disorder possible (Pierrehumbert, Nicole, Muller-Nix, Forcada-Guex, & Ansermet, 2003). Probably, the adequate management of these stressful events can help to create a more adapted and healthy management of the situation.
Finally, Plutchik's evolutionary theory of emotions contributes with a complementary conceptual frame to this quandary. In the case of premature births, it appears that interactive behaviors are worthy of particular attention, and their origin depends on multiple factors. The emotional suffering of parents, especially the mother's suffering, has been attributed to the immaturity of the premature infant, as well as the early separation of the child from the parents (Crnic, Ragozin, Greenberg, Robinson, & Basham, 1983; Miles & Holditch-Davis, 1997; Muller-Nix et al., 2004). There are studies comparing the behavior of preterm infants’ mothers with that of mothers with healthy children born at term. The former are presented as more active, more vigilant and less sensitive to answer inadequately to certain baby's necessities (take longer to perceive and respond to the baby's physical and emotional alterations) (Joo, Choi, Rha, Kwak, & Park, 2015; Muller-Nix et al., 2004; Wijnroks, 1999).
The main aim of this study is to compare the levels of stress and the emotional state between the parents of premature babies and parents of infants born at term. This comparison is made in two different instances; firstly during the first days of the baby's life (12–72h) and finally after 6 living weeks. This will allow us to recognize the evolution in both groups.
More specifically, what this paper is trying to detect is whether there is a higher rate of positive emotions instead of negative ones in the group of parents of full-term neonates, as compared to the preterm one, and whether these differences are still present with the passing of time. Also whether there are any existing differences between the stress perceived by the preterm group in opposition to the full-term group, both in the first and second phase (first hours against 6 weeks).
MethodSampleThe sample is made up of 54 parents who have been looked after at the University Hospital of the Canaries (Complejo Hospitalario Universitario de Canarias – CHUC) from June 2012 to March 2013. Women represent 74% of the total sample whereas men represent 26%. There are two different groups, parents of preterm babies and parents of full-term babies who participate voluntarily. The latter is made up of 30 participants with an average age of 29.96 years old, while the group of preterm neonates’ parents is made up of 24 participants with an average age of 32.52 years old (approximately a 5% of the whole population of preterm babies’ parents at the province of Santa Cruz de Tenerife).
InstrumentsThroughout the development of this work, we have used two paper-and-pencil questionnaires:
The Perceived Stress Scale (PSS: Cohen, Kamarck, & Mermelstein, 1983). In this case, a scale of 14 items has been employed and adapted to the Spanish population with an internal consistency of .81 (alpha coefficient) and a test-retest reliability of .73. Remor (2006) informs of the meaningful correlations (Pearson) between the scale of distress (.71) and anxiety (.64).
The Scale of Positive and Negative Affects (PANAS; Watson, Clark, & Tellengue, 1988). It is divided into two sub-scales: the positive affect (PA) and the negative affect (NA), each of them with 10 items. What the authors seek is the purest affect descriptors. The reliability for the NA and PA scales, estimated through alpha coefficients, was .89 for men and .87 for women in the PA subscale, while the corresponding alpha in the case of NA subscale was .91 for men and .89 for women (Sandín et al., 1999).
ProcedureThe recruitment of participants was carried out in the University Hospital of Tenerife. The sample of full-term babies’ parents came from the gynecology area. A group of collaborators visited the rooms where mothers were hospitalized and the latter were offered the possibility of participating together with their partners. The same procedure was carried out at the Neonatal Intensive Care Unit (NICU) with parents of preterm babies. Once the purpose of the research was explained and participation was accepted, parents filled in the questionnaires. A brief interview then served to collect useful data. The same steps were followed 6 weeks later either in person or via telephone, to gather full data of all participants.
ResultsData analysisBoth groups in the two aforementioned stages, both in the field of emotions and perceived stress, were compared. For the data analysis, statistical language R through an ULLRToolbox tool was used (Hernández & Betancort, 2014).
Comparison of positive and negative affects in the PANAS scaleIn order to expose PANAS scores, T-test contrasts were used, both in the first moment (birth) as well as in the second one (6 weeks later). Furthermore, the results of the two groups as well as their mean, standard deviations in each moment and the effect sizes are presented (Tables 1 and 2).
The PA scores do not show any significant mean difference between groups, while NA scores manifest significant differences between them, both in the first stage (p<.01) as well as in the second one (p<.01). In both cases, the group of preterm babies’ parents has a significantly higher average than the group of full-term babies’ parents, with an effect size of d=.92 and d=.74.
Principal component analysisTaking the previous results into account, a more detailed analysis was conducted to identify the emotional differences and how they were grouped. In order to do so, a principal component analysis (PCA) with varimax rotation was carried out.
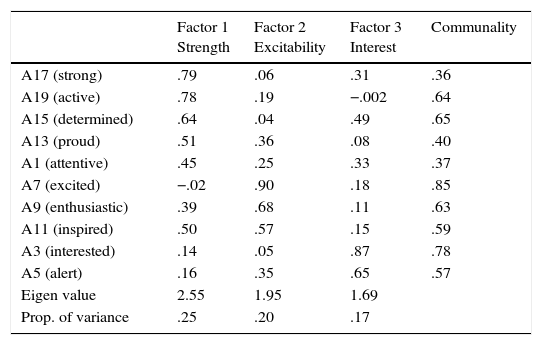
Positive affects subscaleIn Table 3 the results of the PCA are presented. Positive emotions are grouped into three factors. The first one explains 25% of the whole variance and the items with saturations closer or higher to .50 are: “strong”, “active”, “determined”, “proud”, and “attentive”. The second factor explains 20% of the whole variance and the items that saturate above .50 are: “excited”, “enthusiastic” and “inspired”. The last factor explains 17% of the whole variance. Two items saturate over .50: “interested” and “alert”.
Factor scores for positive affect.
| Factor 1 Strength | Factor 2 Excitability | Factor 3 Interest | Communality | |
|---|---|---|---|---|
| A17 (strong) | .79 | .06 | .31 | .36 |
| A19 (active) | .78 | .19 | −.002 | .64 |
| A15 (determined) | .64 | .04 | .49 | .65 |
| A13 (proud) | .51 | .36 | .08 | .40 |
| A1 (attentive) | .45 | .25 | .33 | .37 |
| A7 (excited) | −.02 | .90 | .18 | .85 |
| A9 (enthusiastic) | .39 | .68 | .11 | .63 |
| A11 (inspired) | .50 | .57 | .15 | .59 |
| A3 (interested) | .14 | .05 | .87 | .78 |
| A5 (alert) | .16 | .35 | .65 | .57 |
| Eigen value | 2.55 | 1.95 | 1.69 | |
| Prop. of variance | .25 | .20 | .17 |
These three factors, according to an order of higher saturation, were named: “strength”, “excitability”, and “interest”.
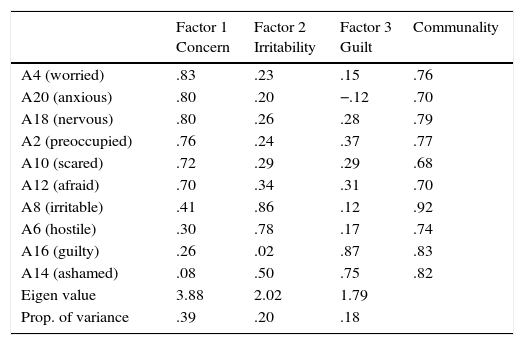
Negative affects subscaleThe results of the PCA for NA items are presented in Table 4. As can be observed, negative emotions are also grouped into 3 factors.
Factor scores for negative affect.
| Factor 1 Concern | Factor 2 Irritability | Factor 3 Guilt | Communality | |
|---|---|---|---|---|
| A4 (worried) | .83 | .23 | .15 | .76 |
| A20 (anxious) | .80 | .20 | −.12 | .70 |
| A18 (nervous) | .80 | .26 | .28 | .79 |
| A2 (preoccupied) | .76 | .24 | .37 | .77 |
| A10 (scared) | .72 | .29 | .29 | .68 |
| A12 (afraid) | .70 | .34 | .31 | .70 |
| A8 (irritable) | .41 | .86 | .12 | .92 |
| A6 (hostile) | .30 | .78 | .17 | .74 |
| A16 (guilty) | .26 | .02 | .87 | .83 |
| A14 (ashamed) | .08 | .50 | .75 | .82 |
| Eigen value | 3.88 | 2.02 | 1.79 | |
| Prop. of variance | .39 | .20 | .18 |
The first factor explains 39% of the whole variance and it contains six elements that saturate over .70 (“worried”, “anxious”, “nervous”, “concerned”, “scared”, and “fearful”). The second factor explains 18% of the whole variance and two factors saturate over .70: “guilty” and “ashamed”. The last factor explains 20% of the whole variance and it also groups two items over .70, more specifically, “irritable” and “hostile”.
These three factors according to the order of saturation as: “concern”, “guilt”, and “irritability”.
Comparisons of the three factors of the sub-scale of positive affects (PANAS)As a result of the factors obtained in the PC analysis, it was considered of interest to compare the average of the two participant groups in those factors, both in the first and second stages, as well as the comparison of both original sub-scales, through a T-test contrast.
In Tables 5 and 6, the factor interest of the PA sub-scale manifests meaningful differences between both groups at both moments (size of the effect of d=.65 and d=.25). The excitability factor presents marginally significant differences (p<.07 in moment 1 and p<.12 in moment 2), with moderated effect sizes (d=.50 and d=.42). The mean of preterm neonates’ parents shows a lower value than that of the full-term neonates’ parents, in both stages.
Means and standard deviations of positive affect factors at birth moment.
| Phase 1 (birth) | Preterm | Full-term | t | gl | Effect size | p | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Factor | Mean | SD | Mean | SD | d | 95% CI | ||||
| Strength | 19.92 | 3.53 | 20.06 | 3.56 | −.15 | 59 | −.4 | −.58 | .50 | .88 |
| Excitability | 10.60 | 3.11 | 11.86 | 2.18 | −1.86 | 59 | −.50 | −1.05 | .03 | .07 |
| Interest | 8.76 | 1.33 | 7.83 | 1.60 | 2.37 | 60 | .65 | .10 | 1.20 | .02 |
Means and standard deviations of positive affect factors 6 weeks after birth moment.
| Phase 2 (6 weeks) | Preterm | Full-term | t | gl | Effect size | p | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Factor | Mean | SD | Mean | SD | d | 95% CI | ||||
| Strength | 20.40 | 3.84 | 21.41 | 2.20 | −1.10 | 31.28 | −.30 | −.08 | .24 | .24 |
| Excitability | 10.48 | 3.72 | 11.77 | 2.27 | −1.56 | 51 | −.42 | −.97 | .11 | .12 |
| Interest | 8.42 | 1.89 | 7.97 | 1.65 | .93 | 52 | .25 | −.28 | .79 | .04 |
As with PA, the means of NA using T-test contrasts were compared.
The comparisons for negative emotions are presented in Tables 7 and 8. In the concern factor there are significant differences between the average of both groups (p<.001 in the first stages and p<.01 in the second one) with a robust size of the effect (d=1.03 and ct=−.74). The guilt factor does not arise any significant statistical differences in stage 1, but it does in stage 2 (d=.64). On its behalf, the factor irritability obtains a slightly significant difference in the first moment with a moderated size of effect (c1=−.49).
Means and standard deviations of negative affect factors at birth moment.
| Phase 1 (birth) | Preterm | Full-term | t | gl | Effect size | p | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Factor | Mean | SD | Mean | SD | d | 95% CI | ||||
| Concern | 23.52 | 6.34 | 18.06 | 5.06 | 3.74 | 59 | 1.02 | .45 | 1.59 | .009 |
| Guilt | 5.04 | 2.72 | 4.69 | 2.21 | .55 | 58 | .15 | −.39 | .69 | .57 |
| Irritability | 2.60 | 1.26 | 2.14 | .69 | 1.80 | 58 | .49 | −.05 | 1.04 | .08 |
Means and standard deviations of negative affect factors 6 weeks after birth moment.
| Phase 2 (6 weeks) | Preterm | Full-term | t | gl | Effect size | p | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Factor | Mean | SD | Mean | SD | d | 95% CI | ||||
| Concern | 20.21 | 7.96 | 15.07 | 6.07 | 2.69 | 52 | .74 | .18 | 1.29 | .009 |
| Guilt | 5.79 | 2.86 | 4.20 | 2.14 | 2.34 | 52 | .64 | .09 | 1.19 | .02 |
| Irritability | 2.79 | 1.25 | 2.53 | 1.17 | .78 | 52 | .21 | −.32 | .75 | .44 |
The results of comparing the two groups (full-term and preterm) at both moments (birth and 6 weeks) in terms of perceived stress are presented.
As can be seen in Table 9, mean comparisons in both groups through T-tests contrasts show differences that are statistically significant in the two groups and circumstances (with size effect magnitudes between medium and large). At both moments, the average of the group of parents of preterm babies is higher than that of full-term babies’ parents, with size effects of d=.83 in the first stage and d=.64 in the second one.
DiscussionIn this research, emotions and perceived stress of both groups of parents have been analyzed and compared. The results reveal that there are differences between parents whose babies are born full-term and parents of preterm babies. These differences tend to put the second group at a level of higher psychological distress than the parents whose babies are within the expected gestation period.
More specifically, in terms of positive emotions (excitability and strength), differences are not that noticeable, but there seems to be a tendency in positive emotions to be fewer in parents of preterm babies than in parents of full-term babies. The Interest factor behaves differently as compared to the other two factors: the group of parents of preterm neonates obtains a significantly higher average both in the series of evidences compiled during moments close to the birth of the baby as well as in the ones obtained after 6 weeks. This may be due to the item “alert” since those parents experiment a state of this kind because their baby is hospitalized and in a delicate health situation. It does not occur with full-term neonates.
Concerning negative emotions, differences are found between the group of parents of full-term neonates and preterm neonates indicating that the latter is the one which experiments more negative emotions. Emotions related with concern (anxiety, anguish, nervousness) and guilt at 6 weeks have a higher rate in parents of preterm babies than in those parents of full-term babies.
In relation to the perceived stress, higher levels at both stages in the group of parents of preterm neonates in contrast with the levels of parents of full-term babies were verified. This difference indicates that the birth of a preterm child is experienced by the parents as a stressful event. This perception is kept during the next 6 weeks after the birth and under determined conditions it could evolve into post-traumatic stress disorder. Probably, these results justify the development of psychological intervention programs as a prevention tool in order to slow down the emotional impact and the stress perceived by the parents of preterm babies. The training of doctors, nurses and health psychologists in these areas could aid parents in receiving the information that their babies are premature in a healthier way. So, informing parents and giving them emotional control tools could avoid disturbances of this kind and, also, help them to cope with parenting in the best psychological conditions possible.
Finally, it would be interesting to explore in future works whether there are any differences regarding the participants’ gender. The high participation of mothers against the low participation of fathers can be a first indirect datum of implication. However, it is not enough if we want to go deeper into possible differences between men and women when living the experience of having a preterm child. These results will help to elaborate intervention programs with parents experiencing the stressful life of having a preterm baby.
Conflict of interestThe authors declare that they have no conflict of interest.