

This study was designed to check the psychometric properties of an online Catalan version of the Type D Personality Scale-14 (DS14). Participants were 600 subjects including university professors, service and administrative personnel (n=419) and students (n=181); in total 196 men (32.7%) and 404 women (67.3%) with a mean age of 36.99 (SD=12.76). The sample was randomly split in two groups: calibration and validation. The structural validity was analyzed in the calibration group (n=311) using exploratory factor analysis with oblique and orthogonal rotation procedures, showing two robust factor structure, corresponding to Negative Affectivity (NA) and Social Inhibition (SI). No differences were found comparing the two rotation methods. Confirmatory factor analysis was performed in the validation group (n=289) and the two factor model was replicated, showing satisfactory goodness-of-fit indices as χ2/df=2.40, RMSEA=0.07, SRMR=0.06, GFI=0.92, TLI=0.93, CFI=0.93 and IFI=0.94. The re-specified model correlating the error terms of four pairs of items mildly improved goodness-of-fit indexes. The Catalan DS14 obtained a satisfactory internal consistency for its two subscales NA and SI (Cronbach's alpha=0.85/0.88), and demonstrates good psychometric properties, being a suitable instrument for use in research in the Catalan population.
El objetivo de este estudio fue explorar las propiedades psicométricas de la versión catalana de la Escala de Personalidad tipo D-14 (DS14) mediante una versión on-line. Los participantes fueron 600 sujetos incluyendo profesores, personal administrativo y de servicio (n=419) y estudiantes (n=181) de la universidad. En total 196 varones (32,7%) y 404 mujeres (67,3%) con una edad media de 36,99 (DT=12,76). La muestra se dividió aleatoriamente en 2 grupos: calibración y validación. La validez estructural se analizó en el grupo de calibración (n=311) utilizando un análisis factorial exploratorio y rotación oblicua y ortogonal mostrando la estructura de 2 factores correspondiente a la afectividad negativa (NA) y a la inhibición social (SI). No se encontraron diferencias comparando los métodos de rotación. El análisis factorial confirmatorio se realizó en el grupo de validación (n=289), y el modelo de 2 factores se replicó, mostrando valores satisfactorios usando diferentes índices de bondad de ajuste como χ2/df=2,40; RMSEA=0,07; SRMR=0,06; GFI=0,92; TLI=0,93; CFI=0,93 e IFI=0,94. El modelo re-especificado que correlaciona los términos de error de 4 pares de ítems mejoró ligeramente los índices de bondad de ajuste. La versión catalana DS14 obtiene una consistencia interna satisfactoria para sus 2 subescalas NA y SI (alfa de Cronbach=0,85/0,88). El DS14 catalán demuestra buenas propiedades psicométricas, siendo un instrumento adecuado para su uso en la investigación en la población catalana.
Cardiovascular diseases are the leading cause of death worldwide (Tunstall-Pedoe et al., 1994). Currently, the control of risk factors represents the main strategy to reduce cardiovascular events (Lobos et al., 2009). Psychological risk factors for cardiovascular risk include emotional aspects and personality traits (Krantz & McCeney, 2002). Type D personality (distressed personality type) is a psychological variable typically associated with cardiovascular risk (Pedersen & Denollet, 2006). Besides, Type D personality is a factor of vulnerability in patients with cancer (Batselé et al., 2016), diabetes (Conti, Carrozzino, Patierno, Vitacolonna, & Fulcheri, 2016; Nefs, Pouwer, Pop, & Denollet, 2012), psoriasis (Molina-Leyva, Caparros-Delmoral, Ruiz-Carrascosa, Naranjo-Sintes, & Jimenez-Moleon, 2015) and asthma (Kim et al., 2015). However, Type D personality has also been studied in healthy samples of the general population. (Beutel et al., 2012; Svansdottir et al., 2013).
The Type D personality construct consists of two primary traits: Negative Affectivity and Social Inhibition. Negative Affectivity is considered a tendency to experience negative emotions in everyday circumstances, while Social Inhibition is a tendency to inhibit one's own emotional and behavioral expression in social situations in order to avoid disapproval of others (Denollet, 2000). Pattern D is considered if both scores in Negative Affectivity and Social Inhibition are 10 points or higher. Notice that pattern D is considered a prognostic factor in coronary risk but not an etiologic factor.
Denollet et al. (1996) investigated the relationship between Type D personality with morbidity and mortality in patients with ischemic heart disease. Type D personality was associated with bad disease prognosis regardless of biomedical risks factors. In another study, Type D personality was related with peripheral artery disease, chronic heart failure and arrhythmia (Pedersen & Denollet, 2006). Type D personality has also been suggested as a predictor of clinical outcome and health status after coronary interventions (Denollet, Vaes, & Brutsaert, 2000). In fact, it has been considered as an independent predictor of cardiac events following percutaneous coronary intervention (Pedersen et al., 2004). It is also a good predictor of early allograft rejection after heart transplantation (Denollet, Holmes, Vrints, & Conraads, 2007).
Denollet (1998) developed a Type D personality measure named DS16, also validated in Danish population (Pedersen & Denollet, 2004), and later this instrument was reduced to 14 items and named DS14 (Denollet, 2005). This version was developed and validated in the Dutch and Belgian general population and cardiac and primary health care patients, and showed improvements over its predecessor, such as its brevity and its greater facility to offer scores. Research on DS14 has shown that it is a suitable instrument for use in clinical and epidemiological research (Denollet, Pedersen, Vrints, & Conraads, 2006). DS14 is a rapid and effective screening instrument to optimize risk stratification in patients with cardiovascular disease (Albus, Jordan, & Herrmann-Lingen, 2004).
Since the publication of the original version, many authors have established the validity and reliability of DS14 in different countries and languages, such as Spanish (Montero, Bermúdez, & Rueda, 2017), French (Batselé et al., 2016), German (Grande, Romppel, Glaesmer, Petrowski, & Herrmann-Lingen, 2010), Greek (Christodoulou et al., 2013), Swedish (Conden, Rosenblad, Ekselius, & Aslund, 2014), Norwegian (Bergvik, Sørlie, Wynn, & Sexton, 2010), Icelandic (Svansdottir et al., 2012), Lithuanian (Bunevicius et al., 2013), Slovak (Ďurka & Ruch, 2014), Chinese (Yu, Zhang, & Liu, 2008), Danish (Pedersen & Denollet, 2004), Polish (Ogińska-Bulik & Juczyński, 2009), Ukrainian (Pedersen et al., 2009), Chinese (Weng et al., 2013), Korean (Lim et al., 2011), Hebrew (Zohar, Denollet, Ari, & Cloninger, 2011) or Persian (Bagherian & Ehsan, 2011). Notice that the factorial structure in two factors was analyzed indistinctly with oblique or orthogonal rotations methods. All of them demonstrated similar psychometric properties to the original version, with a two factor-structure and good reliability. One study also compared the DS14 results from 21 countries, confirming the DS14 as a cross-culturally valid construct (Kupper et al., 2013).
The main objective of this research is to adapt and validate the DS14 to the Catalan language and check its psychometric properties for its use in research in healthy and clinical samples, including the factor structure and internal consistency reliability. Our intention was to replicate the factorial structure of DS14 using oblique and orthogonal rotation methods and compare its similarities and differences in a calibration sample, and re-evaluate its structure using a confirmatory factorial analysis (CFA) in a different validation sample.
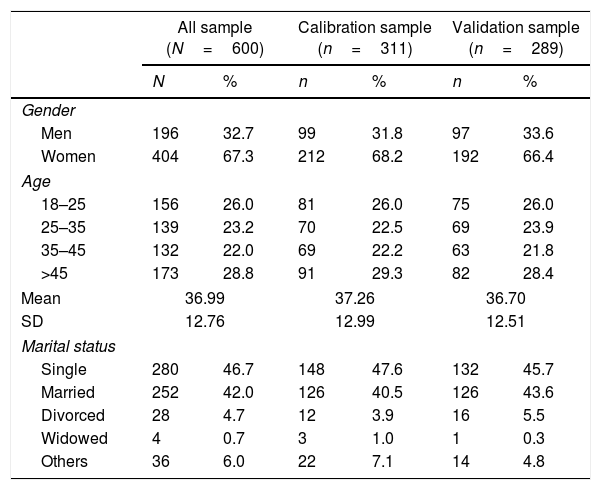
MethodParticipantsThe sample in this study totalled 600 subjects, including professors, service and administrative personnel (n=419), and students (n=181) from the University. The sample was composed of 196 men (32.7%) and 404 women (67.3%) with a mean age of 36.99 (SD=12.76) (range: 18–68). All participants were over 18 years old at the time of the study. The biggest group were single people (46.7%), followed by married people (42%), and divorced and widowed people (4.7% and 0.7% respectively), while other possibilities were not listed (7%). Most of them had University level studies either completed (69.9%), uncompleted (5.8%) or ongoing (13.2%), followed by those with secondary education or vocational training (9%). The remaining (2.2%) had primary education.
InstrumentsThe DS14 has 14 items as a measure of Negative Affectivity (NA) and Social Inhibition (SI), with seven items in each subscale. The seven items of NA cover feelings of dysphoria, worry and irritability, while the seven items of SI cover discomfort, reticence and lack of poise. It is rated on a 5-point Likert scale ranging from 0=false to 4=true with total NA and SI scores ranging from 0 to 28 points. A standard cut-off of ≥10 in both subscales is used to identify individuals with Type D personality. The original version, developed by Denollet (2005), obtained reliability indexes of 0.88 for NA and 0.86 for SI.
For this study, the English version of DS14 was translated into Catalan by our research team and then back translated into English by an independent bilingual professional translator. Discrepancies were consensually resolved through meetings between the translators. Semantic and conceptual equivalence were given priority throughout the adaptation process. The above procedures followed the standard recommendations for adapting questionnaires (Epstein, Santo, & Guillemin, 2015).
ProcedureThe study was carried out in the University of Lleida (Catalonia, Spain). Participants were invited by email to answer DS14 online. All participants were informed before the study and gave informed consent to their participation. Participation was anonymous and disinterested. The academic authorities and the ethics committee authorized this research.
Statistical analysisDemographic characteristics like age, gender and marital status were studied via frequency analysis and descriptive calculation. Differences between demographics were studied using t Student–Fisher, ANOVA or Fisher Chi-square, as appropriate. Means and standard deviations were calculated for items and subscales. Additionally, we calculated skewness and kurtosis values to check for normal distribution of data. Corrected item-total correlations were then calculated. The internal consistency of the subscales and the total scale was calculated by means of Cronbach's alpha.
The sample was segmented using an algorithm that allowed two groups to be divided at random: calibration sample (n=311; 51.8%) and validation sample (n=289; 48.2%). In the calibration sample, the factorial structure was analyzed using principal components analysis. An oblique (Oblimin) and an orthogonal rotation (Varimax) were performed independently. Alternatively, we used Velicer Maps method (Velicer, 1976; Velicer, Eaton, & Fava, 2000) by applying a specific syntax (O’connor, 2000). Both factor extraction methods have been used to retain the factors in the exploratory factor analysis, and this information could be useful to other researches interested in DS14 factor structure.
CFA was performed in a validation sample. Finally, the prevalence of Type D personality was calculated in the total sample, using the standard cut-off (≥10 in both subscales). Statistical analyses were conducted using the SPSS v.23 and AMOS v.24 package.
ResultsDemographic characteristicsTable 1 shows the demographic characteristics used in the study in the full sample. The total sample displays a higher proportion of women than men. There are significant differences in age by gender (t-test=2.652; df=598; p<0.008), men being older than women. There are no significant differences by gender (χ2=0.204, df=1, p<0.651), age (χ2=0.172, df=3, p<0.081), and marital status (χ2=2.140, df=3, p<0.544) between the validation and calibration subsamples.
Socio-demographic variables.
| All sample (N=600) | Calibration sample (n=311) | Validation sample (n=289) | ||||
|---|---|---|---|---|---|---|
| N | % | n | % | n | % | |
| Gender | ||||||
| Men | 196 | 32.7 | 99 | 31.8 | 97 | 33.6 |
| Women | 404 | 67.3 | 212 | 68.2 | 192 | 66.4 |
| Age | ||||||
| 18–25 | 156 | 26.0 | 81 | 26.0 | 75 | 26.0 |
| 25–35 | 139 | 23.2 | 70 | 22.5 | 69 | 23.9 |
| 35–45 | 132 | 22.0 | 69 | 22.2 | 63 | 21.8 |
| >45 | 173 | 28.8 | 91 | 29.3 | 82 | 28.4 |
| Mean | 36.99 | 37.26 | 36.70 | |||
| SD | 12.76 | 12.99 | 12.51 | |||
| Marital status | ||||||
| Single | 280 | 46.7 | 148 | 47.6 | 132 | 45.7 |
| Married | 252 | 42.0 | 126 | 40.5 | 126 | 43.6 |
| Divorced | 28 | 4.7 | 12 | 3.9 | 16 | 5.5 |
| Widowed | 4 | 0.7 | 3 | 1.0 | 1 | 0.3 |
| Others | 36 | 6.0 | 22 | 7.1 | 14 | 4.8 |
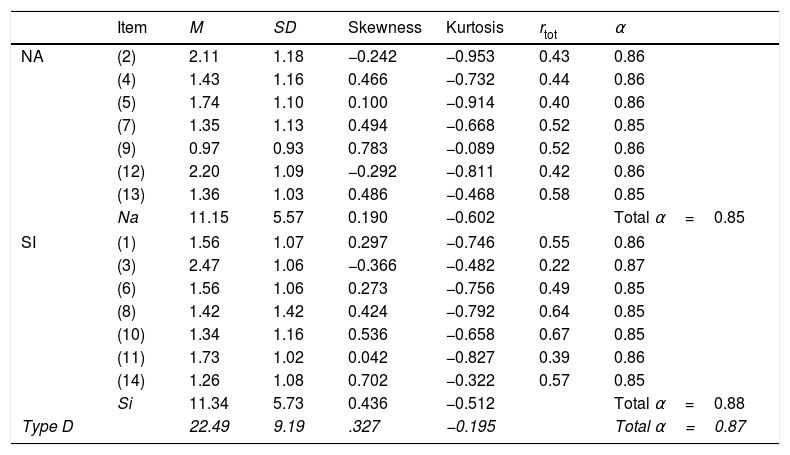
The mean for the total scale was 22.49 (SD=9.19), 11.15 for NA and 11.34 for SI. There were significant differences between men and women in SI (t-test=2.157, p<0.031), with men achieving significantly higher scores than women. There were no significant differences by age (F=0.818; df=3; p<0.484 for NA and F=1.056; df=3; p<0.367 for SI) or by marital status (F=1.231; p<0.297 for NA and F=1.525, df=4, p<0.193 for SI). As shown in Table 2, Cronbach's alpha indicates a satisfactory internal consistency, both for the total scale (α=0.87) and for its subscales (α=0.85 in NA and α=0.80 in SI).
Means, standard deviations, skewness, kurtosis, corrected item-total correlations (rtot), internal consistency of the scale if the item is eliminated (α).
| Item | M | SD | Skewness | Kurtosis | rtot | α | |
|---|---|---|---|---|---|---|---|
| NA | (2) | 2.11 | 1.18 | −0.242 | −0.953 | 0.43 | 0.86 |
| (4) | 1.43 | 1.16 | 0.466 | −0.732 | 0.44 | 0.86 | |
| (5) | 1.74 | 1.10 | 0.100 | −0.914 | 0.40 | 0.86 | |
| (7) | 1.35 | 1.13 | 0.494 | −0.668 | 0.52 | 0.85 | |
| (9) | 0.97 | 0.93 | 0.783 | −0.089 | 0.52 | 0.86 | |
| (12) | 2.20 | 1.09 | −0.292 | −0.811 | 0.42 | 0.86 | |
| (13) | 1.36 | 1.03 | 0.486 | −0.468 | 0.58 | 0.85 | |
| Na | 11.15 | 5.57 | 0.190 | −0.602 | Total α=0.85 | ||
| SI | (1) | 1.56 | 1.07 | 0.297 | −0.746 | 0.55 | 0.86 |
| (3) | 2.47 | 1.06 | −0.366 | −0.482 | 0.22 | 0.87 | |
| (6) | 1.56 | 1.06 | 0.273 | −0.756 | 0.49 | 0.85 | |
| (8) | 1.42 | 1.42 | 0.424 | −0.792 | 0.64 | 0.85 | |
| (10) | 1.34 | 1.16 | 0.536 | −0.658 | 0.67 | 0.85 | |
| (11) | 1.73 | 1.02 | 0.042 | −0.827 | 0.39 | 0.86 | |
| (14) | 1.26 | 1.08 | 0.702 | −0.322 | 0.57 | 0.85 | |
| Si | 11.34 | 5.73 | 0.436 | −0.512 | Total α=0.88 | ||
| Type D | 22.49 | 9.19 | .327 | −0.195 | Total α=0.87 | ||
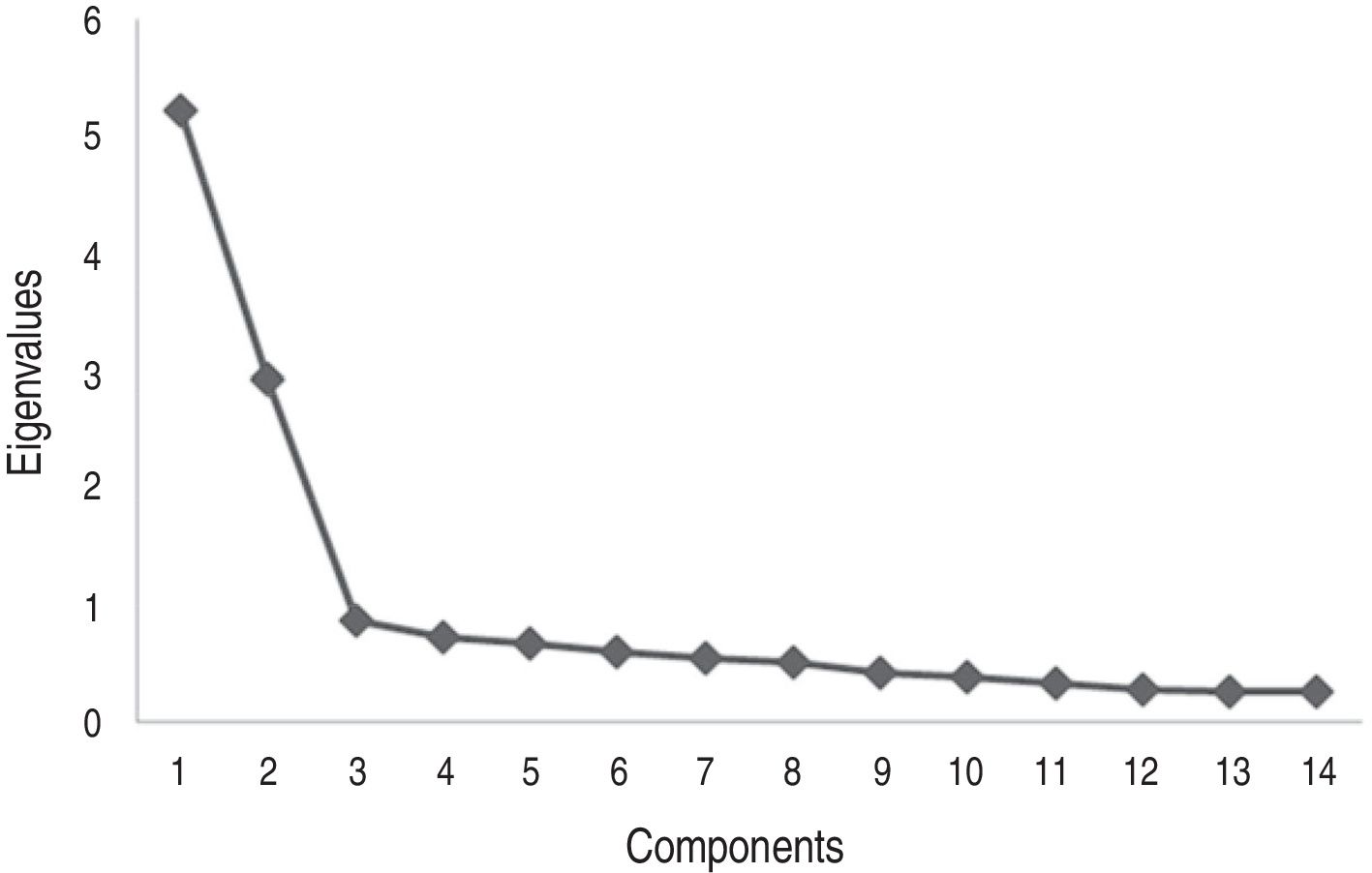
For the exploratory factor analysis, principal components method was used, first with oblique and then with orthogonal rotation, both with Kaiser normalization. Bartlett's test (Bartlett's test=2092.315; p<0.01) and the Kaiser–Meyer–Olkin coefficient (0.88) showed that data fulfilled the assumptions for conducting the factor analysis. The factorial structure showed a two-factor solution, with eigenvalues of 5.22 and 2.93 for NA and SI respectively. This explains 58.3% of the variance, 37.3% for NA and 21% for SI. As shown in Fig. 1, the plot also showed that the two-factor model was the most adequate to represent the data. Velicer Maps method and Parallel analysis confirmed the two-factor model as being more appropriate.

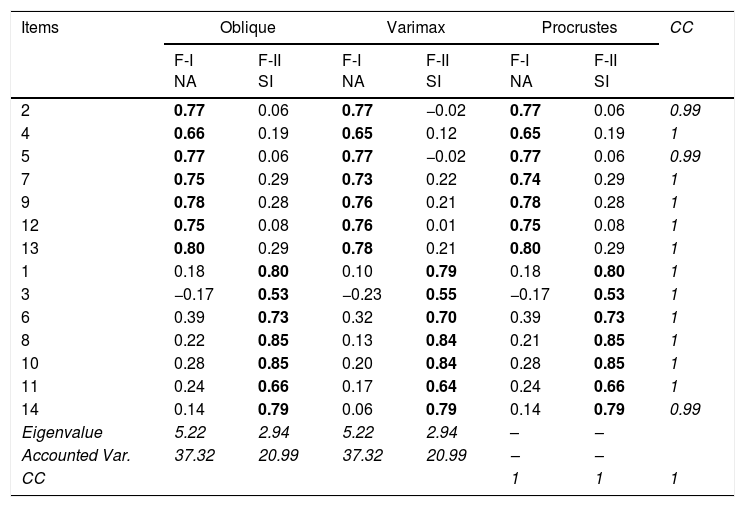
Oblique rotation method obtained structure factor loadings between 0.75 and 0.80 for the first factor (NA) and between 0.53 and 0.80 for the second one (SI). The Varimax matrix showed factorial loadings between 0.65 and 0.78 for the first factor (NA) and between 0.55 and 0.84 for the second (SI). The Procrustes rotation method report high coefficients of congruence both between items and between factors (between 0.99 and 1), indicating that both rotation methods are practically identical (Table 3).
Oblique, varimax and procrustes rotation matrices and factorial congruency coefficients.
| Items | Oblique | Varimax | Procrustes | CC | |||
|---|---|---|---|---|---|---|---|
| F-I NA | F-II SI | F-I NA | F-II SI | F-I NA | F-II SI | ||
| 2 | 0.77 | 0.06 | 0.77 | −0.02 | 0.77 | 0.06 | 0.99 |
| 4 | 0.66 | 0.19 | 0.65 | 0.12 | 0.65 | 0.19 | 1 |
| 5 | 0.77 | 0.06 | 0.77 | −0.02 | 0.77 | 0.06 | 0.99 |
| 7 | 0.75 | 0.29 | 0.73 | 0.22 | 0.74 | 0.29 | 1 |
| 9 | 0.78 | 0.28 | 0.76 | 0.21 | 0.78 | 0.28 | 1 |
| 12 | 0.75 | 0.08 | 0.76 | 0.01 | 0.75 | 0.08 | 1 |
| 13 | 0.80 | 0.29 | 0.78 | 0.21 | 0.80 | 0.29 | 1 |
| 1 | 0.18 | 0.80 | 0.10 | 0.79 | 0.18 | 0.80 | 1 |
| 3 | −0.17 | 0.53 | −0.23 | 0.55 | −0.17 | 0.53 | 1 |
| 6 | 0.39 | 0.73 | 0.32 | 0.70 | 0.39 | 0.73 | 1 |
| 8 | 0.22 | 0.85 | 0.13 | 0.84 | 0.21 | 0.85 | 1 |
| 10 | 0.28 | 0.85 | 0.20 | 0.84 | 0.28 | 0.85 | 1 |
| 11 | 0.24 | 0.66 | 0.17 | 0.64 | 0.24 | 0.66 | 1 |
| 14 | 0.14 | 0.79 | 0.06 | 0.79 | 0.14 | 0.79 | 0.99 |
| Eigenvalue | 5.22 | 2.94 | 5.22 | 2.94 | – | – | |
| Accounted Var. | 37.32 | 20.99 | 37.32 | 20.99 | – | – | |
| CC | 1 | 1 | 1 | ||||
Note: Factorial loadings higher or equal to 0.40 were in boldface. F-I: Factor 1; F-II: Factor 2; CC:congruency coefficients.
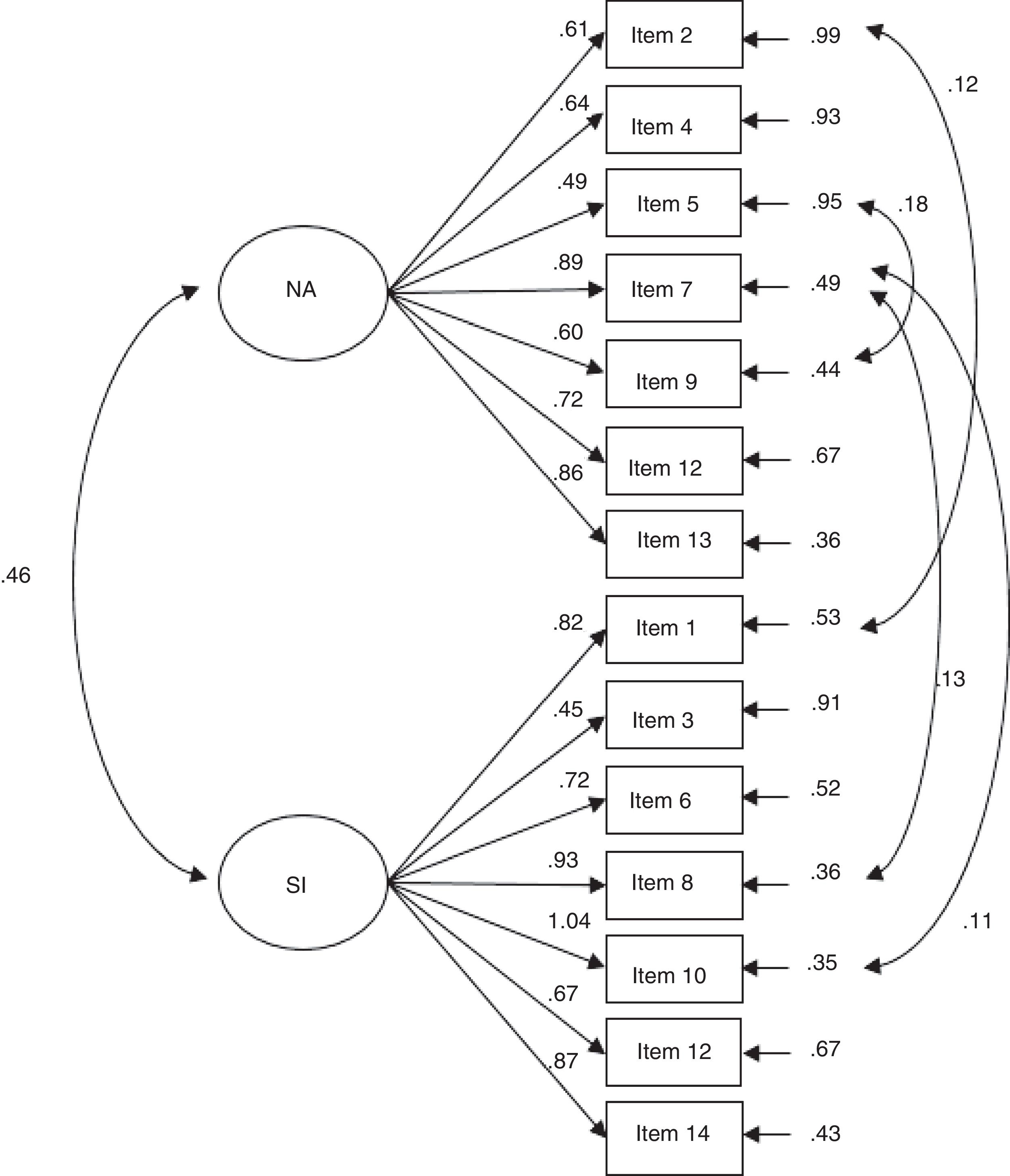
A CFA was performed using the maximum likelihood method in the validation subsample, taking the 14 items of the DS14 as observed variables and the two factors as latent. The goodness of fit indexes used were chi-square, the chi-square/degrees of freedom (χ2/df), RMSEA (root-mean square-error of approximation), SRMR (standardized root mean square residual), GFI (Goodness-of-Fit Index), TLI (Tucker–Lewis Index), CFI (Comparative Fit Index) and IFI (Incremental Fit Index). It was considered that a χ2/df lower than 3 represented a good fit of the model; for RMSEA and SRMR, values below 0.05 indicated a close to fit and values of up to 0.08 indicated reasonable approach errors; Values greater than 0.90 for GFI, TLI, IFC and IFI were considered to reflect a good fit to the model. To improve the goodness of fit indexes, a re-specified model was created by correlating the error terms of the highly correlated items, using as a criterion a modification index value equal to or greater than 10 (Blanch & Aluja, 2009; Hu & Bentler, 1995).
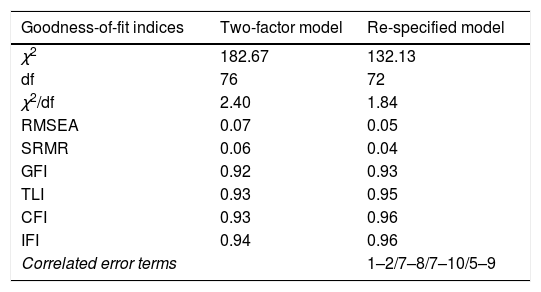
Table 4 shows the analysis revealed a Chi-squared/degrees of freedom (χ2/df=2.404) ratio with a value below 3, indicating that the model presents a good fit to the data. A RMSEA and SRMR less than 0.08 represented a good fit to data. The GFI, TLI, IFC and IFI showed a good fit due to their proximity to 1 (>0.90). In addition, the items were good indicators of their respective latent factors with standardized factor loads of between 0.49 and 0.82 for NA, and between 0.43 and 0.88 for SI. The correlation between the factors was 0.47. The re-specified model, with correlations between the error terms of 4 pairs of highly correlated items, slightly improved the goodness of fit indexes, obtaining a χ2/df lower than 2 a RMSEA and a SRMR very close to 0.05, and closest values to 1 in GFI, TLI, IFC and IFI. The path analysis is showed in Fig. 2.
Goodness-of-fit indices for the two-factor model and the re-specified model.
| Goodness-of-fit indices | Two-factor model | Re-specified model |
|---|---|---|
| χ2 | 182.67 | 132.13 |
| df | 76 | 72 |
| χ2/df | 2.40 | 1.84 |
| RMSEA | 0.07 | 0.05 |
| SRMR | 0.06 | 0.04 |
| GFI | 0.92 | 0.93 |
| TLI | 0.93 | 0.95 |
| CFI | 0.93 | 0.96 |
| IFI | 0.94 | 0.96 |
| Correlated error terms | 1–2/7–8/7–10/5–9 |
Note: χ2:Chi-squared; df:degree freedom; RMSEA: root-mean square-error of approximation; SRMR: standardized root-mean square-residual; GFI: Goodness-of-Fit Index; TLI: Tucker–Lewis Index; CFI: Comparative Fit Index; IFI: Incremental Fit Index.

The prevalence of Type D in the total sample was 37.3%. There were significant differences between groups in social position (χ2=9.80, df=3, p<0.02). No differences were found regarding gender (χ2=0.33, df=1, p<0.57) age (χ2=0.44, df=3, p<0.93) and marital status (χ2=4.16, df=4, p<0.39).
DiscussionThis study was designed to evaluate the psychometric properties of the Catalan version of DS14. The two factor structure was replicated in both oblique and orthogonal rotation methods. No differences in the two methods were found. confirmatory factorial analysis inform that the two factor structure had good goodness-of-fit indexes. The DS14 psychometric properties have therefore been replicated in the present study, and are comparable with the results of the studies conducted in different countries and cultures mentioned in the introductory section. With regard to confirmatory factor analysis, it has been necessary in some studies to correlate several errors terms to get a satisfactory fit index, but in our study the simple structure was obtained without it being necessary to include the correlated error terms. However, as we expected, a re-specified model including some correlated error terms improved the model. A good internal consistency was obtained, equivalent to other studies. The test-retest reliability cannot be assessed because of the anonymous nature of an online study.
In this study, the prevalence of Type D personality in the general population was 37.3% higher to what has been observed in other studies for a healthy sample. However, this high percentage is similar to the 31% prevalence in the German population reported by Grande et al. (2010). In this line, Ferguson et al. (2009) reported a prevalence of 39.6% of females and 34.7% of males (n=1012 healthy young adults, 787 females and 225 males). Additionally, in other studies with non-patient samples, the prevalence rates ranged between 21% and 38.5% (see the revision by Grande et al., 2010).
The present data do not allow us to explain the great variability. One possibility is that Denollet (2005) used the median split method to categorize the scores obtained in the subscales, but the medians do not replicate cross-culturally (Grande et al., 2010). On the other hand, although the study by Emons, Meijer, and Denollet (2007) based on item response theory supports the original cut-off point, the sample and the data used are the same as in the original article by Denollet (2005), so its cross-cultural replicability is also in doubt. One solution to the problem could be to adopt a continuous or dimensional approach (Ferguson et al., 2009), although some authors would argue against it on the grounds that health professionals are more accustomed to thinking categorically (Zohar et al., 2011). Another solution could be to establish differentiated cut-off points for different populations. All these are issues to be addressed in future research.
The results of this study have several implications. On the one hand, it is shown that this scale is psychometrically robust in the Catalan language. This, coupled with the short time required to complete it, makes it an optimal tool for detecting Type D personality in the Catalan population. In addition, since Type D has been shown to be a predictor of morbidity and mortality (Denollet et al., 1996) once the disease is present and has been established as a predictor of poor prognosis in coronary interventions (Denollet et al., 2000), the use of this instrument may be useful as a screening tool to stratify and identify high-risk patients in different cardiology units. This instrument can also be useful for detecting subjects with a high coronary risk in healthy populations, because if they score as Type D, they have higher levels of stress, anxiety and depression, and refer less social support and less subjective well-being (Zohar et al., 2011).
This study has several limitations. First, the sample is limited to people who work in a university environment with representation of professors, administrative personnel and services, and students. In future studies, it would be advisable to investigate different groups of patients, which will allow a more accurate estimation of the prevalence of Type D personality in the Catalan population. Secondly, measures regarding test-retest reliability to verify temporal stability as well as convergent and divergent validity data are not contemplated here, and should be addressed in future research.
In summary, this study replicated the psychometric properties of the online version of Type D personality scale (DS14) in an extensive sample from a healthy Catalan population. The results demonstrate construct validity and internal consistency similar to those obtained in different countries and cultures. The Catalan version of DS14 can be used in epidemiological research in the Catalan language. These results open up the possibility of continuing the investigation of this instrument in different samples and variables that confer additional validity to the DS14. This study is a first step in this direction.
