

We present a single-case study on the potential clinical relevance of a new altered auditory feedback (AAF) device (Forbrain®) in stuttering. One adult who stutter was tested in an appropriately-controlled single-case time-series (A-B-A) study. On each of six consecutive working days, the stuttering adult was instructed to read aloud during three different experimental phases: Baseline, Test and Post-test, while wearing a Forbrain® headset. During the Test phase the device was turned on, whereas it was off during Baseline and Post-test phases. This way the transient effects of Forbrain® could be analyzed. Six quantitative measures of voice quality were retrieved from the participant's voice recordings during his readings over each phase of the experiment. Data was statistically analyzed through the single-case d-statistic. A clear transient effect of Forbrain®, when turned on, was observed on voice quality, supported by significant differences between Baseline and Test, and Test and Post-test in the tilt of the trendline of the long term average spectrum (tLTAS) of the voice. The present single-case study support the effectiveness of Forbrain® in modifying the voice during stuttering, supporting its role as an AAF device.
Presentamos un estudio de caso único sobre la potencial relevancia clínica de un nuevo dispositivo de realimentación auditiva retardada (Forbrain®) en la tartamudez. Se examinó un adulto con tartamudez mediante un diseño de series temporales de caso único (A-B-A) adecuadamente controlado. En cada uno de 6 días consecutivos se dieron instrucciones al sujeto para leer en voz alta durante las 3 fases del estudio: línea base, test y post-test, mientras llevaba colocado un dispositivo Forbrain®. Durante las fases línea base y post-test, el aparato estaba apagado, mientras que este se conectó durante la fase de test. De esta manera se pudieron analizar los efectos transitorios de Forbrain®. Se obtuvieron 6 parámetros cuantitativos de la calidad de la voz durante la lectura a partir de los registros de esta durante cada una de las fases del experimento. Los datos se analizaron estadísticamente mediante el estadístico d para casos únicos. Se observó un claro efecto de Forbrain® en la calidad de la voz al conectar el dispositivo, según revelaron los contrastes significativos ente la línea base y el test, y el test con el post-test en el parámetro tLTAS de la voz. El presente estudio de caso único sugiere la efectividad de Forbrain® para modificar la voz durante el tartamudeo, y da apoyo a la funcionalidad de este como dispositivo de realimentación auditiva retardada.
Persistent developmental stuttering is a communication impairment that affects the individual's ability to speech fluently. It is characterized by involuntary speech disruptions, sound or syllables repetitions, sound prolongations and blocks. It is also accompanied by physical tension while speaking and some characteristic gestures, such as facial grimaces, eye blinking and jaw and neck jerking (Bloodstein & Bernstein-Ratner, 2008). The prevalence of stuttering is about 2–5% of children aged 3–6 years and remits spontaneously in about 80% of these children, yet leaving about 1% of the adult population with the speech impairment. Although the causes of stuttering are currently unknown, recent theoretical accounts have proposed a three-factor model in which (1) a core deficit in the neural processing of spoken language may be susceptible to (2) external triggers which may in turn intervene through (3) a range of modulating factors (Packman, 2012). Importantly, this model is compatible with increasing evidence highlighting the role of central auditory deficits in stuttering (Cai et al., 2012; Corbera, Corral, Escera, & Idiazábal, 2005; Halag-Milo, 2016; Halliday, Barry, Hardiman & Bishop, 2014; Hampton & Weber-Fox, 2008; Ritto, Costa, Juste & de Andrade, 2016a). This may explain why fluency can be temporarily improved in persons who stutter, at least in developmental stuttering, by providing altered auditory feedback (AAF) during speech production in several of its different forms (Cai et al., 2012; Packman, 2012).
AAF are a series of procedures that alter the speaker's voice through electronic or digital manipulation, so that it is perceived differently from normal (Fairbanks, 1954; Yates, 1963). Most typical versions of AAF include masked auditory feedback (MAF), in which the speech signal is presented under a white or pink noise, delayed auditory feedback (DAF) in which the feedback is delayed regarding the input for about 50–250ms, and frequency-altered feedback (FAF), where an increase or decrease in the fundamental frequency of the speech is applied to the feedback (Lincoln, Packman & Onslow, 2006). There are other less clinically used forms of AAF, such as the Lombard effect (Arciuli, Simpson, Vogel, & Ballard, 2013; Garnier, Henrich, & Dubois, 2010; Stathopoulus et al., 2014), sidetone amplification (Garber, Siegel, & Pick, 1976; Heinks-Maldonado & Houde, 2005; Bauer, Mittal, Larson, & Hain, 2006) and the so-called feedback filtering (Burzynski & Starr, 1985; Garber et al., 1976; Garber, Siegel, & Pick, 1980, 1981), which alter the speech input in the amplitude domain or in specific frequency bands. These forms of AAF have been shown also to affect speech in fluent speaking adults and stutterers (Martin, Siegel, Johnson, & Haroldson, 1984). A recent proposal posits that AAF may work through a mechanism of motor compensation, so that a compensatory motor command is issued to correct the perceived shift in the acoustic input based on a predictive internal model of the expected output (Hahnloser & Narula, 2017; Ostry & Gribble, 2016). Further, the so-called Spt area in the planum temporale of the left temporal lobe has been proposed as the candidate brain region to support these predictive interactions (Hickok, Houde, & Rong 2011). The compensatory motor command mentioned above may result in the retuning of the phono-articulatory loop (Eliades & Wang, 2008; Keller & Hahnloser, 2009), and may have in turn, consequences on the speaker's voice (Houde & Jordan, 1998; Jones & Munhall, 2000).
Several AAF devices for the treatment of stuttering are currently available, such as SpeechEasy® (Janus Development Group; Greenville, NC, USA; Foundas, Mock, Corey, Golob, & Conture, 2013), SmallTalk® and Basic Fluency System® (Casa Futura Technologies; Boulder, CO, USA; Unger, Glück, & Cholewa, 2012) and VA601i Fluency Enhancer (VoiceAmp LTd; Capetown, South Africa; Unger et al., 2012); yet the evidence supporting their effects in treating stuttering is weak (Ritto, Juste, Stuart, Kalinowksi, & de Andrade, 2016b; Select Health of South Carolina, 2016). Moreover, with the development of the World Wide Web (WWW), many new telehealth services, technologies and gadgets can now be easily accessed remotely by persons experiencing different forms of speech-language pathology, including those who stutter (Packman & Meredith, 2011). However, due to their rapid development and easy access, many of these new opportunities lack the appropriate clinical testing and supporting evidence.
Among these new tools, Forbrain® (Sound For Life Ltd.), Luxemburg is available through the Internet since 2015. Forbrain® is a headset equipped with a microphone and a pair of bone conductors, which feeds the user back with his/her own voice during natural speech through bone conduction. Forbrain® incorporates a patented electronic dynamic filter that isolates and amplifies the user's voice by blocking out environmental noise. The filter also amplifies the transmission of high frequencies, while simultaneously diminishing low ones, and reacts to the intensity of the voice, so that the user hears his/her own voice filtered with alternating contrast. The resulting sound is delivered through the bones by a process of bone conduction, so that the travelling waveform of a sound can reach the inner ear, induce a travelling wave in the basilar membrane and hence stimulate the cochlea by the same mechanisms as normal air conduction but via bone vibration (Stenfelt & Goode, 2005). Compared to other AAF devices for the treatment of stuttering, one major difference of Forbrain® is that it provides AAF in the amplitude domain (Escera, López-Caballero, & Gorina-Careta, 2018), similar to that of the semitone amplification (Bauer et al., 2006; Garber et al., 1976; Heinks-Maldonado & Houde, 2005) or feedback filtering (Burzynski & Starr, 1985; Garber et al., 1976, 1980, 1981). Moreover, a recent study conducted in healthy volunteers with no personal or familiar history of speech or language disorders showed that Forbrain®, when in use, alters the speaking voice of its users (Escera et al., 2018). The present report describes a single-case time-series study, implemented with an A-B-A design, on an adult who stutters, on the potential effects of Forbrain® on the user's voice. Single-case time-series or single-case designs can provide a rigorous experimental evaluation of intervention effects and are widely use in applied and clinical psychology (Kratochwill et al., 2010). Also they are an excellent option to test a new therapeutical approach before attempting an expensive and time cosuming case-control study. The present study was carried out and reported following the recommendations by Manolov (2017). Voice was chosen as dependent variable because it allows objective and quantitative analysis based on its sound recording, beyond subjective interpretation. Besides, a recent study supported the use of voice to investigate Forbrain® effects, particularly on two specific objective measures: smoothed cepstral peak prominence (CPPS) and spectral trendline inclination (tilt; tLTAS) (see below; Escera et al., 2018).
MethodsSingle caseThe participant was a persistent developmental stuttering adult, 25-year-old man (right handed), with ten years obligatory (secondary) education completed and job as photographer, and with no history of neurological or psychiatric disorders and normal hearing (hearing thresholds<20dB SPL as determined in our lab with a standard audiometry). He was diagnosed at the age of eleven years and reported to have his mother and father to stutter. He presented symptoms and behaviours consistent with a DSM-5 diagnosis of Childhood-Onset Fluency Disorder (Stuttering), including sound and syllable repetitions, audible and silent blockings, and monosyllabic whole-word repetitions. These symptoms were of moderate severity, as noted during the preliminary interview, and evident when reading aloud. As measured with the self-administered questionnaire ‘Conduct and Attitude Scale for the Assessment of Disfluencies (CASAD)’ (total score of 24/100; see Corbera et al., 2005), the participant showed a general positive attitude towards the disorder, despite it had a clear impact on a variety of areas of his daily life. He had no musical expertise.
ProcedureThe study was conducted in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki). The participant was asked to refrain from alcohol intake and from taking any pills during the 24h before the sessions. Before the study began, all its details were explained, and signed informed consent was obtained before the first study session. The study was carried out in the facilities of our laboratory, in six individual sessions, arranged in six consecutive working days, each lasting for about 40–50min. Upon arrival to the lab, instructions were given, and a standard headset of Forbrain® (Sound For Life Ltd./Soundev, Luxemburg; http://www.forbrain.com) was mounted on the stutterer's head, in a way that he felt comfortable, with the microphone located at 3cm from his mouth. He was seated comfortably in a sound-attenuated chamber, and was instructed to read aloud, on a self-administered but regular pace, a text of his choice in a fix arrangement of three runs: one lasting 7min during which Forbrain® was kept off (serving as Baseline); one lasting 14min during which Forbrain® was turned on (Test phase), and a final Post-test run lasting for 7min in which Forbrain® was turned back off. The texts to read along the different phases of each session and along the different sessions of the study were all different passages of the same narrative. The narrative was freely chosen by the participant amongst a collection of short stories on different topics (e.g., travel, the sea, etc.). The duration of the reading phases was set to optimize the total session length while maximizing the time during which the device was set on, so that potential cumulative effects could take place along the 14min set. During the reading periods the participant's voice was continuously recorded. Voice recordings were sampled at a rate of 44.1kHz using a DR-40 TASCAM Microphone (TEAC America, Inc) placed in a fixed position on the table in front of the participant, with a mouth-to-microphone distance of approximately 30cm. The voice samples were saved in WAV-format.
Data processingVoice recordings were processed so that six different acoustic parameters were derived from each session and phase, according to the method proposed by Maryn and Weenink (2015). These parameters have been proved of clinical relevance in cases of dysphonia, dysarthria, in forensic aspect of voice and also in assessing emotion, mood an attitude based on voice quality (Gobl & Ní Chasaide, 2003), and we argue they can provide relevant clinical information regarding the altered speech of persons who stutter. The six parameters are as follows: (1) The smoothed cepstral peak prominence (CPPS), which measures the degree of harmony in a voice sample (Hillenbrand & Houde, 1996; Heman-Ackah, Michael, & Goding, 2002), and increases as the voice signal is more periodic, being considered a reliable and valid measure of voice quality, especially, breathiness (Maryn, Corthals, Van Cauwenberge, Roy, & De Bodt, 2010). (2) The harmonics-to-noise ratio (HNR), which is a glottal noise measure that refers to the relative contributions of aperiodic and periodic components of the voice signal, with periodic voice signals having larger HNR. This feature is closely related to the efficacy of the vocal fold closure. (3) The shimmer local (ShimLoc) and (4) the shimmer local dB (ShimDB), which measure the irregularities or perturbation in the amplitude of cycles of the voice sample. Physiologically, such perturbation could be produced by some asymmetry in the vocal folds, which would make them to meet the same way only every two or three cycles, causing the periodicity to be achieved every second or third cycle of the vibration, respectively. Finally two measures were obtained based on the long term average spectrum (LTAS). This quantifies the averaged frequency spectrum of a speech signal over a long stretch of speech (Vaňková & Skarnitzl, 2014), and the signal obtained is representative of the vocal behaviour of the glottic source as the sound is transferred through the vocal tract. By averaging a long portion of speech, all the spectral differences caused by individual segments are averaged out, thus providing information pertaining to the general quality of voice (Vaňková & Skarnitzl, 2014). For LTAS, (5) the general spectral slope (sLTAS) was measured as the difference between the energy in the 0–1kHz range and the energy in the 1–10kHz range of the long-term average spectrum; and (6) the spectral trendline inclination (tilt; tLTAS) was computed as the difference between the energy in the 0–1kHz range and the energy in the 1–10kHz range of the trendline through the long-term average spectrum. Based on our previous study on healthy volunteers (Escera et al., 2018), we expect that the most sensitive and clinically relevant parameters would be CPPS and tLTAS.
Statistical analysisTo analyze whether the use of Forbrain® had any overall effect on the stutterer's voice across the six days of the experiment, we applied statistical analysis suited for single-case studies (Manolov, Gast, Perdices & Evans, 2014; Shadish, Hedges, Pustejovsky, Boyajian, et al., 2014; Shadish, Hedges & Pustejovsky, 2014). These analyses were carried out over the six acoustic measures extracted from the voice recording segments. Statistical comparisons were carried out for differences between Baseline and Test, Test and Post-test, and Baseline and Post-test. First, the mean amplitude and standard deviation of measurements during Baseline, Test and Post-test were retrieved and the Glass's Δ statistic was calculated to estimate the size of the effect, separately for each day. Then, a standardized mean difference statistic (d-statistic) for single-case designs was calculated in order to estimate the overall effect of the six days of Forbrain® use. This statistic is equivalent to the Glass's Δ used in between-groups experiments but relies here on the total variance across the single participant, and it is the most appropriate choice for short-time series, as in the present study (Manolov, 2017). This d-statistic requires at least three cases to estimate it and its standard error, and assumes that no time trends are present in the baseline, that the treatment effect is constant across cases and that the outcome measures are normally distributed (Manolov et al., 2014; Shadish, Hedges, Pustejovsky, Boyajian, et al., 2014; Shadish, Hedges & Pustejovsky, 2014). Because the baseline recordings in the present study had only three measurements, it was assumed that no time trends were present in the baseline. To test the statistical significance of the d-statistic, a confidence interval was computed using the following formula: CI=d±z·σ(d) where d is the standardized mean difference statistic, z is the z-score which corresponds to a 95% of confidence (i.e. 1.96) and σ is the square root of the d-statistic variance. If the confidence interval excludes the zero value, it can be assumed that the difference between the mean amplitude of two measurements is statistically significant different from zero.
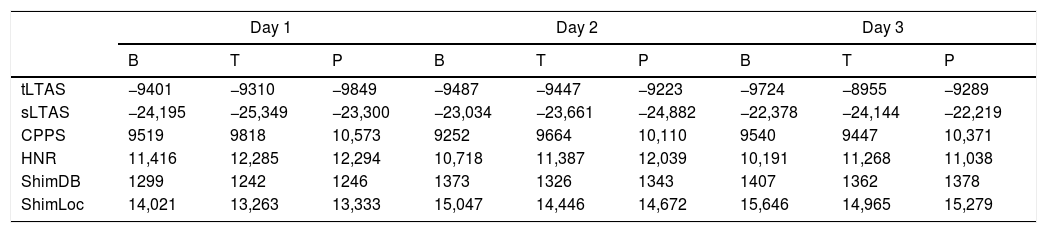
ResultsThe statistical analyses revealed a clear effect of Forbrain® on the stutterer's voice during its use, as supported by significant results in two out of the six objective voice parameters analyzed (Table 1). First, tLTAS was significantly and consistently different across the reading runs along the six experimental days, as there was a significant effect on tLTAS when comparing the Baseline with the Test (d-statistic=0.995, CI=[1.584–0.405]) and the Test with the Post-test (d-statistic=−1.132, CI=[−0.513 to −1.750]), whereas the Baseline versus Post-test comparison was not significant (d-statistic=−0.300, CI=[0.176 to −0.777]). The combination of the significant d-statistic for the contrast Baseline versus Test and the contrast Test versus Post-test, together with the lack of differences between Baseline and Post-test indicates that when Forbrain® was turned on the tLTAS increased in a significant manner, to recover its baseline level when Forbrain® was turned off (Fig. 1, top). A similar pattern of results was observed for the slope of the long term average spectrum (sLTAS). Indeed, significant differences were observed between Baseline and Test (d-statistic=−0.495, CI=[−0.065 to −0.924]) and between Test and Post-test – (d-statistic=0.643, CI=[1.129–0.157]), whereas the Baseline and Post-test measurements of sLTAS did not differ significantly (d-statistic=0.254, CI=[0.653 to −0.145]).
Mean across each of the phases (B, baseline; T, Test; P, Post-test) and days (1–6) of the six acoustic parameters measured in the experiment.
| Day 1 | Day 2 | Day 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| B | T | P | B | T | P | B | T | P | |
| tLTAS | −9401 | −9310 | −9849 | −9487 | −9447 | −9223 | −9724 | −8955 | −9289 |
| sLTAS | −24,195 | −25,349 | −23,300 | −23,034 | −23,661 | −24,882 | −22,378 | −24,144 | −22,219 |
| CPPS | 9519 | 9818 | 10,573 | 9252 | 9664 | 10,110 | 9540 | 9447 | 10,371 |
| HNR | 11,416 | 12,285 | 12,294 | 10,718 | 11,387 | 12,039 | 10,191 | 11,268 | 11,038 |
| ShimDB | 1299 | 1242 | 1246 | 1373 | 1326 | 1343 | 1407 | 1362 | 1378 |
| ShimLoc | 14,021 | 13,263 | 13,333 | 15,047 | 14,446 | 14,672 | 15,646 | 14,965 | 15,279 |
| Day 4 | Day 5 | Day 6 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| B | T | P | B | T | P | B | T | P | |
| tLTAS | −9421 | −8679 | −10,333 | −9475 | −9360 | −9764 | −9514 | −9081 | −9325 |
| sLTAS | −23,819 | −26,465 | −21,293 | −23,078 | −21,591 | −21,535 | −22,591 | −23,373 | −23,698 |
| CPPS | 9605 | 9289 | 10,053 | 9231 | 9489 | 10,202 | 9808 | 9631 | 10,181 |
| HNR | 10,757 | 11,373 | 10,659 | 10,437 | 10,047 | 10,577 | 10,965 | 10,752 | 11,275 |
| ShimDB | 1375 | 1382 | 1392 | 1395 | 1412 | 1387 | 1336 | 1386 | 1364 |
| ShimLoc | 15,281 | 15,176 | 15,410 | 15,546 | 15,803 | 15,461 | 14,576 | 15,353 | 15,280 |
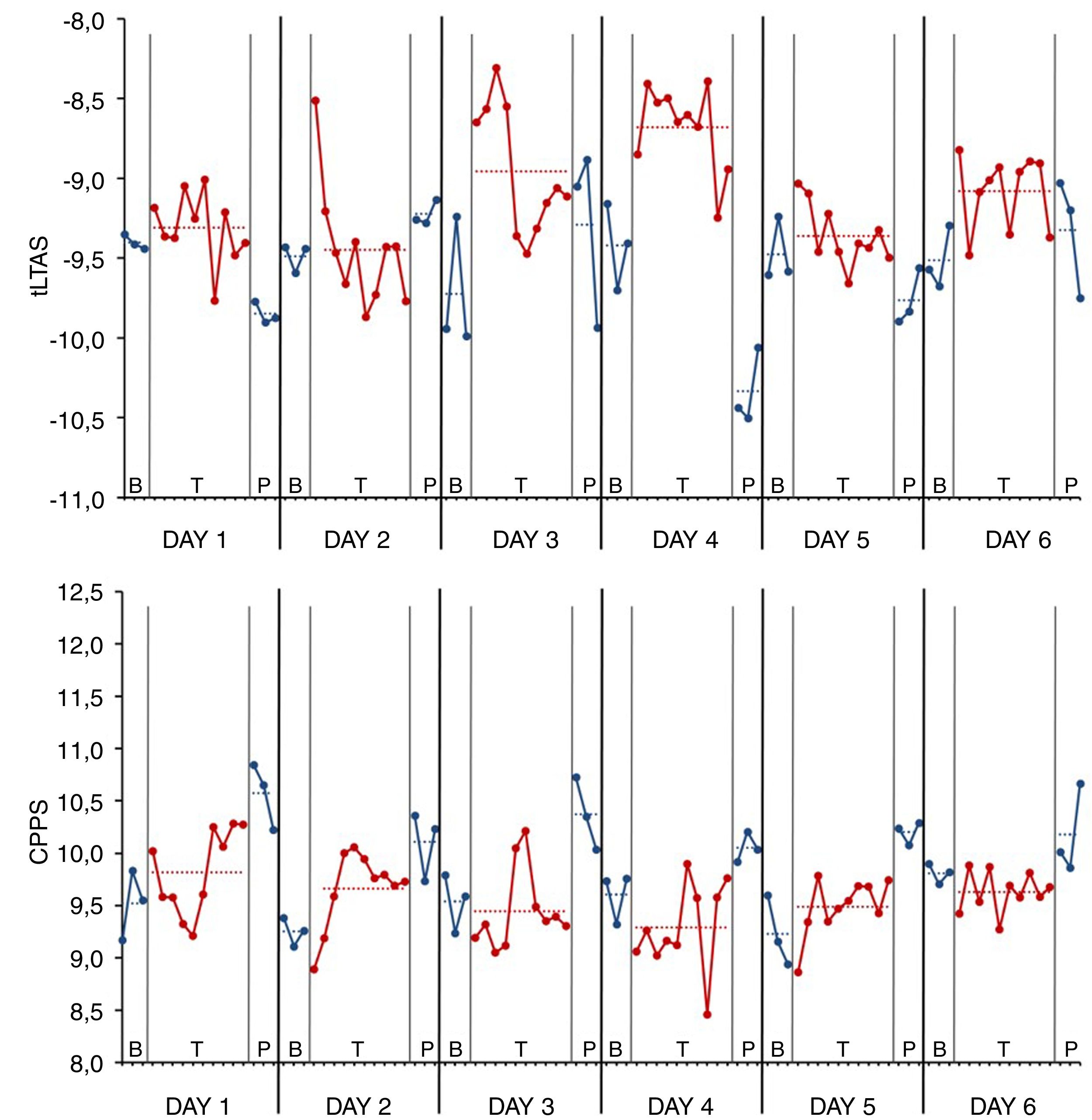
![Voice quality measurements across the three phases (Baseline [B], blue; Test [T], red; Post-test [P]; blue) and along the six days of the study in the AWS. (Top) Tilt of the trendline of long term average spectrum (tLTAS). Notice that for every of the single days of the study, when Forbrain® was turned on during the Test phase, the tLTAS increased, to return to baseline level when the device was turned off. (Bottom) Smoothed cepstral peak prominence (CPPS). Here, no significant differences were observed between Baseline and Test, but CPPS increased in the Post-test phase, compared to both Test and Baseline phases.](https://static.elsevier.es/multimedia/00665126/0000004800000002/v1_201810070718/S0066512618300151/v1_201810070718/en/main.assets/gr1.jpeg?xkr=ue/ImdikoIMrsJoerZ+w997EogCnBdOOD93cPFbanNfMxPujdHrEeG4f3s86xAjO5cBU5IvoB459YPqDE/94IGbez0oBQWvguIpveqc/i0AG6BbLw0w0dapD3WpzzMy3OCZ3gsIogKbkfXn6OIE5kmp9fNdUh2vsT0uwprTErSnzrHo0TSGTN6atmPcxR1ZnTR4LQHt2yRedokMlBEDqB3an3DVFaFq5KxJpgb6D1shYhPr1IsbGO0kZDoE1mkWvDVq7CTiaYvSXp0xMF/a2tLxPmC3nXQVbk5dDkMm19Qo= "Voice quality measurements across the three phases (Baseline [B], blue; Test [T], red; Post-test [P]; blue) and along the six days of the study in the AWS. (Top) Tilt of the trendline of long term average spectrum (tLTAS). Notice that for every of the single days of the study, when Forbrain® was turned on during the Test phase, the tLTAS increased, to return to baseline level when the device was turned off. (Bottom) Smoothed cepstral peak prominence (CPPS). Here, no significant differences were observed between Baseline and Test, but CPPS increased in the Post-test phase, compared to both Test and Baseline phases.")
Voice quality measurements across the three phases (Baseline [B], blue; Test [T], red; Post-test [P]; blue) and along the six days of the study in the AWS. (Top) Tilt of the trendline of long term average spectrum (tLTAS). Notice that for every of the single days of the study, when Forbrain® was turned on during the Test phase, the tLTAS increased, to return to baseline level when the device was turned off. (Bottom) Smoothed cepstral peak prominence (CPPS). Here, no significant differences were observed between Baseline and Test, but CPPS increased in the Post-test phase, compared to both Test and Baseline phases.
On the other hand, the smoothed cepstral peak prominence (CPPS) was also significantly affected during Forbrain® use. The statistical analyses revealed significant differences between Test and Post-test (d-statistic=1.920, CI=[2.662–1.177]) and between Baseline and Post-test (d-statistic=2.357, CI=[3.265–1.450]), while there were no differences between Baseline and Test (d-statistic=0.179, CI=[0.829 to −0.470]) (Fig. 1, bottom). This pattern of results suggest that after the use of Forbrain® for about fourteen minutes, CPPS experiences a large increase compared to the baseline, supporting the role of Forbrain® in modulating voice quality. A further significant result was obtained for the harmonics-to-noise ratio (HNR) parameter, as it showed a significant increase from Baseline to Test (d-statistic=0.490, CI=[0.975–0.005]), and from Baseline to Post-test (d-statistic=0.766, CI=[1.099–0.397]), whereas the measurements obtained in Test and Post-test were similar (d-statistic=0.135, CI=[0.564 to −0.294]), altogether suggesting that Forbrain® rose the parameter to remain at this level even after the device was turned off.
CommentThe present single-case study was set to test the potential effects of Forbrain® on voice production, so that it could have any clinical relevance as potential treatment of stuttering as an AAF device. To test for these potential effects, a time-series design was implemented where the participant's voice was recorded while he was reading aloud (in isolation) across three different experimental stages (Baseline, Test, Post-test), and six different quantitative parameters typically used in voice quality studies were calculated (Maryn et al., 2010; Maryn & Weenink, 2015). Data was analyzed by means of quantitative statistical methods suited for single-case studies (Manolov et al., 2014; Shadish, Hedges, Pustejovsky, Boyajian, et al., 2014; Shadish, Hedges & Pustejovsky, 2014). The results obtained revealed compelling significant effects on voice production.
Specifically, we found that both tLTAS and CPPS were significantly affected by Forbrain® in a manner that can be considered specific and transient. Indeed, compared to a baseline reading period where Forbrain® was in off mode, tLTAS was increased when Forbrain® was turned on during the test phase, whereas it returned to baseline level when the device was set back off. In a similar vein, CPPS was increased after a period of 14min using Forbrain®, compared to a baseline level. CPPS is a measure of the degree of harmony in a voice sample, so that it is larger when the voice signal is more periodic, and has been considered to indicate voice quality, particularly, breathiness (Heman-Ackah et al., 2002; Hillenbrand & Houde, 1996; Maryn et al., 2010). The results on CPPS showed no effect when turning Forbrain® one in the test phase, but revealed a large surge when the device was turned off in the Post-test (Fig. 1). These results indicate a perturbation of voice breathiness with the use of Forbrain®. Whether this can be considered as an undesired effect of a potential fluency treatment is discussed next in the light of the results obtained for tLTAS. tLTAS provides a measure that captures the average frequency distribution of the sound energy in a continuous speech sample (Maryn et al., 2010; Vaňková & Skarnitzl, 2014). It has been suggested that strong resonant voices present less differences between the strong and weak regions of the voice spectrum, while poor fluid voices present larger differences, and poor speaking voices have relatively lower sound level in the mid frequency range (1–3kHz), while glottal closing speed has been related with less tilting slope of LTAS (Leino, 2009). Results regarding tLTAS revealed a strong transient effect of Forbrain®, with voice raising its strength and becoming more fluid during the test phase (Forbrain® on; significant differences between Baseline and Test), to recover baseline levels when it was turned off (significant differences between Test and Post-test). This pattern of results, with effects observed solely on two of the six measurements and consisting on a effective change taking place during the phase in which the device was turned on, can be considered specific and transient. Specific because effects occur on two voice parameters formerly observed to be affected by Forbrain® in a sample of healthy volunteers with no personal nor family history of speech and language disorders (Escera et al., 2018); transient because they were circumscribed to the time moments in which the device was active. This is clinically very relevant, as it supports using Forbrain® as a device, one providing a form of AAF, that can have a direct impact in the speech performance of it stuttering users. Of course, future studies carried out on a larger sample of persons who stutter and implementing the appropriate randomized blind case-control designs should validate this initial observations.
Whether the two effects of Forbrain® on voice quality observed here are in apparent contradiction is discussed next. Indeed, the effects on CPPS, which reflects voice harmony, suggest reduced voice breathiness with the use of Forbrain®, whereas the effects on tLTAS, which is thought to reflect voice robustness, indicate strengthening of the voice during Forbrain® use. This apparent contradiction is reconcilable in the context of the phono-articulatory loop, which features the existence of two parallel premotor systems for speech production (Ritto, Costa, et al., 2016), and supports Forbrain@ in fact as a device of AAF. Indeed, the sensory processing is altered as a consequence of motor adaptation to altered visual, somatosensory and auditory feedback (Ostry & Gribble, 2016), and conversely, motor output is fine-grained adjusted as a consequence of distorted sensory input (Hahnloser & Narula, 2017). This is in line with the so-called corollary discharge view of motor control, according to which the motor (e.g., vocal) system sends an efferent copy or corollary discharge of the sound it aims producing, so that the encoding of the auditory input resulting from the self-produced sounds is attenuated in the auditory system (Scott, 2013; Wolpert et al., 1995). When the received input does not match the efferent copy of the motor command, a prediction error is generated (Hahnloser & Narula, 2017) that forces a system readjustment. The results obtained here with Forbrain® fit well with this proposal. Indeed, the effects observed on CPPS suggesting reduced voice harmony support a perturbation of voice control caused by the altered feedback of the ongoing speech fed to the model. In turn, the parallel increased voice strength during Forbrain®, as supported by the results on tLTAS, would indicate an attempt of the audio-vocal loop to compensate for the voice perturbation caused by the altered feedback.
Whether the results obtained in the present study are relevant and potentially useful from a clinical viewpoint, several limitations need to be taken into account. First, it should be mentioned that the duration of the study phases was not equal, with a longer phase for the use of the device compared to the baseline and post-treatment phases. Yet, this was chosen to optimize the session's durations while at the same time maximizing the time using the device. Another limitation is that the design did not follow the optimal conditions to estimate the d-statistic, which require that no time trends are present in the baseline, that the treatment effects are constant across sessions and that the outcome measures are normally distributed (Manolov et al., 2014; Shadish, Hedges, Pustejovsky, Boyajian, et al., 2014; Shadish, Hedges & Pustejovsky, 2014). Given the exploratory nature of this study, and the fact that this is the first attempt to use Forbrain® in a single case study in a person who stutters, we could only assume these requirements. In general, single-case designs are thought to convey internal and external validity issues (Kratochwill et al., 2010), and ours, as a n=1 design on the effects of Forbrain® on a person who stutters cannot escape such a general criticism. Future studies using more stringent controls, either in single-case or group designs should corroborate our findings.
ConclusionsThe present single-case study on an adult who stutters was addressed to investigate, in an objective manner, whether the use of a new commercial device announced to provide AAF, namely Forbrain® (Soundev Ltd, Luxemburg), would have any observable effect on the speaker's voice. After quantitative analyses of different voice parameters retrieved during reading aloud, and statistical tests suited for single-case studies, it was found that turning the device on induced observable changes in voice quality, specifically, a reduction in voice harmony paralleled by a strengthening of voice robustness. The present results support the role of Forbrain® in improving speech, and suggest its role as a potential tool in improving speech fluency in people who stutter. Further, the present study has direct clinical implications, as wearing the device in on mode immediately affects the voice quality of its users. Future studies should be undertaken on a larger sample of stuttering participants, including a control group of adults that do not stutter, and complementing the objective measurements of voice quality with more clinically relevant assessment of both speech utterances and subjective measures.
Author contributionsNGC and CE conceived the design. FLC performed the research. FLC analyzed the data. FLC and CE interpreted the results. FLC, NGC and CE wrote the manuscript.
Conflict of interestThis study was sponsored by Sound for Life Ltd (Soundev). However, the company was not involved: in the study design; in the collection, analysis and interpretation of the data; in the writing of the report; and in the decision to submit the paper for publication. Solely the authors had full access to all data in this study, and the corresponding author takes complete responsibility for the integrity of the data and the accuracy of the data analysis. None of the authors has any private including financial interest in Soundev for Life Ltd (Soundev).
The research received funds partially from the Catalan Government (SGR2017-974), the Spanish Ministry of Economy and Knowledge (PSI2015-63663-P-MINECO/FEDER) and the ICREA Academia Distinguished Professorship awarded to CE.
