


The Remoralization Scale (RS) was developed in order to measure an individual's state in terms of how the person perceives him or herself in relation to his/her self-concept, self-value, hope, empowerment and positive anticipation. However, there is no data on the psychometric properties of the instrument in a non-clinical population. The aim of this study was to validate a Spanish version of the Remoralization Scale (RS) in a non-clinical sample with a prevention objective and/or the promotion of mental health. The original version of the RS was translated into Spanish and it was applied to a non-clinical sample of 1443 university students in Argentina (18–25 years old). Exploratory and confirmatory factor analyses were performed to study the factorial structure and the validity of the construct. Results suggest that a two factor-model (self-satisfaction and self-concept) results in the best fit for this non-clinical population. The reliability of the total scale and for both sub-scales was moderate to high. Discriminant analysis and contrasting groups analysis showed significant results: the clinical sample and the depression-symptoms sample showed less “remoralization” than the non-clinical sample and a group without depression symptoms, respectively. Results are discussed taking into account previous conceptualizations and studies. In conclusion, the RS was validated for its use in a non-clinical Argentinean population. Regarding its construct validity, a two-factor model with high reliability was obtained.
La Escala de Remoralización (RS) fue desarrollada para medir el estado de un individuo en términos de cómo se percibe a sí mismo con relación a su autoconcepto, autovaloración, esperanza, empoderamiento y anticipación positiva. Sin embargo, no hay datos de propiedades psicométricas en la población no clínica. El objetivo de este estudio fue validar una versión española de la RS en una muestra no clínica con un objetivo de prevención y/o promoción de la salud mental. La versión original de la RS fue traducida al español y se aplicó a una muestra no clínica de 1.443 estudiantes universitarios en Argentina (de 18 a 25 años). Se realizaron estudios de análisis factorial exploratorio y confirmatorio para estudiar la estructura factorial y la validez del constructo. Los resultados indican que un modelo de 2 factores (autosatisfacción y autoconcepto) presenta un mejor ajuste para esta población no clínica. La consistencia interna de la escala total y de ambas subescalas fue de moderada a alta. Los análisis discriminantes y análisis de grupos contrastados fueron significativos: la muestra clínica y sujetos con síntomas de depresión mostraron menos «remoralización» que la muestra no clínica y sujetos sin síntomas depresivos. Los resultados se discutieron teniendo en cuenta conceptualizaciones y estudios previos. En conclusión, la RS fue validada para su uso en una población no clínica de Argentina. Respecto a su validez de constructo, se obtuvo un modelo de 2 factores con una alta confiabilidad.
Research in the area of contemporary psychotherapy has moved from a focus on symptom reduction to other effectiveness outcomes (Vissers, Keijsers, van der Veld, de Jong, & Hutschemaekers, 2010; Dohrenwend, Shrout, Egri, & Mendelsohn, 1980). Some authors have criticized the strong emphasis on symptom reduction in psychotherapy outcome research derived from the medical disease model (Hill & Lambert, 2004; Perkins, 2001). Other researchers have also pointed out that patients expect not only the reduction of symptoms but also the improvement of self-confidence and quality of life (e.g., Levitt, Beutler, & Hill, 2006; Lindfors, Knekt, Virtala, & Laaksonen, 2012).
An important development in the description of the positive effects of psychotherapy besides symptom reduction has been the concept of “demoralization”, and its opposite “remoralization”. Demoralization was introduced by Frank (1974) as a state of mind characterized by the belief of being incapable of solving problems and having a feeling of impotence, isolation and despair. This concept has significance across several psychotherapeutic traditions and approaches in the context of common therapeutic factors (Frank & Frank, 2004; Gelso, 2011). Many years after Frank's first description of demoralization, cognitive therapists introduced the term “remoralization” very much attuned with the goal of cognitive therapy in general (Vissers et al., 2010; Howard, Lueger, Maling, & Martinovich, 1993; Slavney, 1999). Remoralization implies a process of restoration of a person's morale, related to an improvement of self-esteem, self-value and self-concept, resulting in higher expectations and self-perceived power, positive anticipation, and active hope (Howard et al., 1993). In addition, remoralization is related to a sense of inner control and restored hope (Kuyken, 2004). Howard et al. (1993) state that remoralization could be the first step in the process of therapeutic change.
A related concept, “learned helplessness”, was proposed by Seligman (1998). “Learned helplessness was defined as a conditioned attributional state of perceived absence of control over a situation that could be overcome” (Robinson, Kissane, Brooker, & Burne, 2014, p. 3). Seligman (1998) states that a global and stable attribution for failure will lead to long-term generalized helplessness, and that internal attributions will intensify these effects. In this context, remoralization is a necessary process in order to reach a sense of active hope.
A large series of studies have distinguished changes in remoralization independently from symptom reduction (Callahan, Swift, & Hynan, 2006; Grissom, Lyons, & Lutz, 2002; Hilsenroth, Ackerman, & Blagys, 2001; Howard et al., 1993; Lutz, Lowry, Kopta, Einstein, & Howard, 2001, Lutz, Martinovich, & Howard, 1999). However, these studies did not focus on the relationship between both outcomes (Vissers et al., 2010). Therefore, further research needs to incorporate remoralization as a valuable component of the assessment of treatment outcome, as a generic therapeutic factor (Vissers et al., 2010). Moreover, the measurement of remoralization could be useful in the mental health area in general, allowing an early warning system for health promotion and mental health promotion in educational, workplace, and social settings. Although remoralization has been discussed in the psychotherapeutic literature, the development of reliable and valid outcome measures, not only for clinical area but also for health field, still requires further efforts.
A first measure of remoralization as a brief self-report instrument was developed for mental health-care patients in The Netherlands (Vissers et al., 2010). In that context, the goal was to develop an easy-to-use self-report measure of the patient's morale at different times of the treatment process. The morale involved the self-perception regarding his/her self-concept, self-value, hope, empowerment and positive anticipation (Vissers et al., 2010). It was first administered to a clinical population, in order to explore its correlation with other depression measures.
This original version of the Remoralization Scale (RS) was based on fundamental theoretical concepts that the literature has shown to be related to a state of demoralization when this state is measured with the various corresponding instruments: (1) self-esteem using items of the Rosenberg Self-Esteem Scale (Rosenberg, 1965); (2) personal empowerment and sense of mastery considering the Empowerment Scale (Rogers, Chamberlin, Ellison, & Crean, 1997); (3) feelings of competence applying the adapted Dutch version of the General Self-efficacy Scale (Bosscher, Smit, & Kempen, 1997; Sherer et al., 1982); (4) optimism using the Optimism Subscale from the Positive Outcome Scale (Appelo, 2005) and sense of inner control, via the Autonomy Subscale also from the Positive Outcome Scale; and (5) hope by the State Hope Scale (Snyder, Sympson, Ybasco, Borders, Babyak, & Higgins, 1996). A unidimensional structure was found through exploratory and confirmatory factorial analyses by the authors, suggesting that this original version of the RS measures a single concept. This single structure was confirmed for both patients and non-patients and it has been shown to have very good psychometric properties (for a more detailed description of the procedures and results see Vissers et al., 2010). The results suggest that patients do not interpret all these concepts described in the literature as highly different. In addition, this previous finding supports the hypothesis about a common state, namely remoralization that could be used across a variety of treatments to measure beneficial effects other than symptom reduction (Vissers et al., 2010; Howard et al., 1993).
The aim of the present study is to validate a Spanish version of the English version of the Remoralization Scale developed by Vissers et al. (2010), in a non-clinical sample from Argentina. Since this concept is so relevant to mental health in general, as in Frank's conceptualization of common therapeutic factors, it would be interesting to assess its psychometric properties including its reliability, as well as its discriminative and construct validity in a non-clinical sample with the objective of emphasizing prevention and/or promotion of mental health. Given the applicability of the construct in the general population, and not only in mental health patients, this would allow us to utilize the instrument in different settings in the future (e.g. educational and epidemiology areas).
MethodParticipantsA non-clinical sample of 1443 undergraduate students, females (55.1%), 18–25 years old (M=20.58 years old, SD=3.915), from middle and high socio-economic level, attending a private university in the city of Buenos Aires, Argentina, participated in this study. A clinical sample of 150 patients (males=58.7%), 18–65 years of age (25–50 years old=52%), from middle socio economic level, mostly with personality disorders, was used. The exclusion criterion was patients who suffered from depression as a primary diagnosis because a reduction of symptoms in these patients could be erroneously attributed to an improvement in remoralization (Vissers et al., 2010).
InstrumentsA local Spanish translation of the English version of the RS (Vissers et al., 2010) was used. The English version of the RS is composed of 12 items with a 4-point Likert scale (from “totally disagree” to “totally agree”), with self-perception items such as “I am in control of my life”. This version has shown very good internal consistency (Cronbach's α=.92) and test–retest reliability (.89; p<.01), with a unidimensional structure, a good construct validity and discriminative validity both for patients and non-patients, and sensitivity to therapeutic change (Vissers et al., 2010).
The SMU Health Questionnaire (SMU-HQ) was applied to measure symptoms of depression. This instrument assesses a broad range of health problems involving 63 items regarding symptoms and complaints, minor illnesses, and more serious and chronic health problems (Cronbach's α=.71). In the SMU-HQ, subjects have to check any health problem experienced during the last year. In this study, only the depression item was considered as an external criterion.
ProcedureAs a first step, all the items of the RS (English version, 12 items) were translated into Spanish by two independent bilingual professional translators. They agreed in 90% of the items in their initial translation. A second step followed in which the translators reached consensus on the remaining 10% of the items. This version was administered to a small sample of students to evaluate several aspects of the adapted instrument, including semantic comprehension, linguistic characteristics, and cultural elements. A final version of the reviewed 12 items was obtained. Each item was presented in a Likert-type scale ranging from 1 (totally disagree) to 4 (totally agree). In addition, the SMU Health Questionnaire (SMU-HQ) was applied to measure symptoms of depression.
Regarding the administration of both instruments to the non-clinical sample informed consent was obtained following the current APA code of conduct guidelines. Students were informed on the purpose of the research, expected duration, their right to decline to participate, and to withdraw from the research once participation had begun. Those students who agreed to participate were asked to complete a socio-demographic questionnaire, the RS and the SMU-HQ, administered under supervision as a single package of survey instruments during a lab session at university.
The clinical sample was recruited of several mental health centers from Buenos Aires city, at the beginning of the treatment by two researchers of the team. Patients signed an informed consent before their participation. The patients were asked to answer individually the Spanish version of RS by a pencil and paper format.
Statistical analysisFirstly, an exploratory factorial analysis (EFA) was conducted on the set of 12 items (n=605; Female: 53.5%; M=20 years old, SD=3.915) using the Maximum Likelihood extraction method, with a Promax rotation to determine the number of factors obtained taking into account the common variance. The correlation matrix and anti-image correlation matrix were studied. The Kaiser–Meyer–Olkin adequacy of sample measure (KMO) and Bartlett's test of sphericity were calculated in order to assess the possibility of a factor analysis of items, and both measures confirmed the adequacy of the data for the analysis. This EFA yielded a model with two factors.
In addition, a confirmatory factorial analyses (CFA) was carried out with a new sample of students (n=838; female: 56.3%; M=20 years old, SD=3.915) in order to test the two-factor model previously obtained in the EFA, using the AMOS Graphics 16.0 program. A Comparative Fit Index (CFI) and Normed Fit Index (NFI) were calculated to analyze the goodness-of-fit level of the model. In addition, the Root Mean Square Error of approximation (RMSEA) was calculated to identify the degree of error.
In order to study the capacity of the RS to differentiate between subjects with and without depression symptoms, Discriminant Analyses was carried out, considering the total score of RS (within the non-clinical sample). In addition, a contrasting groups analysis was carried out using a clinical sample to provide evidence of discriminant validity. In order to obtain equivalent groups, a random sample of 15% was selected from the non-clinical sample (n=208).
ResultsStudy 1: Exploratory factorial analysis (EFA)The EFA involved 605 students at a private university from Argentina. It was conducted on the set of 12 items using a maximum likelihood extraction method to determine the number of factors, and a Promax rotation.
The correlation matrix showed satisfactory values (diagonal of anti-image matrix between .883 and .942 with a partial correlation values nearing 0). The KMO=.911 and test of sphericity=2394.906; p=.000, showed the adequacy of the data.
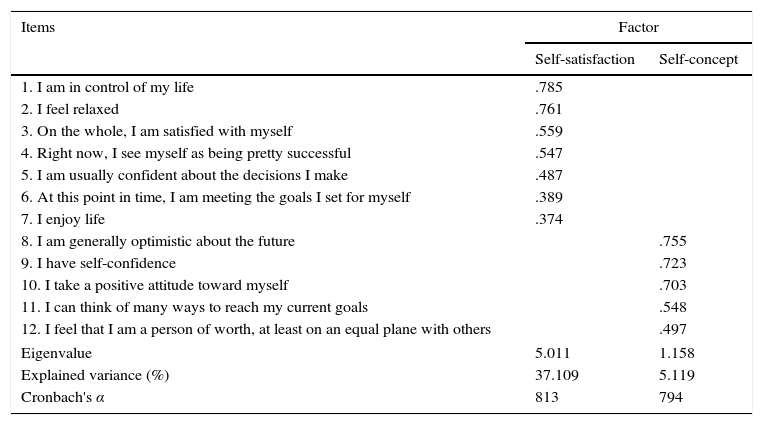
The Scree Plot and eigenvalues equal or greater than 1 were used as the criteria to determine the number of factors. The results obtained indicated the extraction of two factors. The two factors explain 42.23% of the variance of the RS scores. The first factor explains 37.11% of the variance; and the second factor explains 5.12% of the variance. Factor 1 involves items related to self-satisfaction (e.g. “I am in control of my life”, “I feel relaxed”, etc.). Factor 2 includes items more related to a sense of the self or self-concept (e.g. “I take a positive attitude toward myself”, “I have self-confidence”). Both factors were interpreted using an empirical criterion based on items with weights equal to or greater than .40 (Table 1). The correlation between both factors was moderate (r=.703; p=.001).
Factor analysis of the Remoralization Scale (Promax solution).
| Items | Factor | |
|---|---|---|
| Self-satisfaction | Self-concept | |
| 1. I am in control of my life | .785 | |
| 2. I feel relaxed | .761 | |
| 3. On the whole, I am satisfied with myself | .559 | |
| 4. Right now, I see myself as being pretty successful | .547 | |
| 5. I am usually confident about the decisions I make | .487 | |
| 6. At this point in time, I am meeting the goals I set for myself | .389 | |
| 7. I enjoy life | .374 | |
| 8. I am generally optimistic about the future | .755 | |
| 9. I have self-confidence | .723 | |
| 10. I take a positive attitude toward myself | .703 | |
| 11. I can think of many ways to reach my current goals | .548 | |
| 12. I feel that I am a person of worth, at least on an equal plane with others | .497 | |
| Eigenvalue | 5.011 | 1.158 |
| Explained variance (%) | 37.109 | 5.119 |
| Cronbach's α | 813 | 794 |
The internal consistency of the total scale was evaluated with Cronbach's alpha (α=.871, n=605). For Factor I (self-satisfaction) Cronbach's alpha was .813 (n=606, number of items=7). Factor II (self-concept) showed a Cronbach's alpha of .794 (n=605; number of items=5). In both sub-scales, all items contributed positively to the reliability of the scales (Table 1).
Study 2: Confirmatory factor analysisA total of 838 university students (all different from the sample in Study 1) participated in a second study in which the RS was administered in order to carry out a confirmatory factor analyses (CFA). The CFA was conducted on the same set of 12 items of the total RS instrument, using the AMOS 16.0 software, to assess the fit of the factors found in the initial EFA to the data in the second sample. Three measures of model fit were considered: the model chi-square, the root mean squared error of approximation (RMSEA), and the fit index (CFI).
The two-factor model shows a very good fit to the data, as is shown by the indices of overall fit: the model chi-square, the root mean squared error of approximation (RMSEA), the Comparative Fit Index (CFI), and the Normed Fit Index (NFI).
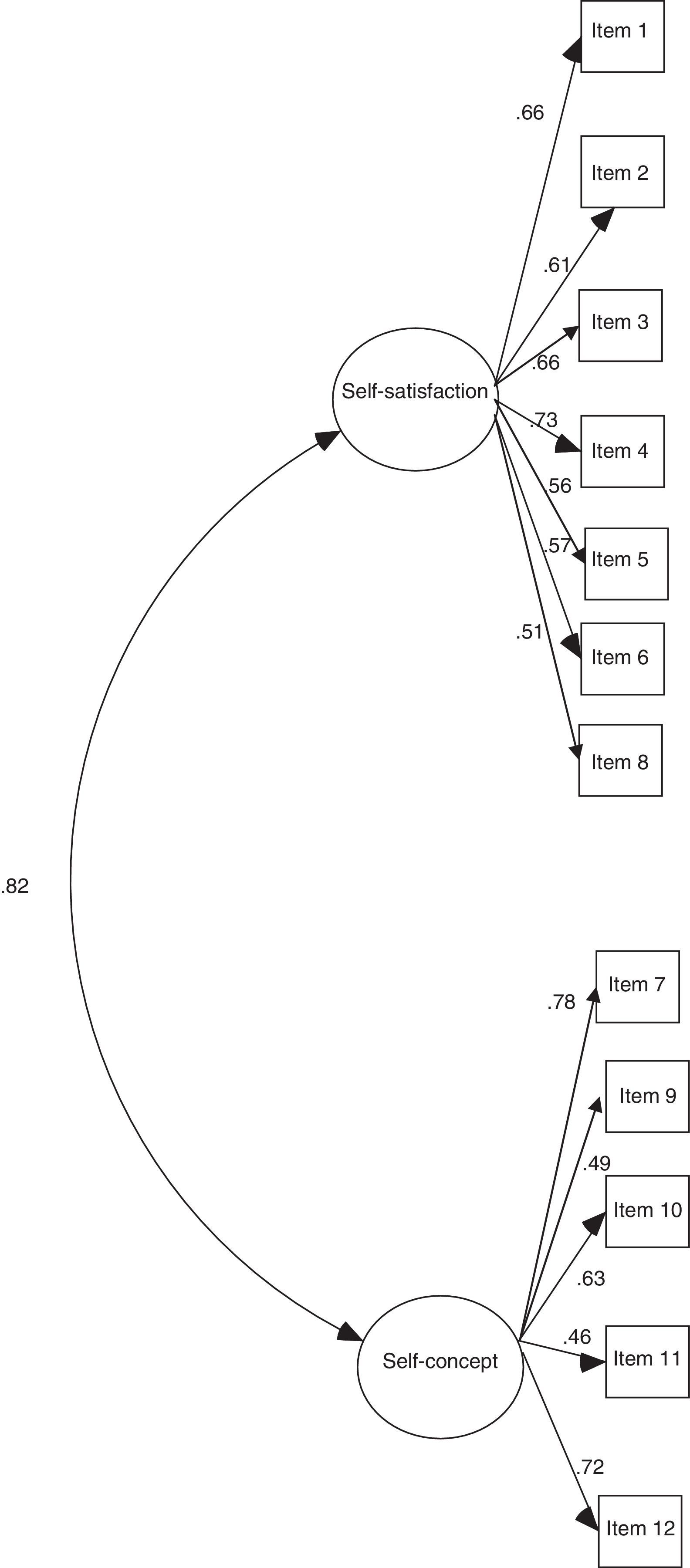
Although the chi-square was significant, it is expected given the large sample size (Anderson & Gerbing, 1988; Hair, Anderson, Tatham, & Black, 1998) (χ2=249.301; df=53; p=.001). The other measures of fit performed confirmed a very good fit: the CFI and the NFI were greater than .90 (CFI=.935 and NFI=.92), and the RMSEA (.067) was not greater than the cut off value of .08; all confirming good fit of the model to the data. In addition, a one-factor model was examined in order to compare to the structure obtained in a previous study (Vissers et al., 2010). This model did not show a good fit to the data (χ2=372.443; df=p=.000; CFI=.89; NFI=.880; RMSEA=.084) (Table 2). The two-factor model showed a much better fit to the data than the one-factor model (Fig. 1).
Fit indices for the two models.
| Models | χ2 | df | p | CFI | NFI | RMSEA | Parameters estimated |
|---|---|---|---|---|---|---|---|
| Sample (n=838) | |||||||
| Two factor model | 249.30 | 53 | .000 | .93 | .92 | .067 | 37 |
| One factor model | 372.44 | 54 | .000 | .89 | .88 | .084 | 24 |
Note: Values higher than 0.90 for CIF and NFI, and RMSA below 0.08 indicate good fit. Best fit model is in bold.

In order to study the capacity of the RS to differentiate between subjects with and without depression symptoms, Discriminant Analyses was carried out, considering the total score of RS. One of the restrictions of this analysis has to do with the assumption of equality of covariance matrices that, in this case, is not violated (Box's M=.450, F=.446, p=.504). The total score of the RS was able to discriminate between the two groups composed by the clinical and the non-clinical samples. The squared canonical correlation (CR2) gives the amount of variation between the groups that is explained by the discriminating variables, which in this case was low (Wilk's λ=.948, χ2=37.986, df=1, p=.001, CR2=.227).
ANOVA results have shown that subjects who have suffered some depression symptoms during the last year showed significantly less remoralization (M=32.17, SD=5.66) than the subjects without these kind of symptoms (M=37.24, SD=4.94) (F (1,655)=33.400; p<.001, η2=.049; 1−β=1.00).
In order to add discriminant validity to the scale, a contrasting groups analysis was carried out using a clinical sample (n=150), mostly composed by personality disorders. ANOVA results showed a lower total score of RS for the clinical sample (M=32.04, SD=8.132) compared to the non-clinical sample (M=36.30, SD=5.176) (F (1,337)=34.757; p<.001, η2=.093; 1−β=1.00).
DiscussionThe present study is based on an outcome measure that has been developed from several highly correlated psychological concepts: self-esteem, empowerment, self-efficacy, optimism, sense of inner control, and hope (Vissers et al., 2010). The objective of this previous study was to obtain a single measure of a common state underpinning a successful psychotherapy: remoralization (Vissers et al., 2010). Data confirmed that all these concepts have a common factor both in patients and non-patients (Vissers et al., 2010). However, the present validation offers an abridged and adapted version (in Spanish) of the RS, comprising 12 items and identifying two factors of this construct that were named self-satisfaction and self-concept, respectively. Although the correlation among both factors was high, a two-factor model achieved a better fit to the data than a one-factor model in this population.
The one-dimensional structure found in the validation of the English version of the RS, could not be replicated in this population. The original version of the RS also found factorial invariance between both clinical and non-clinical samples concluding that both groups understand the items similarly (Vissers et al., 2010). Instead, a two-factor model seems to be a more appropriate structure of this construct in a non-clinical population from Argentina. Socio-cultural differences and specific characteristics of this non-clinical sample (e.g. university students) could have influenced this result. Further research is necessary to understand this difference. In addition, multigroup confirmatory analyses should be carried out to provide further support for this finding using different samples from Argentina.
According to this study, Remoralization has two facets which could be identified in the self-perception of non-patients: (a) an emotional and situational component, and (b) a more general cognitive self-concept. Previous conceptualizations of “Demoralization” have involved two dimensions: distress and subjective incompetence (de Figueiredo & Frank, 1982). The first factor found in this study (self-satisfaction) could be related to the opposite of “distress” described as the incapacity to adapt to stressful events; the distress is characterized by feelings of anger, discouragement and sadness (de Figueiredo & Frank, 1982). On the other hand, the second factor in this version of the RS focuses on the opposite of subjective incompetence. This is supported by a previous psychometric study that has shown a strong negative correlation between the RS and the Demoralization Scale (DS) of Kissane et al., 2004 (Vissers et al., 2010). Moreover, the process of remoralization in the context of psychotherapy requires addressing the issue of subjective incompetence, but it also involves the decrease of the distress element, as it has been pointed out previously (de Figueiredo, 2007).
Although we cannot infer from this research that in clinical and non-clinical populations Remoralization is associated to self-satisfaction and self-concept, this is an interesting and relevant possibility that should be studied in further research. Remoralization is the enhancement of subjective well-being and it could be reached early in treatment (Howard et al., 1993). However, as shown in this study, these aspects could be better differentiated in a non-clinical sample than in a clinical sample. In order to be able to discriminate self-concept from self-satisfaction, subjects need to differentiate properly negative from positive expectations. For instance, a negative self-concept does not necessarily imply non-self-satisfaction and vice versa. Therefore, we can hypothesize that non-clinical populations can tolerate frustration (negative self-satisfaction) without altering self-concept. The reverse can also be true, for those incapable of certain things (negative self-concept) it does not necessarily follow that they are not able to obtain satisfaction in other things (negative self-satisfaction). In addition, healthy subjects could be unable to adapt to specific stressful events, feeling less control of him/herself (or another negative emotions), but at the same time they could also have a positive general self-concept. This result may be due to the use of more adaptive than maladaptive strategies to regulate negative emotions for both self-regulation and interpersonal regulation (Oberst, Company, Sánchez, Oriol-Granado, & Páez, 2013). These adaptive strategies allow a perception of an improvement in the achievement of adaptive goals and self-concept (functionality) (Oberst et al., 2013).
The second dimension of Remoralization found in this study (self-concept) is an important cognitive resource that could be used as a discriminating factor in the process of therapeutic change. Further studies, in different clinical samples, should explore whether the two-factor model underlying the RS could help psychotherapists to achieve a more discriminating evaluation of the changes in one or both dimensions, from a general subjective well-being at the beginning of psychotherapy, to a more discriminating self-assessment in a more advanced phase of treatment. This is coherent with the cognitive based conceptualization of the relevance of belief systems in clinical and non-clinical populations (Beck, 2010). In the clinical tradition, within the cognitive therapy perspective, the belief system bias (either overly positive or overly negative) is considered to support psychopathology symptoms. Depression, for instance, has been largely demonstrated to be associated with negative thinking and negative anticipation of the future (Beck, 1979). Since its first formulations, the concept of moralization (Frank & Frank, 2004) was associated with hope, and hope implies a positive expectation for the future. Within the cognitive psychology tradition, expectations are an essential part of human cognition (Gardner, 1985). It is possible that further studies discriminating clinical and non-clinical populations, may allow us to use this measure in the early detection of psychopathology, and thus be a useful tool in mental health prevention and promotion.
Limitations and conclusionA possible limitation of the present validation study concerns the “convenience sampling” of the “healthy” student population, which could restrict the generalization of the results. In addition, the procedure of data collection in both clinical and non-clinical samples was carried out without assistance by the researcher to preserve the anonymity of the participants. Future research on RS should consider including a broader and random sample of the general population. Another limitation has to do with the absence of other self-concept and demoralization scales to evaluate the concurrent validity of the RS instrument. In addition, given that this is a cross-sectional study design, the predictive validity of the instrument should be further studied. Although test–retest reliability could not be evaluated with this design, the RS showed high internal consistency.
Regarding the factor structure differences found in comparison with the original version, further studies applying multi-group analyses should be carried out comparing non-clinical and clinical samples. In addition, further research on this Spanish version of the RS should examine its discriminating potential between patients and non-patients, and the relationships between symptom reduction and Remoralization in a similar population.
In conclusion, a brief scale to measure Remoralization was validated for its use in a non-clinical Argentinean population, obtaining a two-factor model which has a good fit to this non-clinical sample, contributing to its construct validity. The reliability coefficients found for the Spanish version of the RS were found to be satisfactory. This type of brief outcome measure could provide an important tool both for treatment effects research and for health promotion, beyond a simple symptom-reduction model (Vissers et al., 2016).
This study was supported by UADE (Argentina). The authors gratefully acknowledge to Dolores Blasco, Javier Salgado, Marie De Bellefroid, Hernán Belozo, and Mariano Gianni for their assistance with the test administration.
