


Introducción: Existe poca información que compara características clínicas y tendencias terapéuticas en población mexicana, hispánica y anglosajona, con síndrome coronario agudo sin elevación del ST (SCA SEST).
Métodos: Describimos características clínicas, proceso de atención y evolución hospitalaria en población mexicana, hispánica y anglosajona con SCA SEST, en hospitales mexicanos y americanos. En tres mil cuatrocientos veinticuatro mexicanos, 3 936 hispánicos y 90 280 anglosajones de los registros RENASICA y CRUSADE, se analizaron características basales, uso de recursos, apego a las guías clínicas y mortalidad hospitalaria.
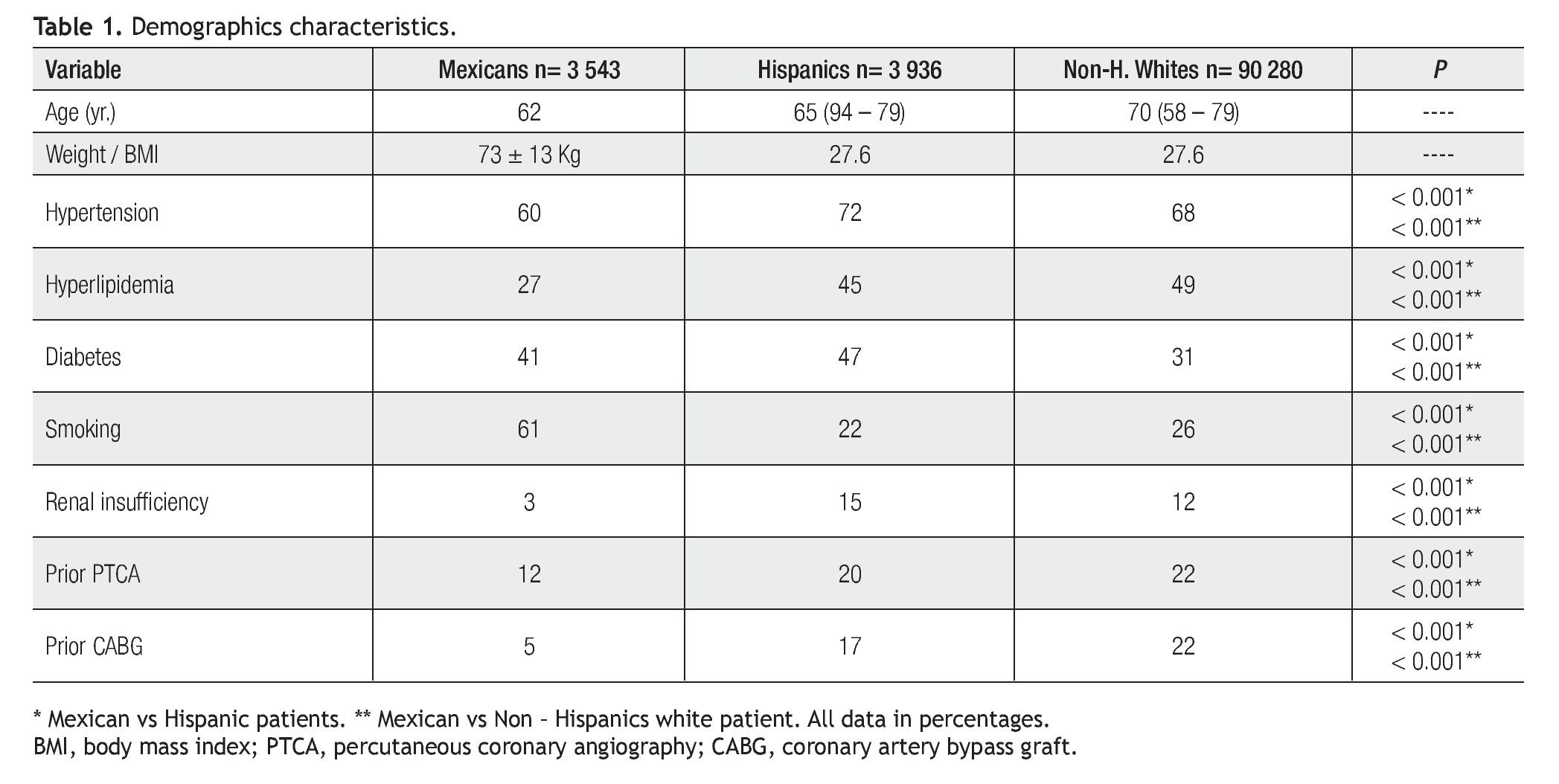
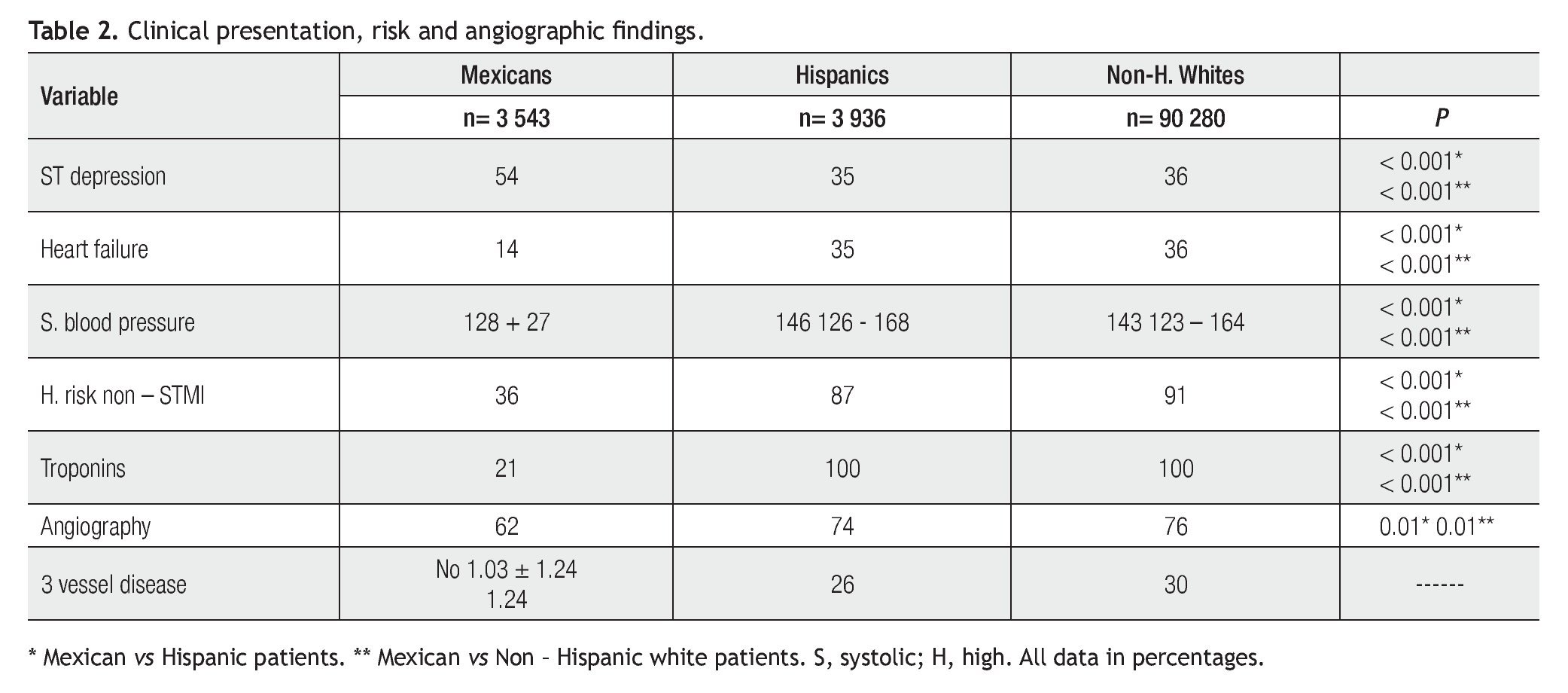
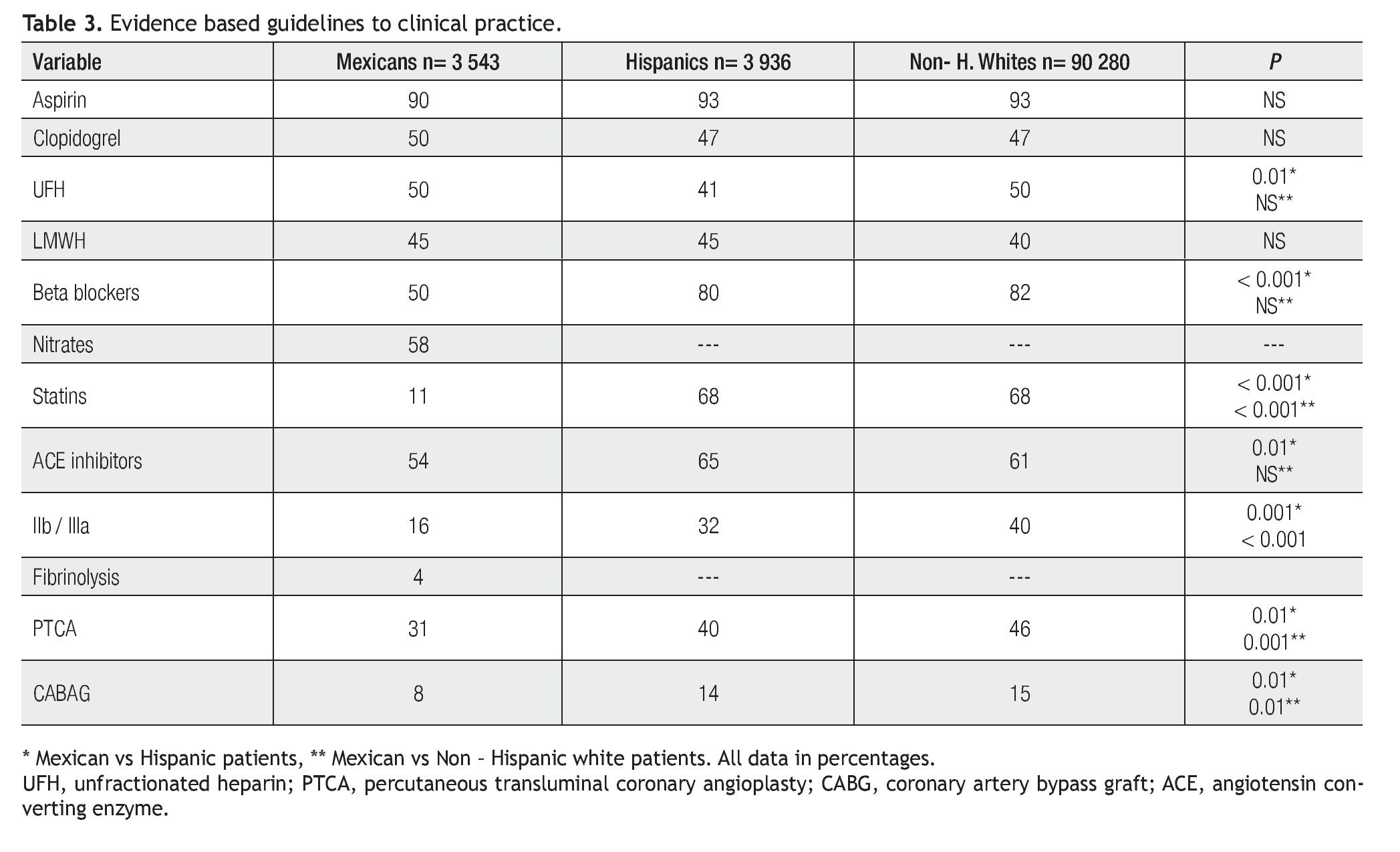
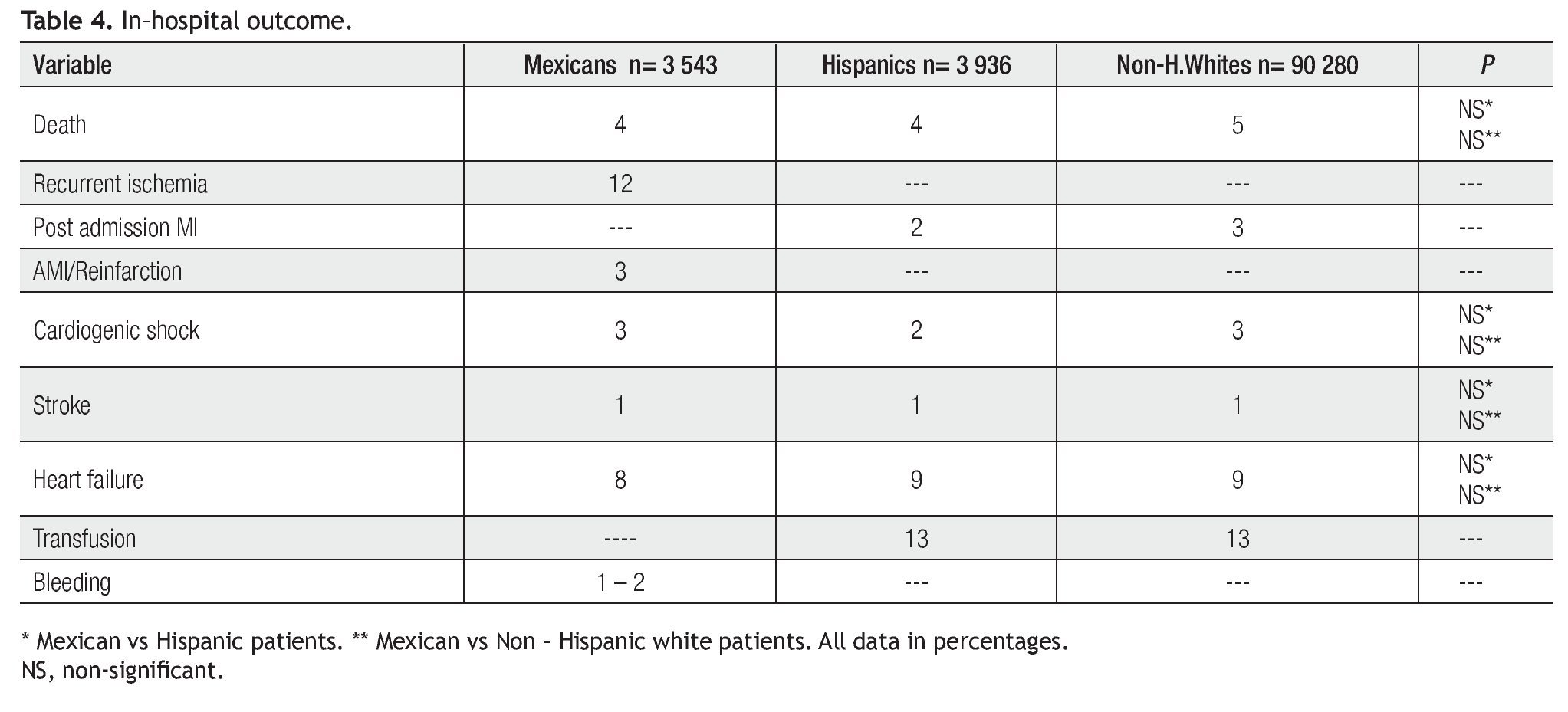
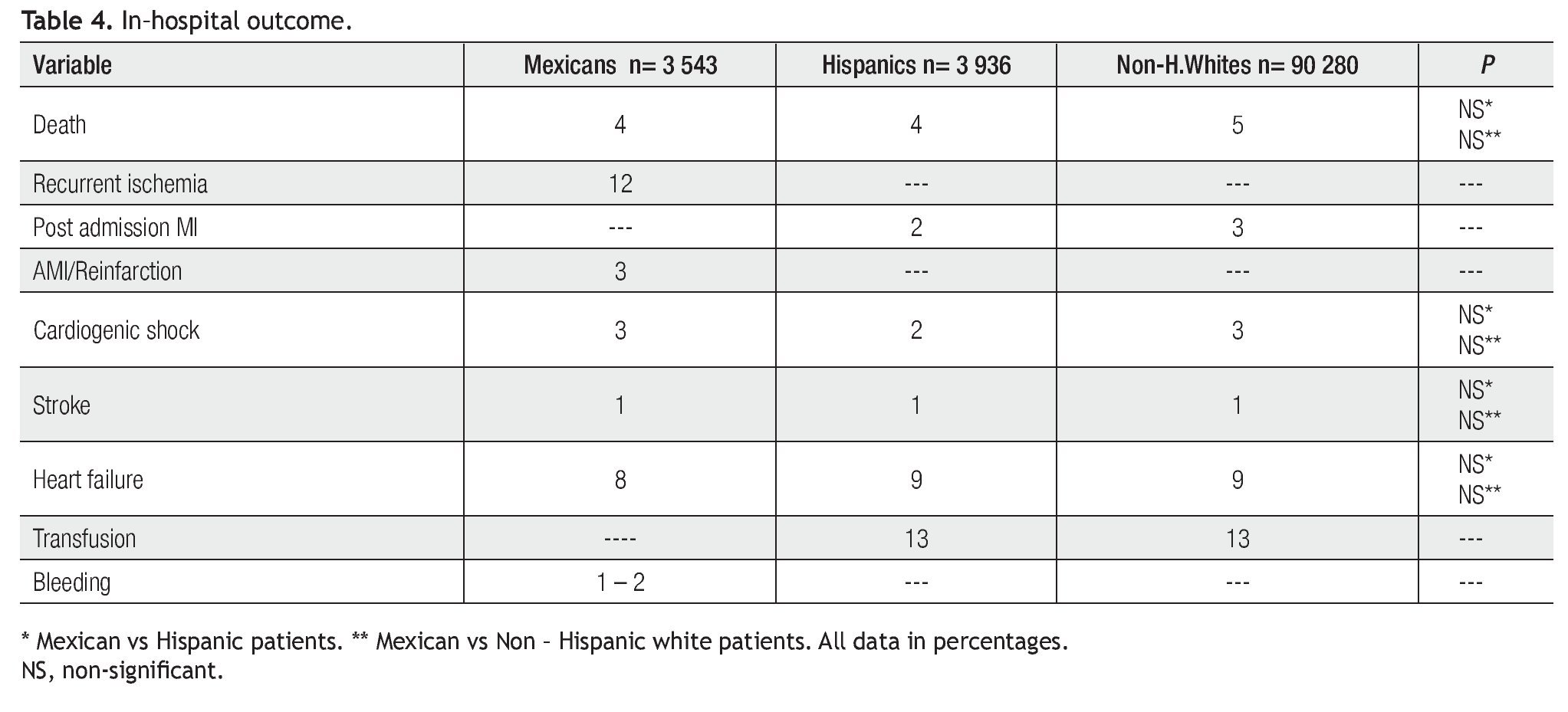
Resultados: Los pacientes mexicanos fueron más jóvenes y con diferente perfil de riesgo cardiovascular, por menor incidencia de hipertensión (p< 0.001), hiperlipidemia (p<0.001), insuficiencia renal (p<0.001) e historia de revascularización (p< 0.001), pero tuvieron mayor historia de tabaquismo (p<0.001) en comparación con hispánicos y anglosajones. La mayor incidencia de diabetes se observó en pacientes hispánicos y mexicanos (p<0.001). En éstos, al ingreso se observó mayor incidencia de desnivel negativo del ST (p<0.001), y menor grado de disfunción ventricular (p<0.001) y uso de troponinas (p<0.001). En relación al apego de las guías clínicas, en prácticamente todos se utilizó aspirina (90%), pero el uso de clopidogrel y heparina no fraccionada o de bajo peso molecular, sólo se utilizó en aproximadamente el 50%. Los pacientes mexicanos recibieron menos inhibidores de la glicoproteínas IIb / IIIa y menos revascularización. A pesar de algunas diferencias clínicas y terapéuticas, la mortalidad cardiovascular fue similar en los tres grupos (mexicanos 4%, hispánicos 4% y anglosajones 5%). En todos los grupos, el apego a las guías clínicas no fue el ideal.
Conclusiones: En un análisis retrospectivo, pacientes mexicanos con un SCA SEST tuvieron diferente perfil de riesgo cardiovascular, presentación clínica y tratamiento hospitalario, que los pacientes hispánicos y anglosajones. Sin embargo, estas diferencias no parecen afectar la mortalidad hospitalaria.
Introduction: Data regarding management characteristics of non-ST elevation acute coronary syndromes (NSTE ACS) in Mexican, Hispanic and Non- Hispanic white patients are scarce.
Methods: We sought to describe the clinical characteristics, process of care, and outcomes of Mexicans, Hispanics and non-Hispanic whites presenting with NSTE ACS at Mexican and US hospitals. We compared baseline characteristics, resource use, clinical practice guidelines (CPGs) compliance and in-hospital mortality among 3 453 Mexicans, 3 936 Hispanics and 90, 280 non-Hispanic whites with NSTE ACS from the RENASICA and CRUSADE registries.
Results: Mexicans were younger with a different cardiovascular risk profile, fewer incidences of hypertension (p<0.001), hiperlipidemia (p<0.001), renal failure (p<0.001) and prior revascularization (p<0.001) but were more likely to be smoking compared with Hispanics and non-Hispanic white populations. Mexicans and Hispanics had a higher incidence of diabetes (p<0.001). At clinical presentation Mexican patients were more likely to have ST depression (p<0.001) but less likely to have left ventricular dysfunction (p<0.001) and troponin stratification (p<0.001). Regarding CPGs compliance, aspirin was used in 90% of patients in all groups, but clopidogrel or unfractionated or low-molecular weight heparin in 50% of patients or less. Mexican patients were less likely to receive glycoprotein IIb/IIIa inhibitors and revascularization. In spite of clinical differences and therapeutic trends, cardiovascular mortality was similar among all groups (Mexicans 4%, Hispanics 4% and non-Hispanic white 5%). In all groups of patients, a poor CPGs compliance was observed.
Conclusions: In a post-hoc analysis, Mexican patients with NSTE ACS had a different cardiovascular risk factor profile and clinical presentation, and less intensive in - hospital treatment than Hispanic and non-Hispanic white patients. However, these differences do not appear to affect in - hospital mortality.
Introduction
Worldwide, acute coronary syndromes (ACS) are estimated to be the leading cause of death and loss of disability- adjusted life years in developing and developed countries.1 Current knowledge about therapeutic and mortality trends in non-ST elevation (NSTE) ACS is largely derived from randomized control clinical trials.2,3 Prospective registries provide a unique opportunity to accurately assess current clinical practice and outcomes, and compare these with other institutions and clinical practice guidelines. These data contribute to an ongoing process of quality assurance, indicating areas where education is necessary.4 RENASICA II5 and CRUSADE6 are contemporaneous high quality clinical registries that could identify in the "real clinical practice" if knowledge from clinical trials is being properly applied in NSTE ACS patients under different health care systems. We analyzed clinical characteristics, process of care, clinical practice guidelines (CPGs) compliance, and in-hospital outcomes among Mexican, Hispanic and non-Hispanic white patients presenting with NSTE ACS.
Methods
In a post - hoc study data from patients enrolled in two contemporaneous registries were analyzed. Objective is to identify clinical characteristics, process of care, resource use, CPGs compliance and in-hospital mortality among Mexican, Hispanic and non-Hispanic white patients at Mexican and United States of America (USA) hospitals. Inclusion: patients enrolled with final diagnosis of NSTE ACS secondary to ischemic heart disease. Design: RENASICA II5 and CRUSADE6 designs have been published previously. In brief: RENASICA II was a prospective and observational registry that aimed to reflect an unbiased and representative population with final diagnosis of ACS secondary to ischemic heart disease to identify diagnosis, stratification and treatment trends. In-hospital outcome was analyzed through major adverse cardiovascular events (MACE) including death, recurrent ischemia, acute myocardial infarction, reinfarction, cardiogenic shock and stroke. Patients were included in the registry if during hospital admission they had high clinical suspicion of ACS: acute ischemia manifestations, with or without ECG changes or necrosis and proven ischemic heart disease by invasive or non-invasive tests. Patients with symptoms precipitated by anemia, hypertension, heart failure, etcetera, were not considered. With or without ST elevation nomenclature was standardized on admission and at discharge. All treatment decisions were taken by the patient's respective physicians. To ensure quality control of registry data the criteria developed by Alpert were applied. An electronic case report form was used.5
CRUSADE6 was a multidisciplinary quality improvement initiative for patients with NSTE ACS across 443 hospitals in the United States. Criteria for enrollment included ischemic symptoms at rest within 24 hours before presentation with high-risk features including ST-segment depression >0.5 mm, transient ST-segment elevation 0.5 to 1.0 mm (lasting for<10 minutes), and/or positive cardiac markers (elevated troponin I or T and/or creatinekinase - MB higher than upper limit of normality). Patient information was collected retrospectively in an anonymous fashion using a three page case report form that captured demographic and clinical characteristics at enrollment, use of evidence-based therapies within 24 hours of presentation, laboratory results, use and timing of coronary angiography and revascularization procedures, discharge medications, and in-hospital clinical outcomes. Contra-indications to therapies given class IA or IB recommendations by the American College of Cardiology/American Heart Association Guidelines were recorded. The institutional review board of each institution approved participation in CRUSADE.6
Definitions
Hispanic patient: term used exclusively in the United States coined without a scientific basis by the Office of Management and Budget in 1978 to standardize data collection among federal agencies. Hispanics are an amalgamation of different cultures and nationalities (Mexican, Puerto Rican, and Cuban), whose origins and race are diverse.7
Acute Coronary Syndrome NSTE
RENASICA II
High - risk: characteristic ischemic chest pain lasting > 20 minutes during the last 48 hours with dynamic or persistent ST depression > 1 mm in 2 consecutive leads or > 3 leads, left ventricular dysfunction, independent of troponin or creatininekinase - MB status.
Low - risk: characteristic ischemic chest pain lasting < 20 minutes in the last 48 hours with negative t waves, non-specific changes or normal ECG, without left ventricular dysfunction and normal biomarkers.5
CRUSADE
High - risk: ischemic symptoms at rest within 24 hours before presentation with risk features including ST depression > 0.5 mm, transient ST elevation of 0.5 to 1.0 mm (lasting for < 10 minutes), and/or positive cardiac markers (elevated troponin I or T and/or creatinekinase - MB higher than upper limit of normal values).6
Statistics
Chi square tests for discrete and two - tailed t tests for continuous variables, Yates corrected chi square and Wilcoxon test were used. As a measure of association odds ratio with 95% confidence interval (CI) was considered. Statistical significance was assumed with p<0.05 level. Data are expressed in percentage, median, mean and SD.
Results
Between December 2002 and November 2003, 8098 Mexican patients were considered in the final report of RENA-SICA II. Of these, 3 543 had NSTE ACS. A total of 76 investigators in 66 primary and tertiary hospitals participated. Regarding the hospitals participating in the registry, 90% (60 hospitals) had active participation, 48% belong to government health system, 39% from private medicine, and 12% were teaching hospitals from other health systems. Hospitals located throughout the country enrolled 52% of the total of patients and those in Mexico City accounted for 48%. Tertiary hospitals with capabilities for coronary arteriography, percutaneous transluminal coronary angioplasty (PTCA) and coronary artery bypass graft (CABG) surgery enrolled 90% of the patients.
Between November 2001 and December 2004, 3 936 Hispanics and 90 280 non-Hispanic whites were enrolled in CRUSADE. The regional distribution of Hispanic enrollment closely paralleled the distribution of the Hispanic population across the USA. Hispanics were treated in hospitals of similar size compared with non-Hispanic whites but were less commonly treated on-site with surgical revascularization capabilities and cared for by a cardiologist. However, Hispanics were more frequently treated at academic facilities compared with non-Hispanic whites.
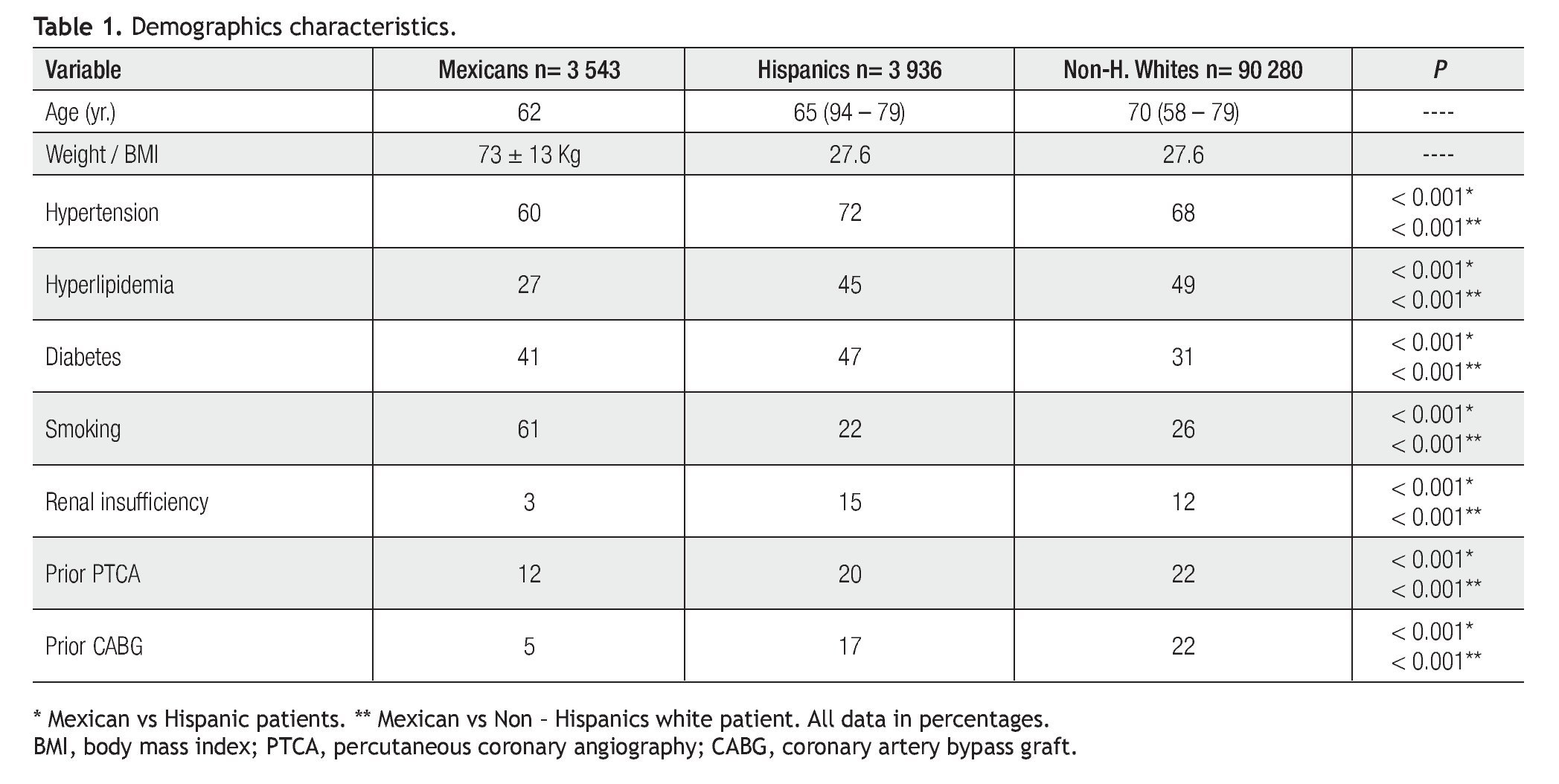
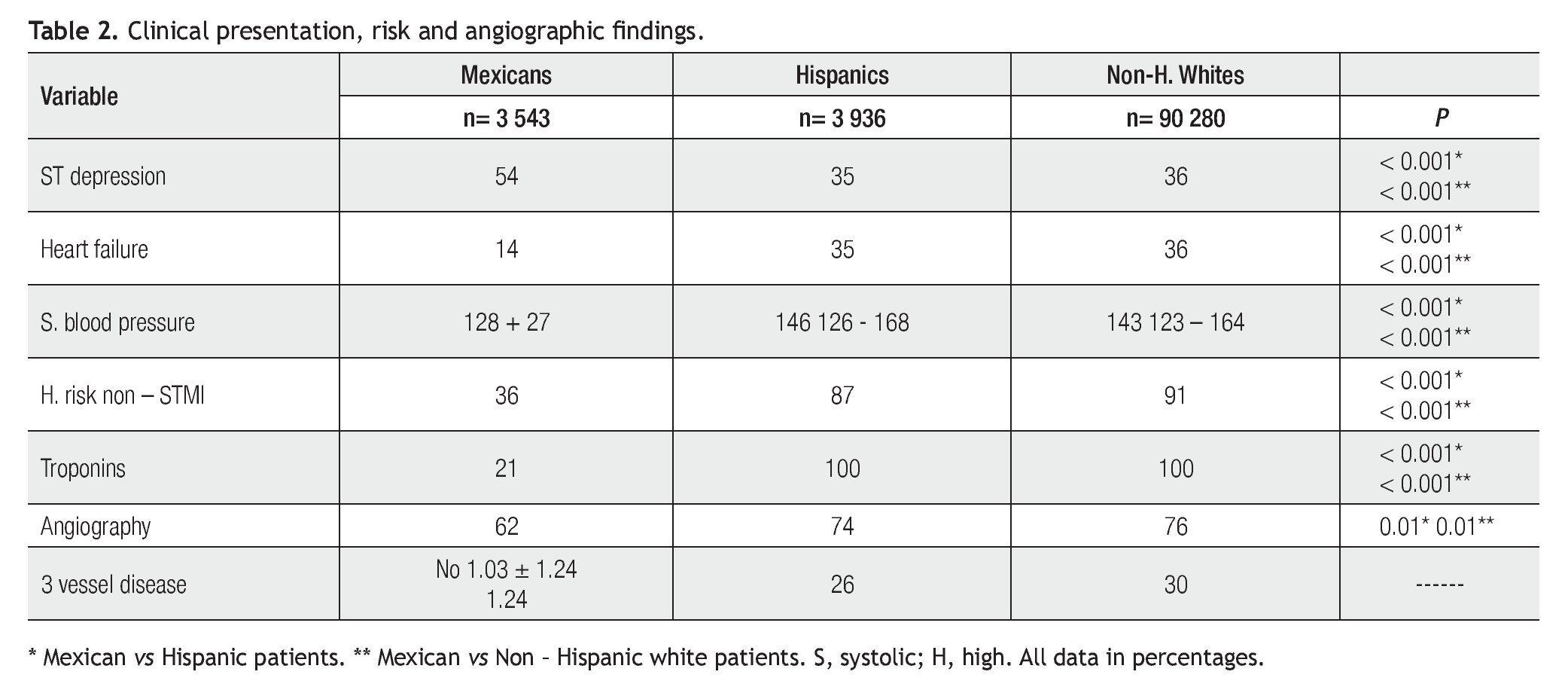
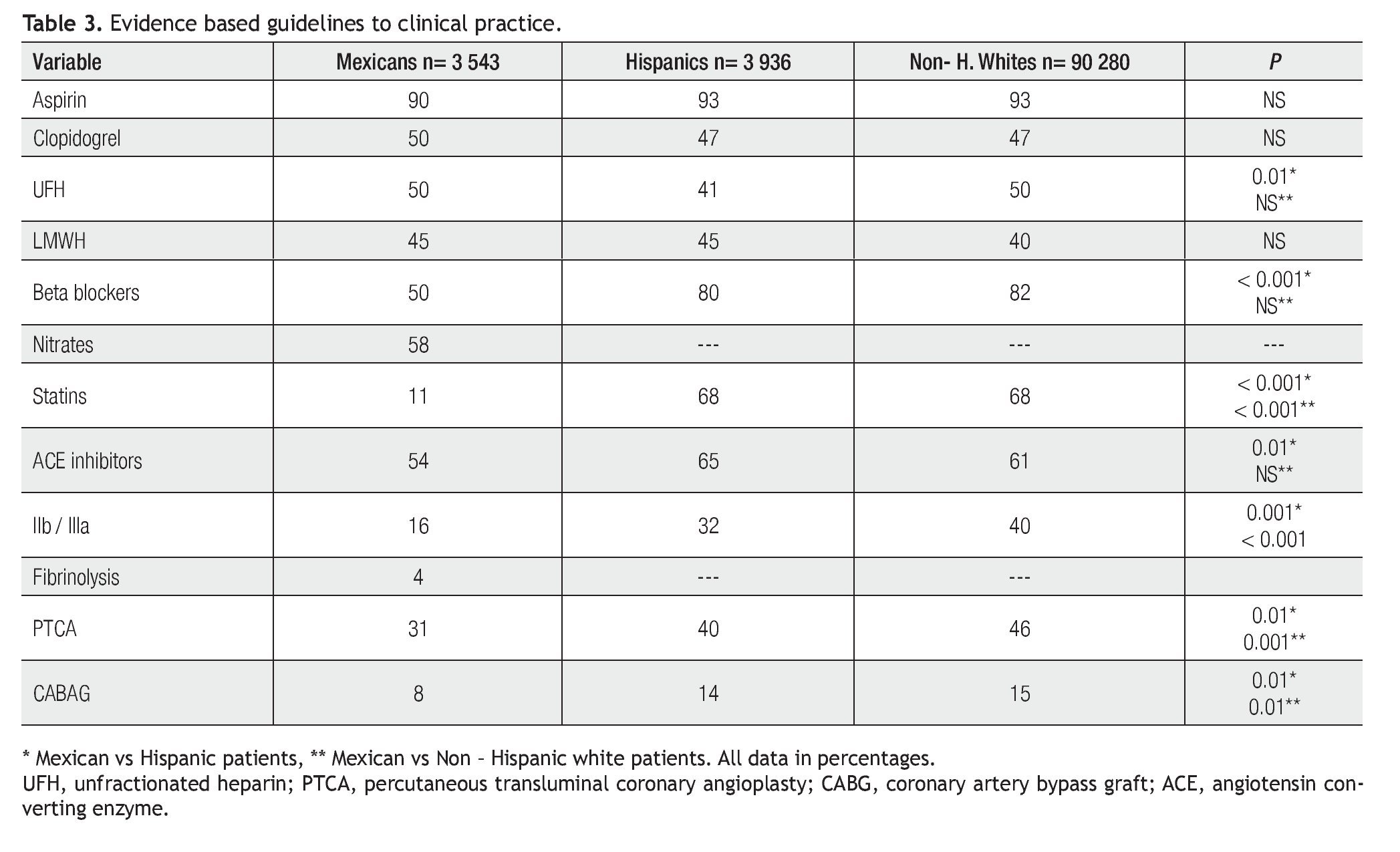
Non-ST elevation ACS Mexican patients were younger with different cardiovascular risk profile, fewer incidences of hypertension (p<0.001), hyperlipidemia (p<0.001), renal failure (p<0.001) and prior revascularization (p<0.001), but were more likely to have diabetes (p<0.001) and to be currently smoking (p<0.001) compared with Hispanics and non-Hispanic white populations (Table 1). At clinical presentation Mexican patients were more likely to had ST depression (p<0.001) but less likely to have left ventricular dysfunction (p<0.001), high-risk (p<0.001), and angiographic (p=0.01) or troponin stratification (p<0.001). All groups had clinical stability (Table 2). Regarding antithrombotic treatment only aspirin was used in according CPGs compliance. Clopidogrel and heparins were used in 50% of patients or less. Mexican patients were less likely to receive glycoprotein IIb / IIIa inhibitors and revascularization (Table 3). In spite of clinical differences and therapeutic trends, in - hospital cardiovascular mortality (Mexicans 4%, Hispanics4% and non-Hispanic whites 5%) and other major cardiovascular adverse events were similar among all groups (Table 4).
Discussion
In our results three relevant findings were identified. First, in the contemporary era of evidence-based medicine, although invasive processes of care probably depend on income capacity, no difference in the in-hospital mortality was observed. Second, Mexican patients had different risk factors and clinical presentation profile than patients living in USA. Third, strategies to improve CPGs compliance have to be implemented in developed and developing countries.
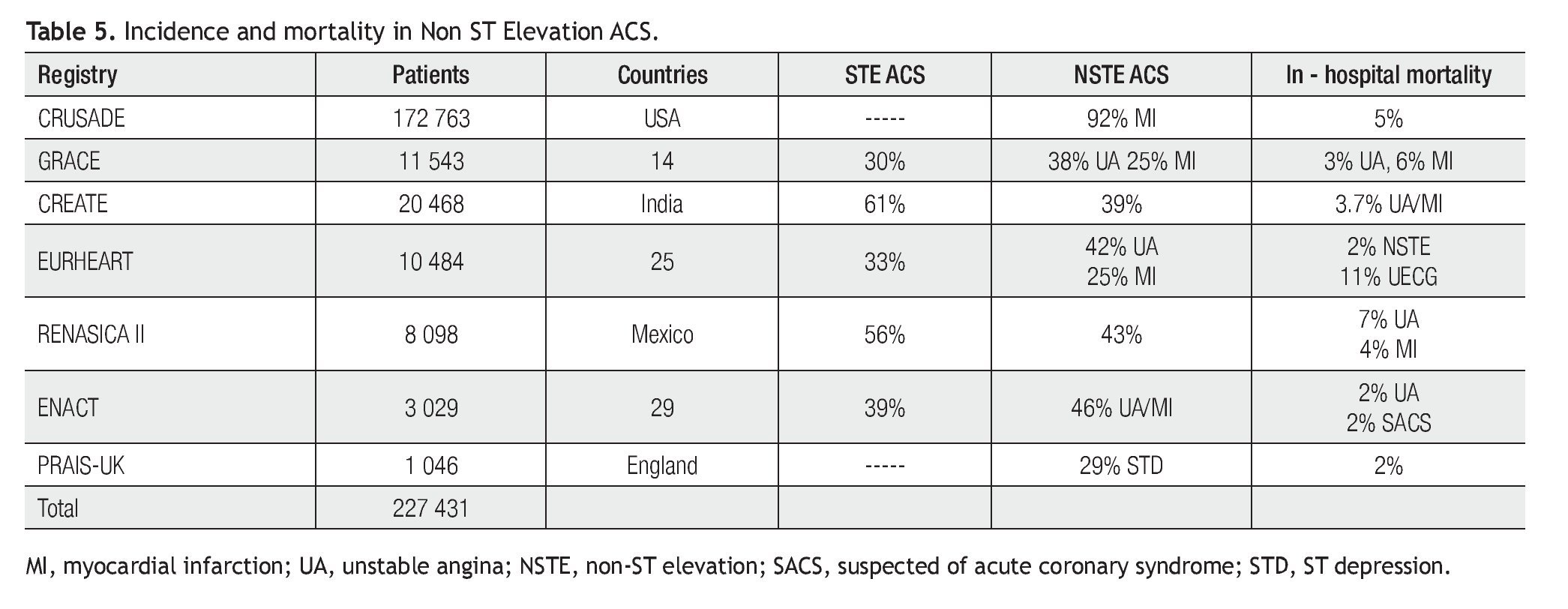
Ischemic heart disease is the leading cause of deathglobally.8 At the beginning of this century it was responsible for 7.1 million deaths worldwide;7of these, 5.7 million (80%) happened in low-income countries.9,10 In relation to baseline levels in 1990, by 2020 this disease is expected to increase by 120% in women and 137% in men in developing countries, compared with a 30% - 60% increase in developed countries.11According to epidemiological data from Mexico, it is the first mortality cause in the elderly and second in general population, being responsible for 50 000 deaths in 2003 and roughly accounting for 10% of all deaths.5 Recently, evidence coming from CREATE registry in India suggested that by 2010, 60% of the world's heart disease will occur in this country.12
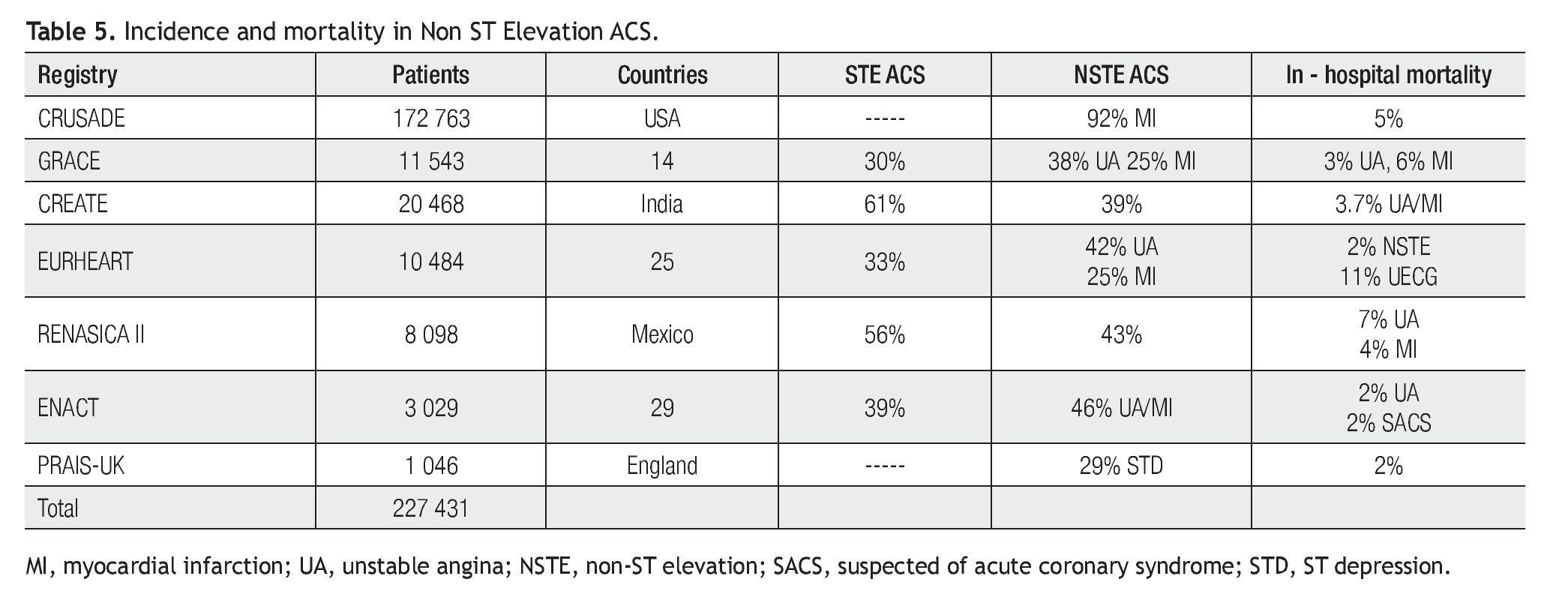
A panoramic view on 227 431 NST ACS patients from developing5,12 and developed6,13-16 countries is shown in Table 5. In Mexico and India STEMI was the most frequent clinical expression of coronary instability. This ratio between STEMI and unstable angina/NSTEMI was higher than reported for other registries. A less STEMI incidence in developed countries can be attributed to cultural differences in the perceptions of disease, insurance status (USA 27% vs Mexico 4% and Indian 4%), access to care, social support and educational level. In RENASICA II, mechanical reperfusion facilities in participating hospitals and the overall prevalence of STEMI associated to other co-morbidities (diabetes) that increased rather rapidly5 as a possible explanation were considered. In CREATE registry this issue was not analyzed.12 In NSTE ACS, in - hospital mortality ranged from 2% to 6% (Table 5), except in EUR-HEART (11%)14 and RENASICA II (7%).5 In both, troponin use was low (36% and 21%, respectively), so under diagnosis of NSTEMI has to be considered and should be fundamental to increase use of micronecrosis biomarkers to identify high-risk patients according current CPGs.2,3
Risk factors. Mexican patients had a different cardiovascular risk factors profile. They were more likely to be younger, diabetic and smokers, with less degree of renal failure. In accordance with previous evidence a higher incidence of diabetes was observed in Mexican and Hispanic patients.5,17,18 RENASICA II had the highest diabetes incidence (50%) ever reported in the setting of an ACS survey.5 Low smoking rate in American patients has to be attributed to effective anti-tobacco programs. Cigarette smoking is a powerful independent risk factor for sudden cardiac death in patients with coronary heart disease and smokers have about twice the risk of non-smokers. Primary and secondary prevention through effective anti-tobacco programs have to be implemented in order to improve the natural history of ischemic heart disease in Mexico. In RENASICA II body mass index was not considered, so it is not possible to known obesity degree; however, in American patients being overweight was the rule. The lower incidence of hyperlipidemia in Mexican patients could be attributed to genetic, nutritional habits or under-registry.
Clinical presentation and process of care. Although Mexican patients had a higher incidence of ST depression on initial ECG, CRUSADE patients had highest risk considering left ventricular dysfunction incidence and biomarkers use. In this registry patients were assisted promptly, with similar times to first electrocardiogram (< 15 minutes) and first cardiac marker assessment (~1 hour), however, several factors may explain the more conservative process of care in Hispanics: non-cardiologist management with fewer catheterization, revascularization capabilities, and insurance status.19 In RENASICA II, in spite of 90% being enrolled in tertiary hospitals with cardiologists and capabilities for angiographic stratification and percutaneous or surgical reperfusion, a conservative approach was observed too. Physician and hospitals profile, insurance use, resource and real accessibility have to be considered.
Clinical practice guidelines compliance. In-hospital antithrombotic use does not differ among groups. In spite of clinical risk and previous evidence and recommendations2,3 dual antiplatelet treatments were low in both medical care systems (middle and high income). There was a trend toward lower use of beta blockers and statins in Mexican patients (Table 3). Mexican and Hispanics were more often treated with ACE inhibitors, if this therapeutic trend was used considering a higher prevalence of diabetes and its beneficial effects to delaying macro and microvascular complications it is unknown.19,20 A similar trend was observed with glycoprotein IIb / IIIa inhibitors in Mexican and Hispanic patients in whose less invasive management was used. Considering current therapeutic directions in NSTE ACS,2,3 strategies to improve compliance have to be implemented. However, whether or not low compliance is due to drug contraindication or collateral effects is unknown.
Mortality. Despite differences in baseline risk factors and process of care, and risk stratification, in-hospital mortality was similar in all groups of patients (Table 4). Although Mexicans and Hispanics could have higher rates of diabetes, obesity, lower socioeconomic status and difficulties to proper health care, they had lower all-cause and cardiovascular mortality rates than non-Hispanic whites. This phenomenon has been dubbed the "Hispanic paradox".21-23 Although, similar outcomes have also been reported in STEMI,24-26 better short-term outcomes and long-term follow-up studies are needed to assess these observations. Continued cardiac care for secondary prevention may be unfavorably affected by socioeconomic factors such as poverty, limited insurance coverage, and restricted access.27
Registries role in evidence-based medicine. Non-randomized prospective registries document the treatment and outcomes for consecutive patients in clinical practice.
Therefore, data are gained from a 'real-world' selection of patients, many of whom would be excluded from randomized control trials (RCTs), in a variety of clinical settings. These studies are costly, which limits the size of the populations under study. In contrast, registries can survey large populations, providing a powerful scientific tool.4 Currently, the main goal of evidence-based medicine is to guide therapeutic decisions; in ST elevation MI only 13% of the recommendations in the USA guidelines are based on level A evidence.28 CRUSADE and RENASICA II are contemporaneous high quality registries4,28,29 including entire spectrum of NSTE ACS in a representative population with co-morbidities under-represented in RCTs. The findings have the potential to provide a link between RCTs and the real clinical situation. In addition, both prospective registries provide a unique opportunity to accurately assess current clinical practice and in-hospital outcome and contribute to an ongoing process of quality assurance, indicating areas where education is necessary, in which treatment practices are suboptimal or conflicting with guideline recommendations.4
Limitations. Post-hoc analysis, lack oflong-term follow-up and several variables were not considered in either registry. Higher clinical risk profile in CRUSADE patients compared to RENASICA II patients has induced mortality bias. CRUSADE was not specifically designed to assess patterns of care according to ethnicity and, therefore, did not collect information on subcategories of Hispanic origin. Another important bias was that all patients in RENASICA II and CRUSADE registries were already hospitalized and, therefore, may represent a population with better access to health care and with higher socioeconomic status than the general population in both countries. In both registries contraindications or collateral effects for specific drugs were not analyzed.
Conclusions
In post-hoc analysis Mexican patients with NSTE ACS had a different cardiovascular risk factors profile, clinical presentation, risk and less intensive in-hospital treatment than Hispanic and non-Hispanic white patients. However, these differences do not appear to affect in-hospital mortality.
Corresponding author: Carlos Martínez Sánchez.
Instituto Nacional de Cardiología Ignacio Chávez. Juan Badiano No. 1. Colonia Sección XVI, Tlalpan. CP.14050. México.
(52) 55 73 29 11.
E-mail: marcar@cardiologia.org.mx
Received on May 27, 2011;
accepted on January 16, 2012.