


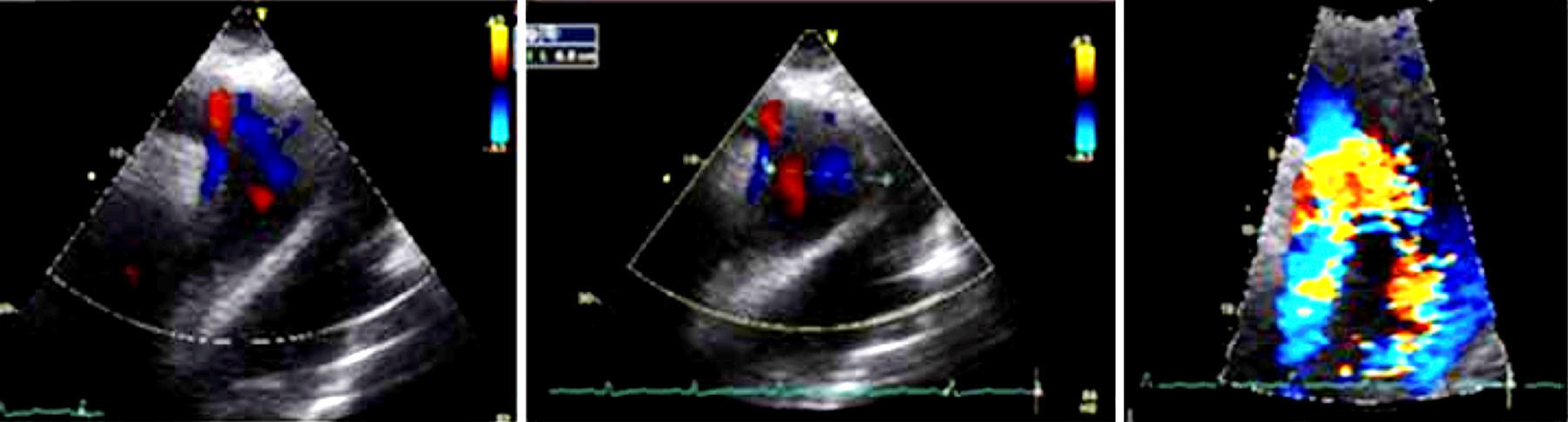
The acute aortic syndrome refers to a spectrum of life-threatening aortic emergencies. Acute aortic syndromes include non-traumatic entities as aortic dissection with an incidence of 80–90% of the cases, affecting 5–30 person-years, penetrating atherosclerotic ulcer with a incidence of 2.8% and intramural hematoma with incidence of 5–25%. Nowadays there are several imaging modalities for diagnosis, such as echocardiography, magnetic resonance imaging and computed tomography angiogram without let out the clinical characteristics and keep in mind differential diagnosis for initial suspicion (Figs. 1 and 2).1–3

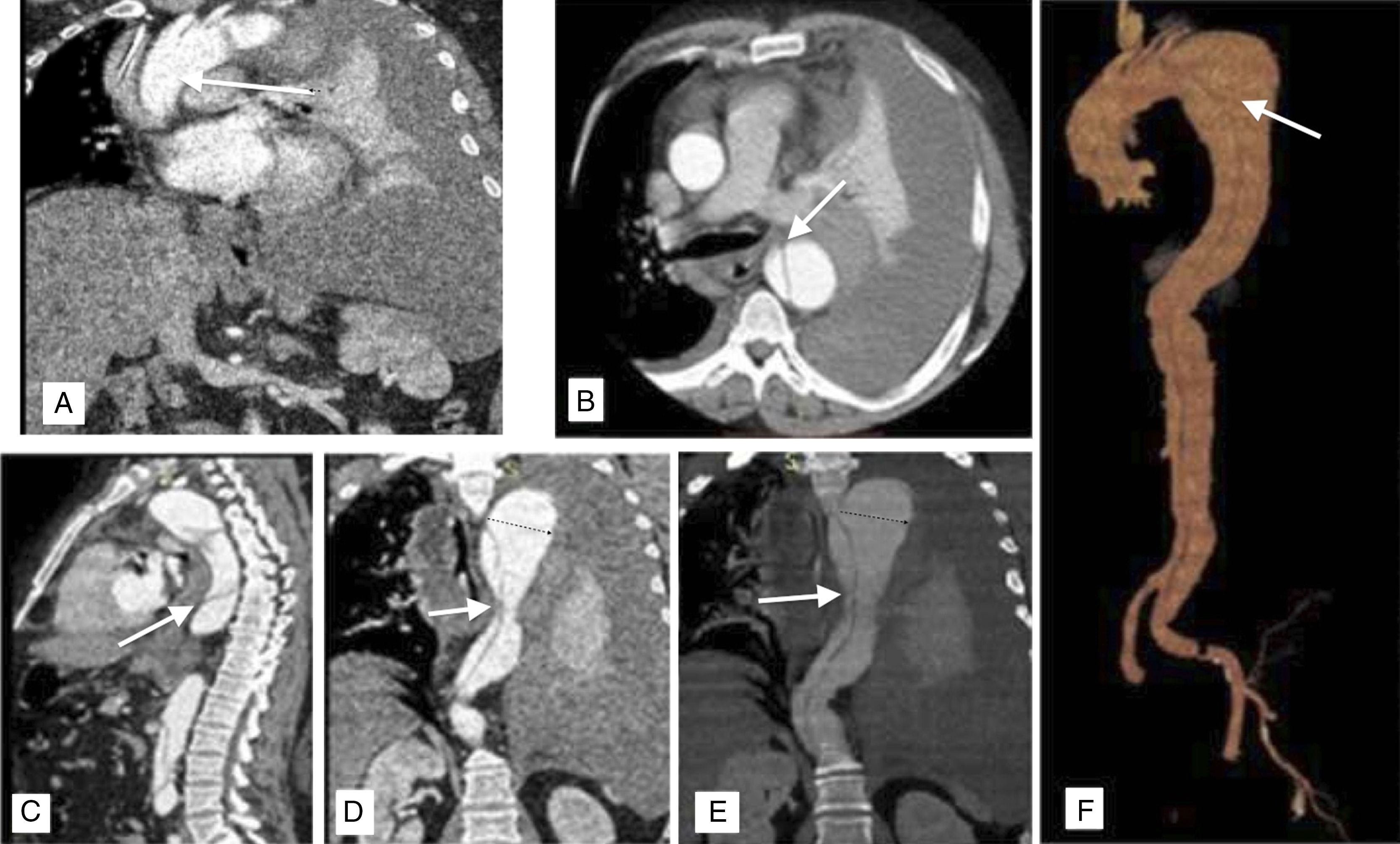
 Chest CT sagittal and axial scans showing aneurysmal dilatation with extravasation area, left pleural effusion. (C–E) Sagittal and coronal section showing double lumen from descending aorta to common iliac. (F) Digital reconstruction of aorta.")
We report the case of a hypertensive 42-year-old, with obesity and obstructive sleep apnea. He starts with oppressive chest pain with adrenergic discharge at rest, lasting 40min, blood pressure was documented to 180/111, electrocardiogram with positive slope of the ST in aVR and V1 and negative troponin. The patient developed cardiogenic shock and death.4–7 Acute aortic syndrome should be identified early by clinical suspicion and supported by diagnostic studies to provide timely treatment because of its high mortality rate. Diagnostic imaging studies in clinical suspicion of dissection play an important role, such as confirmation of clinical suspicion, classification of dissection, localization of tears, assessment of extent of dissection and indicators of urgency.8
Ethical responsibilitiesProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
FundingNo endorsement of any kind received to conduct this study/article.
Conflict of interestThe authors declare no conflict of interest.