


Case presentation
A 65-year-old woman with high blood pressure and past medical history positive for rheumatic fever during childhood on ambulatory medical treatment with spironolactone, enalapril, and furosemide presented at our institution, the Instituto Nacional de Cardiologia Ignacio Chavez, with a history of progressive worsening of her functional class over the last 6 years. She was referred to our Institute after detecting a cardiac murmur. A trans-thoracic echo-cardiogram showed evidence of inactive rheumatic heart disease, pure mitral valve stenosis with a mean trans-mitral valve pressure gradient of 15 mmHg, and dilatation of the left atrium of 47 mm. In addition, there was evidence of mild mitral valve, tricuspid valve, and aortic valve regurgitation, as well as pulmonary artery hypertension with a pulmonary artery systolic pressure calculated at 62 mmHg. Left ventricular ejection fraction was normal (70%). Echocardiographic Wilkins score was calculated at 6 and the patient was considered for percutaneous mitral valvuloplasty with the Inoue balloon.
Valvuloplasty technique
Using the modified Seldinger technique, introducer sheaths were placed in the right (8 Fr) end left (11 Fr) femoral veins, as well as the left femoral artery (6 Fr). Left and right cardiac catheterization was performed, measuring baseline pressures at main pulmonary artery, pulmonary capillary wedge, and left ventricle; as well as simultaneous trans-mitral pressure gradient. In addition, a left ventriculogram was performed in the RAO projection.
After baseline hemodynamic assessment, percutaneous mitral valvuloplasty was performed, for which a Mullins catheter was advanced with the Brockenbrough needle through the right femoral vein. At this point, an AcuNav (Acuson, Mountain View, CA) intracardiac echo-cardiogram (ICE) catheter was advanced through the left femoral vein. This catheter system consists of an element located at the tip, which collects two dimensional ultra-sound images at 7 and 8.5 MHz resolution, and a handle with three rotator controls, two to position the tip of the catheter and the other to lock it in position.
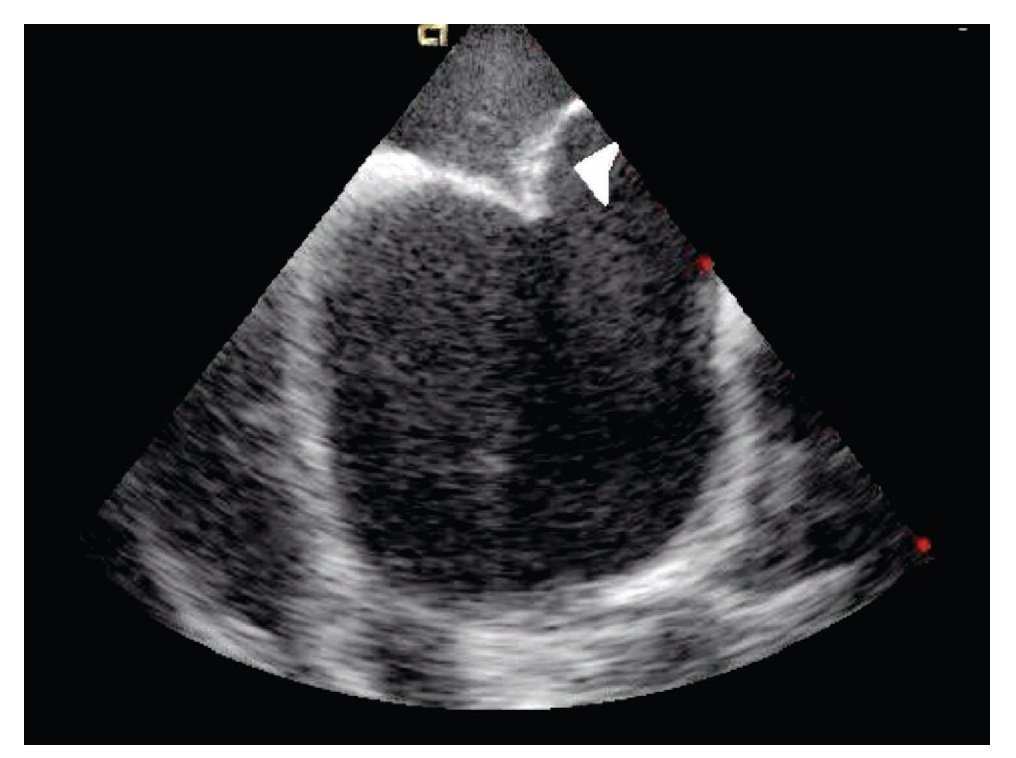
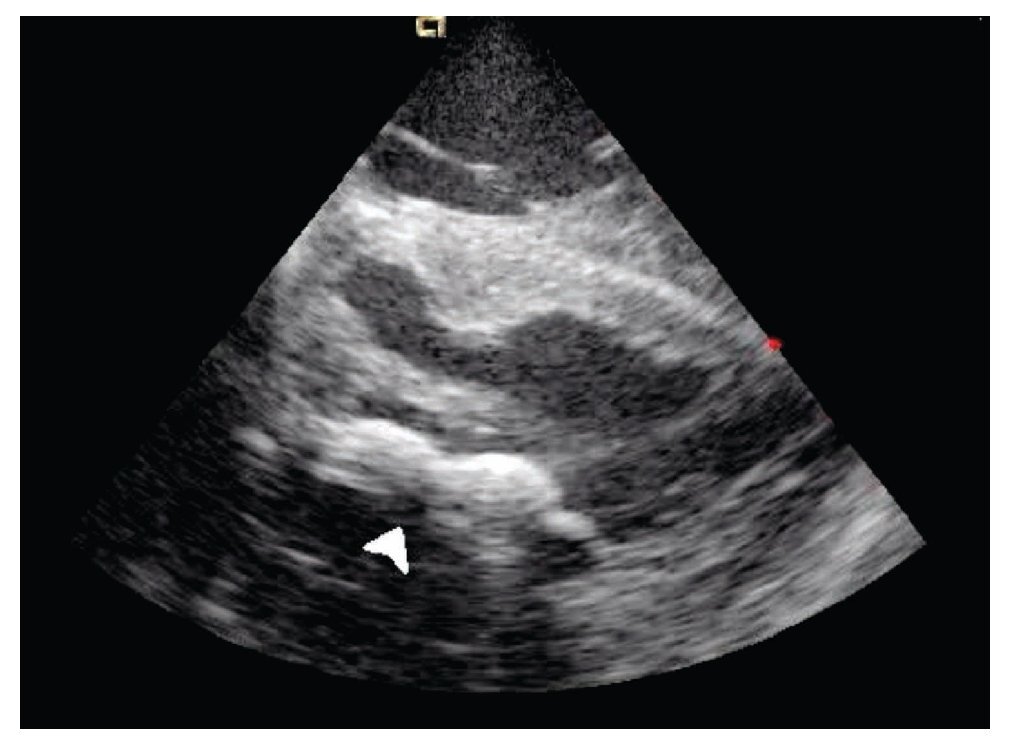
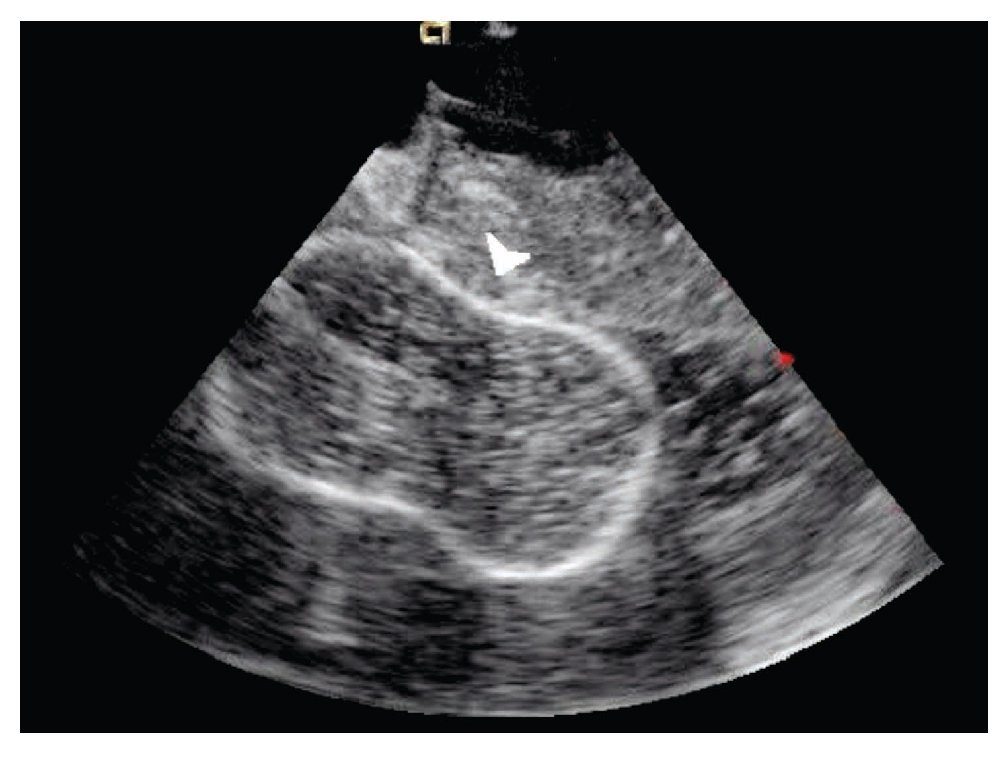
The transeptal puncture was performed under direct ultrasound guidance (Figure 1). After hemodynamic confirmation of left atrial curve morphology, the Mullins catheter was advanced and exchanged for a spiral guide-wire. Interatrial septum was dilated with the usual technique and an Inoue 28 balloon was advanced through the mitral valve into the left ventricle under direct ultrasound guidance (Figure 2). Mitral valvuloplasty at the level of the valve (Figure 3) was performed by a single inflation with the Inoue balloon with 28 ml of normal saline. ICE analysis across the mitral valve showed a significant drop of mean transmitral valve gradient and an increase of the mitral valve area, without an increase of mitral regurgitation.
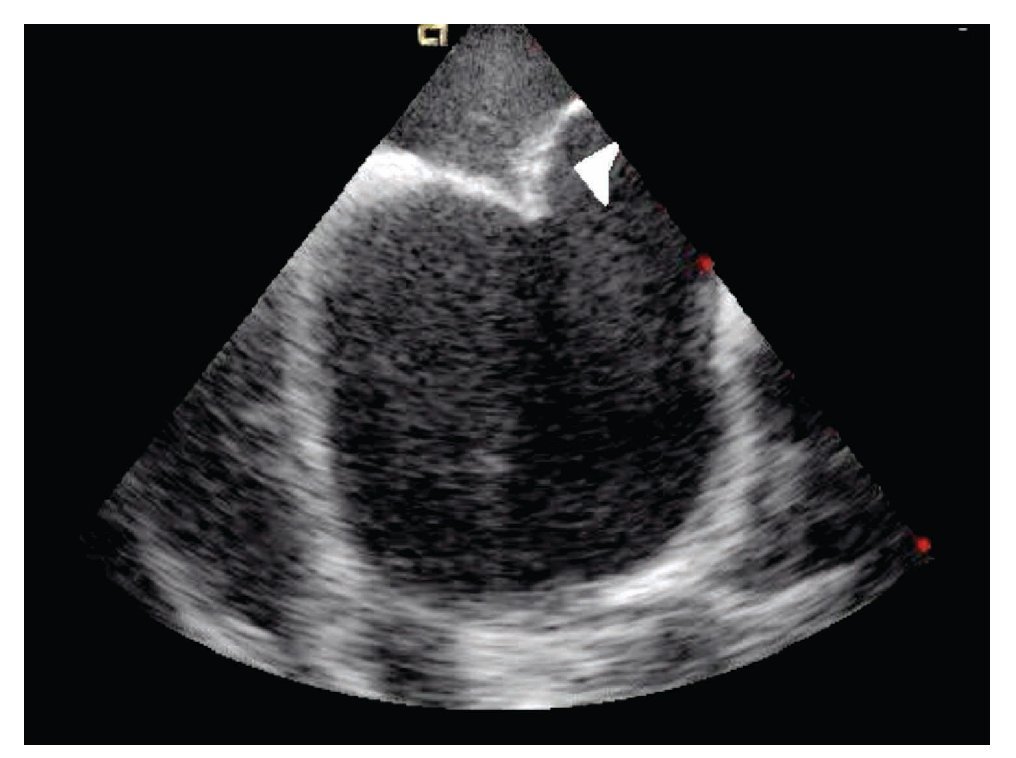
Figure 1. Intracardiac echo in short-axis view showing the interatrial septum forced off the left by the Brockenbrough needle.
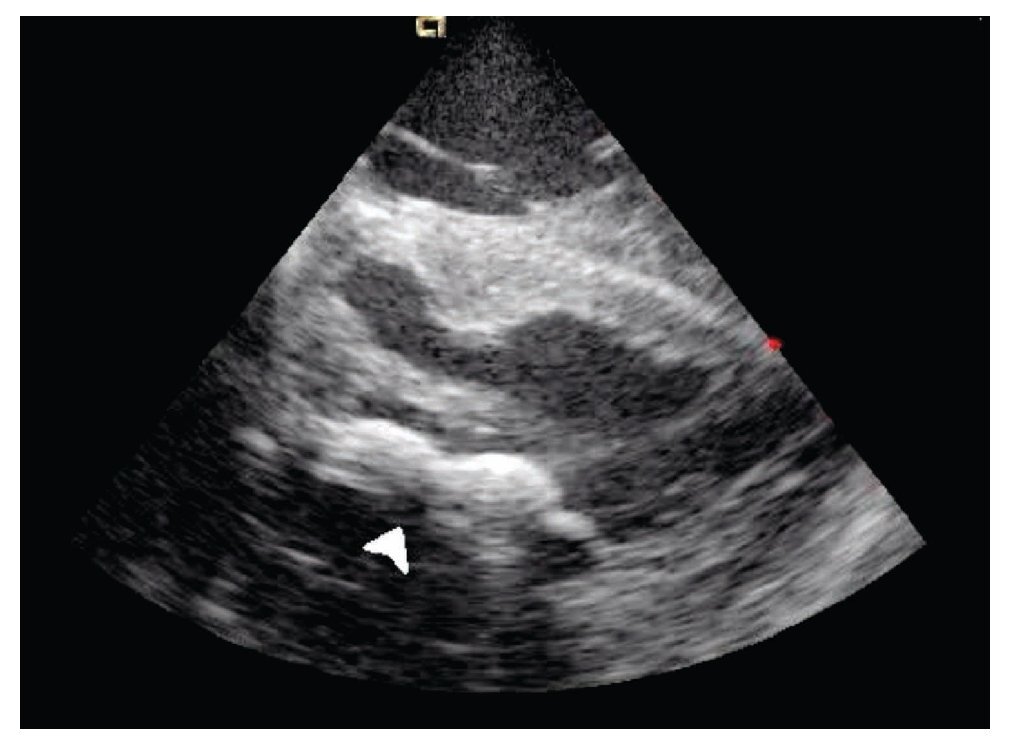
Figure 2. Shows the Inoue balloon deflated (arrow) at the mitral valvular plane in a long-axis view of the left ventricle.
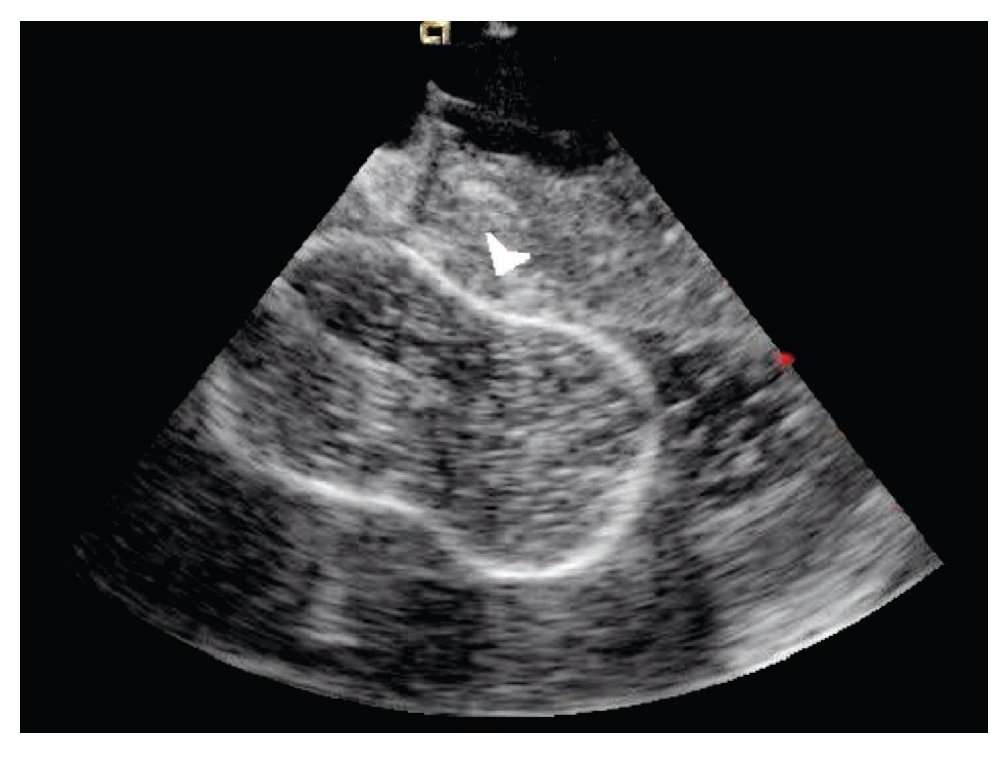
Figure 3. Shows the Inoue balloon inflated (arrow) with a waist in its middle; mitral valvular plane in long-axis view.
Conclusions
Intracardiac echocardiography is a relatively new ultra-sound imaging modality that has been progressively used for guidance of interventional cardiac procedures.1 The first experience in humans with this method was reported in 2000 presenting two cases of mitral valvuloplasty with distorted anatomy of the interatiral septum due to bulking of the fossa ovalis within the atrium;2 since then, several reports have been published confirming its usefulness in the guidance of several interventional cardiac procedures, and it is currently replacing transesophageal echocardiography in the guidance of transcatheter treatment of interatrial and interventricular septal defects, patent foramen ovale, as well as in the guidance of transeptal puncture procedures for mitral stenosis and radiofrequency ablation of atrial fibrillation.3,4 At the Instituto Nacional de Cardiologia Ignacio Chavez, this method was started to be used around the year 2002 for guidance of the interventionist treatment of congenital structural heart disease.5 This is the first case at our Institute, however, of ICE guidance of a percutaneous mitral valvuloplasty with Inoue balloon. Its potential advantages would be that it provides guidance for a safe and rapid transeptal puncture, shortens fluoroscopy exposure time, and provides immediate on-line assessment of the result of the mitral valvuloplasty by both two-dimensional ultrasound and Doppler technique.5,6,7 We hope that the ICE guidance for mitral valvuloplasty will help the low-volume inter-ventionist to obtain similar results as those performing lots of procedures per year in a high-volume reference center. This can be achieved by reducing the potential complications of trans-septal puncture during the Inoue balloon mitral valvuloplasty.
Corresponding author: Marco Antonio Martínez Ríos.
Hemodynamic Service. Instituto Nacional de Cardiología.
E-mail: mtzrios@cardiologia.org.mx
Received on December 24, 2009;
accepted on February 16, 2010.