


Cardiovascular diseases (CVD) presentation patterns have changed over the last century. During the first decades of the 20th century CVD were caused mainly by infections and/or parasitic etiologies, such as rheumatic fever and syphilis,1 treatment was based on palliative measures until the discovery of antibiotics2 and other drugs around the middle of this century; with the use of these drugs, as well as other health measures, the frequency of cardiovascular infectious diseases began to decrease.
During the second half of last century a different scenario started to arise, an increasing rate in the morbidity and mortality related to coronary heart disease, was observed along with an increased prevalence of some mayor cardiovascular risk factors,3 like hypertension,4 type 2 diabetes5 and obesity.6 Both situations have also been observed in Mexico.1,7
An epidemiological study of acute myocardial infraction (AMI)8 patients admitted at the Instituto Nacional de Cardiología Ignacio Chávez (INC-ICh) between 1954 and 1964 was published; it described the socioeconomical conditions of patients at that time. The purpose of the present study is to compare these conditions in patients admitted at the Institute forty years latter (1997-2007) with the same diagnosis.
Method
The present study included the first AMI of all discharged patients seen at the INC-ICh between 1997 and 2007. Diagnosis of AMI was established according to the International Statistical Classification of Disease and Related Health Problems 10th Revision9 codes I 21 to I 21.9. Age, gender, marital status, socioeconomical level, occupation and current address were obtained from each patient personal record.
Socioeconomical levels from both decades were reviewed by a Certified Social Worker and an equivalent classification was established in order to compare classifications used in each decade.
Admission and attention criteria, for patients with AMI from both decades are based on the Ley General de Salud and therefore are comparable: Social Security and High Income Patients are given emergency medical care, then the former are send to the appropriate hospital or clinic to continue their treatment. The AMI diagnosis was based on clinical findings, ECG changes and enzyme determinations in both decades.
A total of 5872 patients were identified; 34 patients, (15 women and 19 men) 14 to 30 years old were eliminated from the analysis because they had other cardiovascular diseases like: coronary aneurism or Kawasaki disease in three cases, congenital heart diseases five cases, drug addiction (cocaine) four cases, antiphospholipid syndrome three cases, Takayasu disease two cases, 11 unknown etiology cases, family hypercholesterolemia in two cases and four with different diseases (Pulmonary thrombusembolism, pulmonary hypertension, pericarditis, and Aortic stenosis).
A data base was constructed with current data, and the statistical analysis was carried out with Stata software version 8.0 for Windows. Mean and standard deviation of patients´ age, for all patients and by gender were estimated, as well as the proportion of each gender, marital status (married, including living together, divorced, single, and widower), socioeconomical level (i, ii, iii, iv, and v according to current INC-ICh classification, lowest income patients are classified as i to iii, medium class as iv, and class v are the highest income patients), occupation (free-lance professionals, executives, office-worker, commerce worker, skilled worker, unskilled worker, farmer, retired, students, and housewife), and residence location at the AMI occurrence (state of the Mexican Republic). Data from 1954-1964 decade were taken from a previous published paper.8
Data from both decades were compared with aggregated statistical methods; chi square test was used to compare qualitative variables such as socioeconomical level, marital status, occupation and residence location. Quantitative variables were compared between groups with Student T test. Statistical significance was set at a p value equal or smaller than 0.05. The study was approved by the Institutional Ethics and Research Committees
Results
The number of AMI patients in the INC-ICh in the 1997-2007 decade (5,838) increased five times in relation to 1954-1964 decade (1171).8 No differences were identified in the proportion of women (22.3% [1954-64]8vs. 20.3% [1997-07]) and men (77.7% [1954-649]8 vs. 79.7% [1997-07]) and, in the average age in men 57.1 years (1954-64)8vs. 58.4 years (1997-07), the average age in women showed that women from the 1954-64 decade (61.2 years) were younger8 than women from 1997-07 decade (65.4 years); however, AMI was diagnosed in younger women in the 1997-07 decade (31 years old) than in the 1954-64 (36 years old).8 The youngest male in both decades had similar age (25 years old [1997-07] vs. 24 years old [1954-64]).8
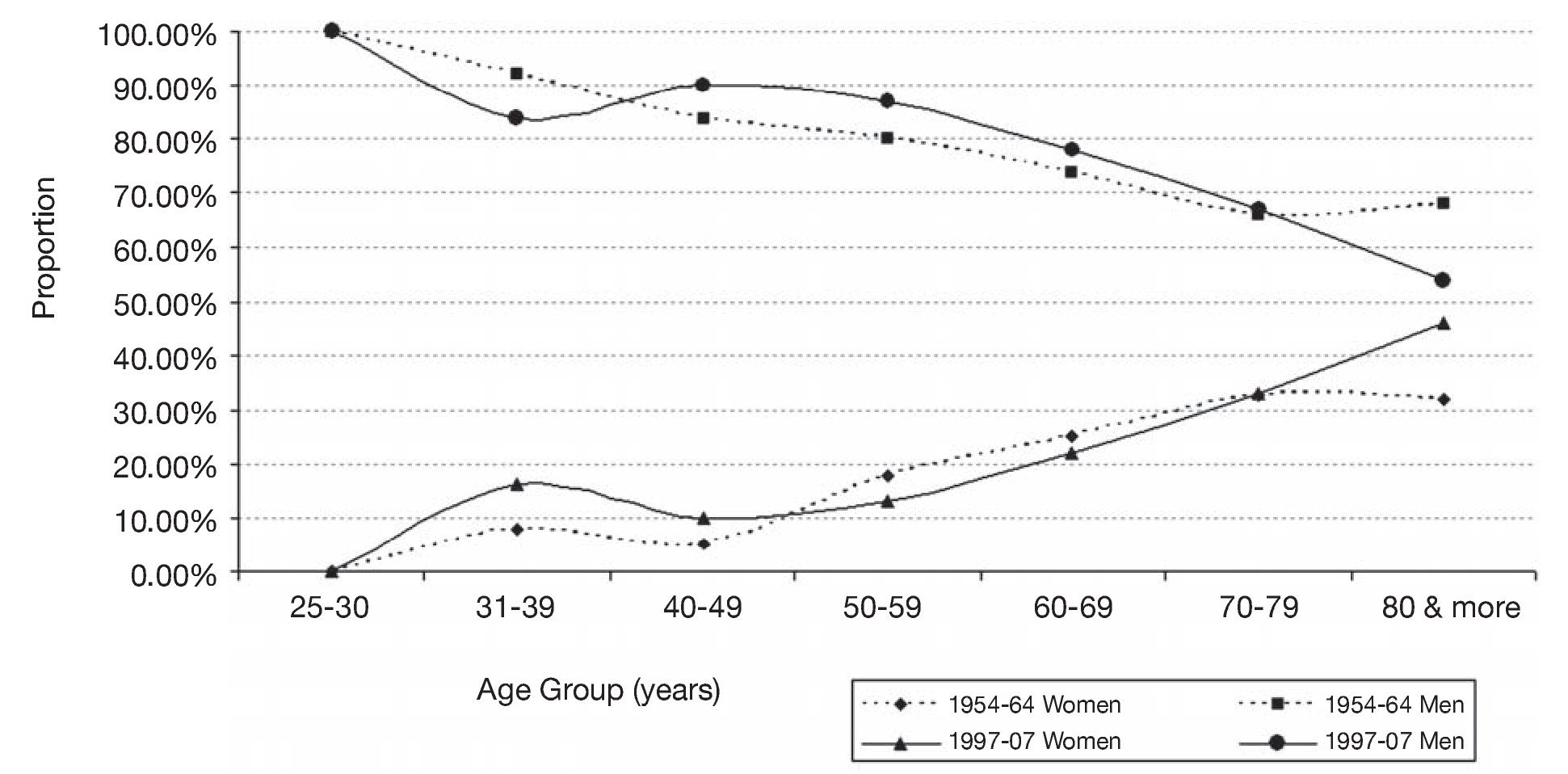
Analysis of the proportion of women and men with AMI by age showed that in both studies the number of young men, between 25-30 years, was larger than the number of women; and this tendency continued until the women reached the 7th decade of life (between 60-69 years); at this time the proportion of men started to decrease (29.4%) in relation to women (26.4%), in the 80th decade when the number of AMI cases in women (28%) was twice the observed in men (14%) and in the 90th decade, there were three women (12%) per each men (3.7%) (Figure 1).
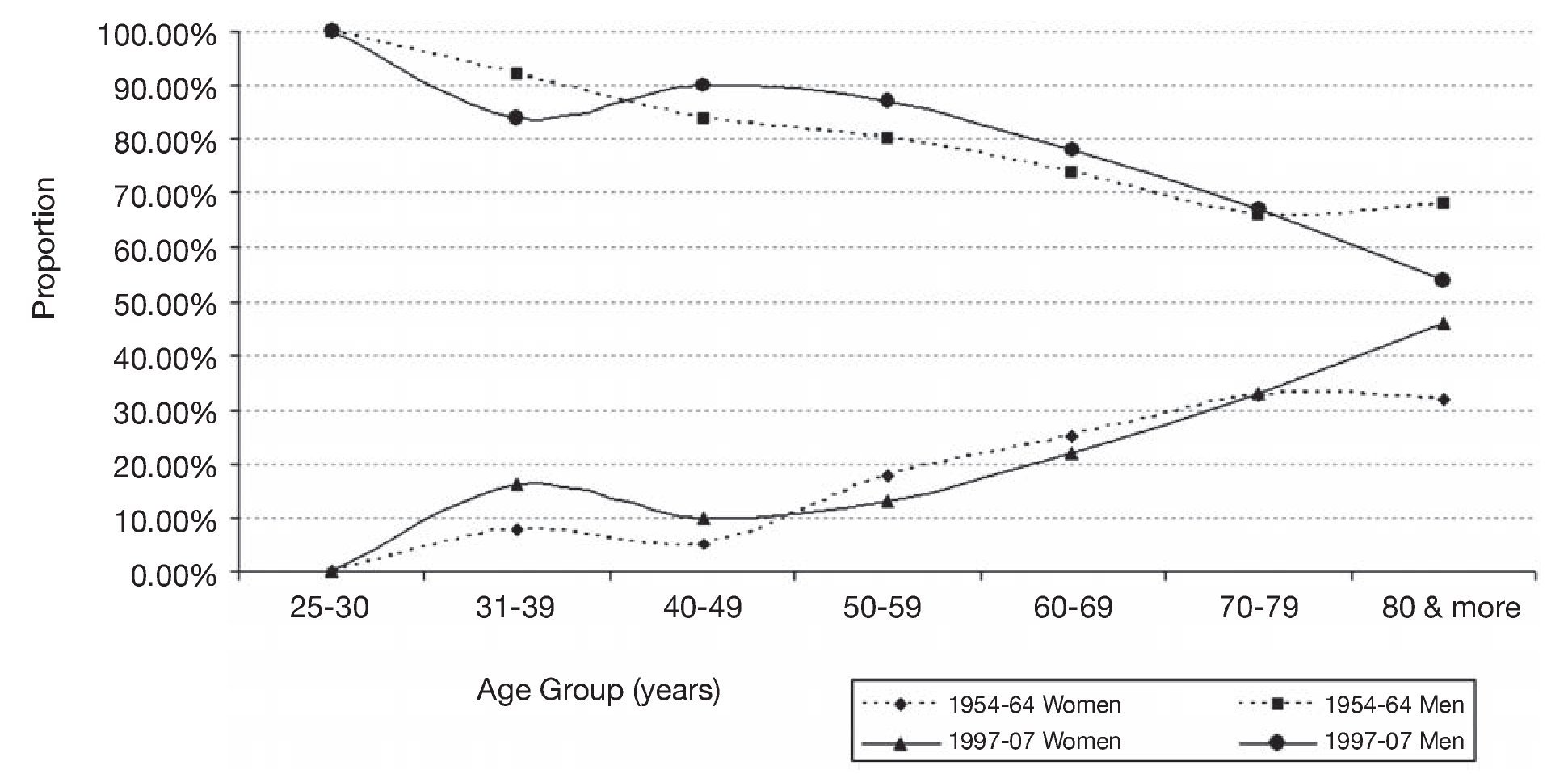
Figure 1. Comparison of proportion between women and men by age group.
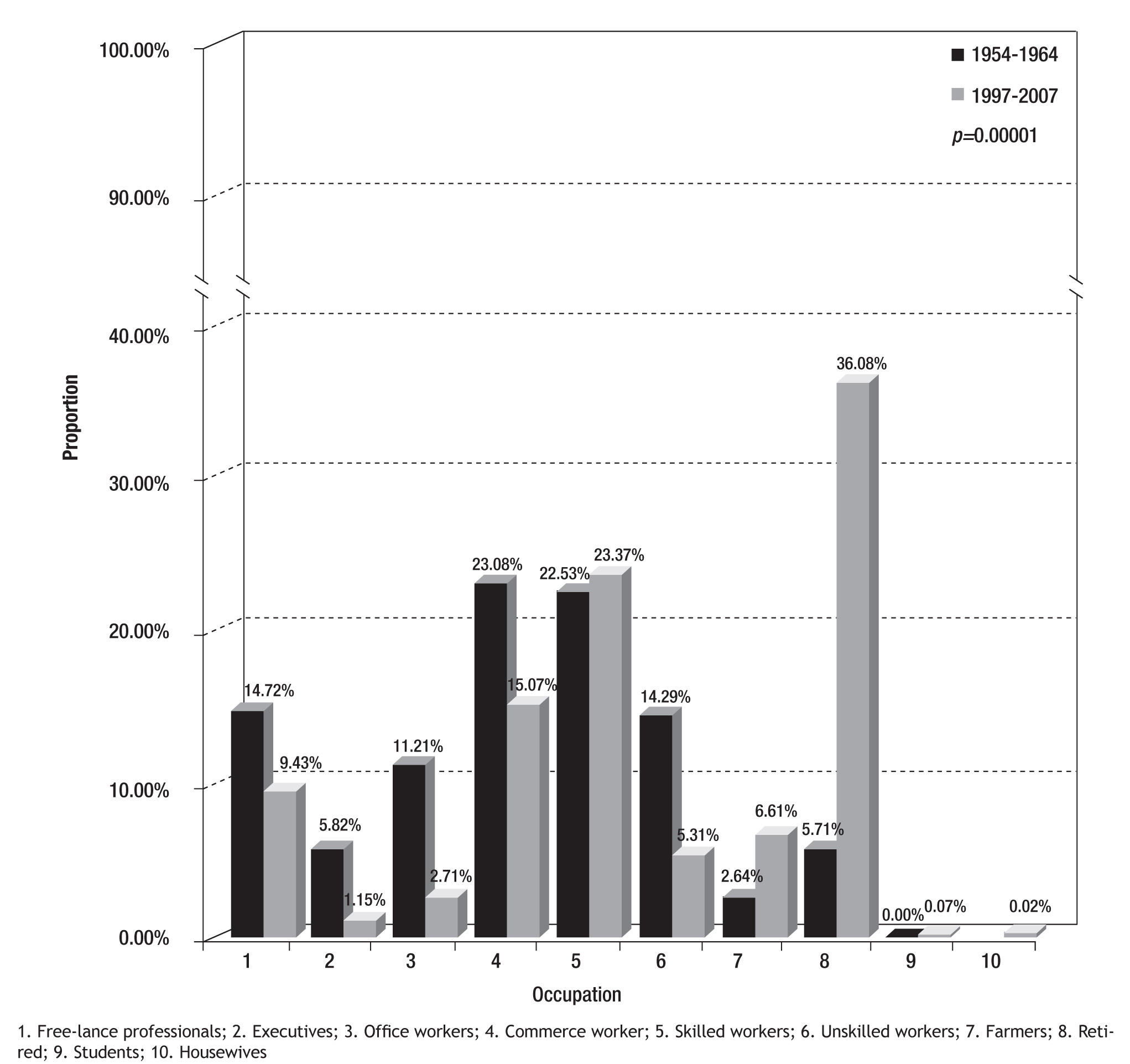
The distribution of male patients´ occupational activity showed significant differences between the studied decades. While most patients were traders or skilled-workers in the 1954-64 decade,8 the majority of patients in the 1997-07 decade were retired, followed by skilled-workers. In the 1997-07 decade most women were housewives (75.3%), but this information was not available for the 1954-64 decade8 (Figure 2).
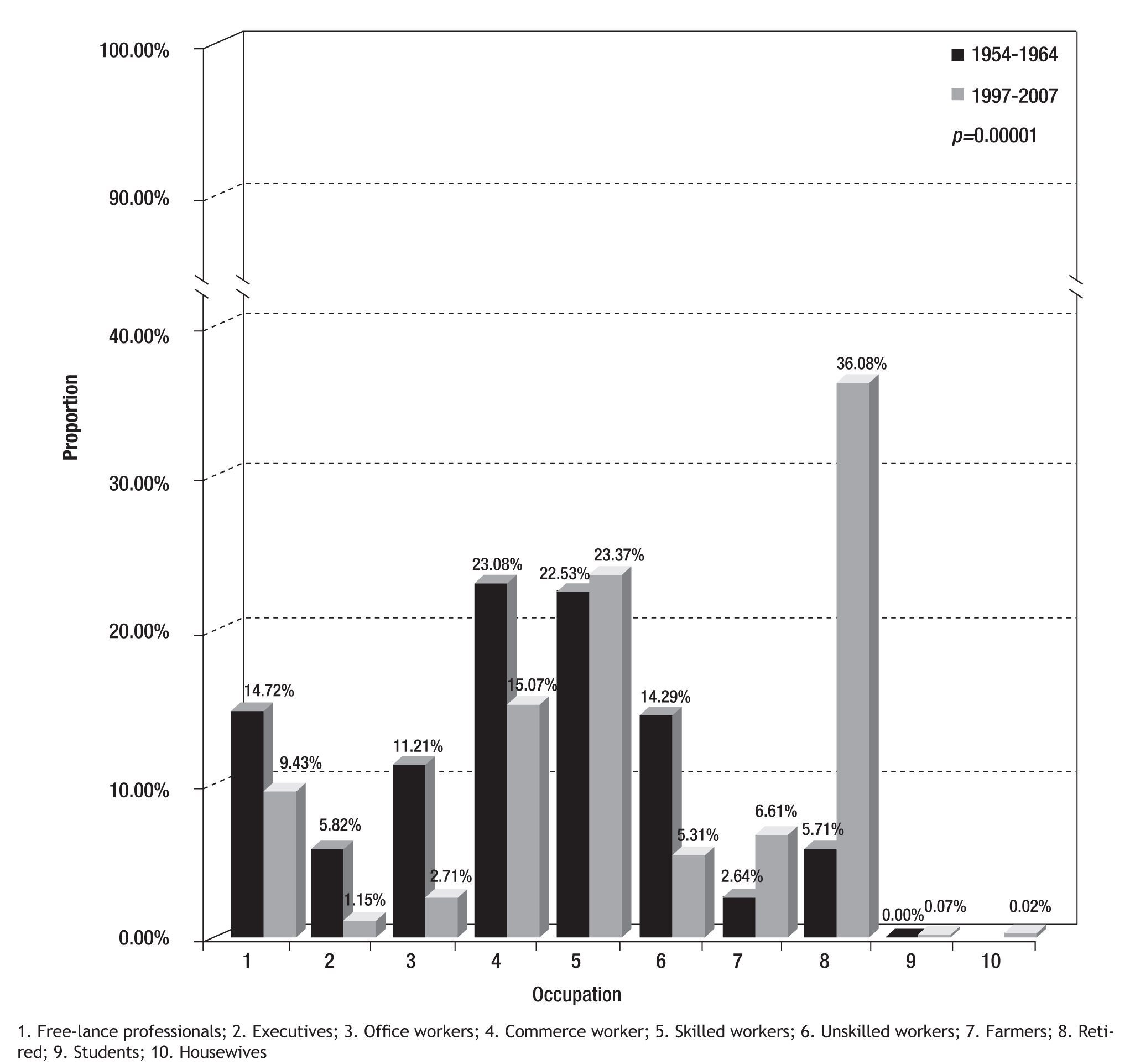
Figure 2. Occupational activity in male myocardial infarction patients.
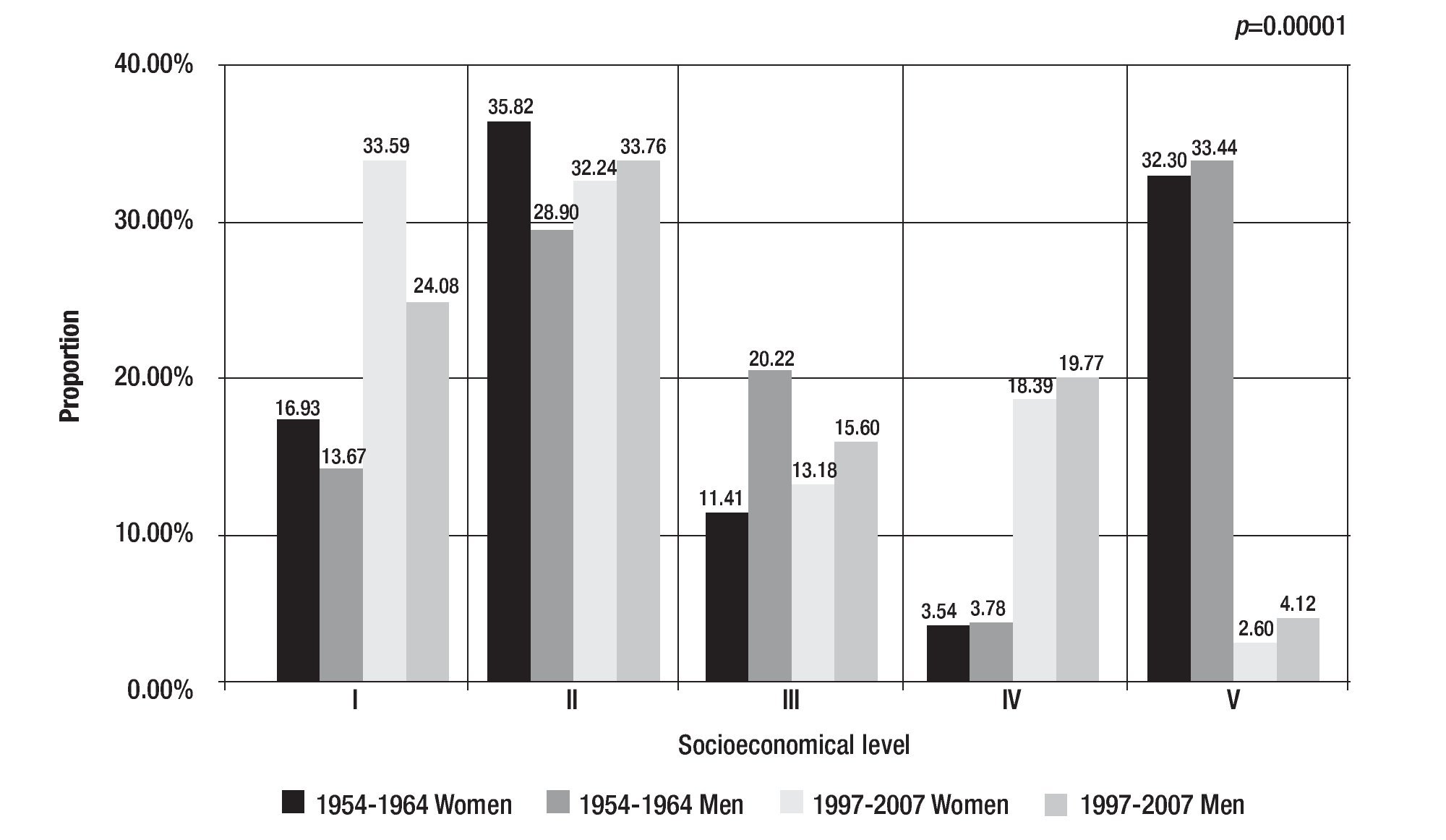
Socioeconomical level showed that in the 1954-64 decade8 the largest proportion of patients belonged to the classes II and V, the former included low income patients while the class V included high income patients. In the 1997-07 decade, the majority of patients were classified as class I of II, both include low income patients, these differences were statistical significant (p < 0.0001), (Figure 3).
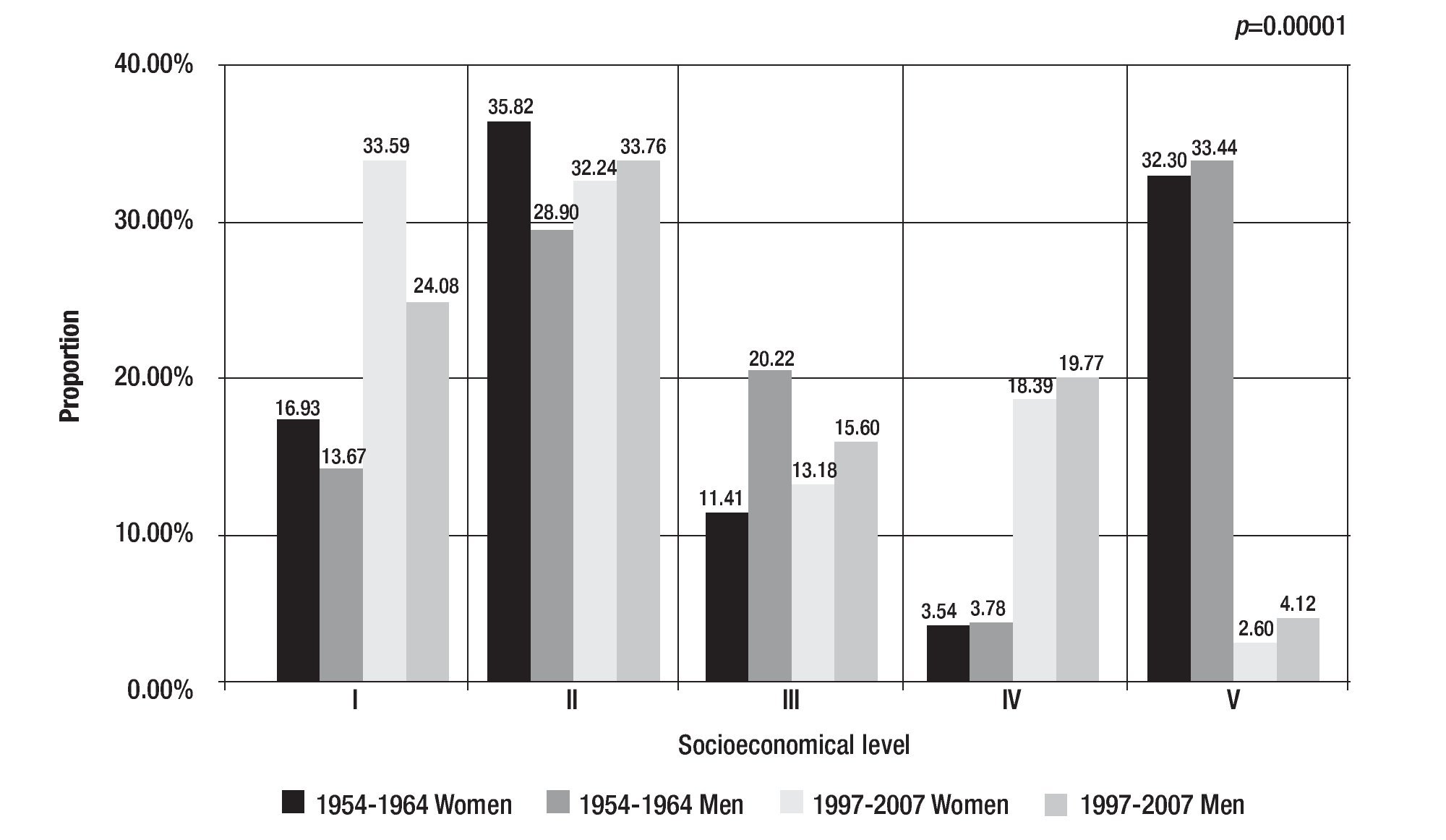
Figure 3. Socioeconomical level of myocardial patients.
In relation to the marital status the largest proportion of women and men in both decades were married, however, two times more men were in this status than women. Most women in both decades tend to stay married or were widows, nevertheless, single and divorced in the 1997-07 decade were 1.6 and 3.7 more frequent than in the 1954-64 decade.8 In the group of men, divorce increased 1.7 times between decades. These differences were statistical significant (p <0.0001).
Most patients from both decades were living in Mexico City at the occurrence of the AMI (81.12% in 1954-648 and, 99% in 1997-1907).
Discussion
This study compares some socioeconomical characteristics of AMI patients treated at the INC-ICh in two decades 40 years apart; the most important finding was that the number of AMI patients increased five times in these four decades even though the number of ward beds is almost the same.
Changes in the occurrence of myocardial infarction could be partially explained by demographic variations like the fact that the Mexican population has tripled between 1950 (25 millions) and 2000 (97.5 millions) and approximately one third of the population lives in Mexico City Metropolitan Area.10 Life expectancy has also increased from 49 to 75 years, the death rate of children under one year has decrease seven times since 1930 (from 178 to 24 per each 1000 new born)11 and the global fecundity rate decreased from 7.3 to 1.8 children per mother.12
Gender13 and age14 are two variables closely related to AMI. There are marked differences between genders, it is well known that men have higher incidences of AMI than women, and that these differences are more important at younger ages,15 and as the women reaches the menopause these differences become smaller until the incidence is almost the same between the seventh and eight decade
In our study, no differences were identified between patients from both decades, in relation to gender, the proportion of women and men that were admitted in 1954-648 and 1997-07 were almost the same; however, the age of women at the time of diagnoses was younger in 1997-07 than in 1954-64;8 further more, the proportion of women by age showed a similar tendency in both decades, the frequency of women diagnosed with AMI increased after the menopause, and, when women reached the 80th decade of life the proportion of women admitted with AMI was larger in 1997-07 than in 1954-64,8 and larger than in men.
The urbanization and industrialization process, have a direct impact on the lifestyle, and on the occupational activities which also showed a different behavior between both studies. While in 1954-648 most male patients worked in commerce (23%) or were skilled workers (23%), in 1997-2007 they declared themselves to be self retired (36%). Many social aspects, like the occupational activities, the income and the education level are strongly associated among them.16 A higher education level gives better occupational opportunities and as a consequence the income increase. In 1954-64 patients with AIM treated at the INC-ICh were divided in two occupational activities, two socioeconomical level and in two educational levels8 since in 1950, 44% of the Mexican population was illiterate, today only 9% are in this situation, which could be represented by the skilled workers with a low income, and may be the traders group was a mixture of middle and high social class with at least primary education in 50% of this group and university education in the other 50%.
Socioeconomical level also showed significant differences between the two studied decades, in 1954-648 patients with AMI were divided in two socioeconomical levels in a similar percentage, low income and high income; in the second decade, most patients (60%) were of very low or low income, this shows that the prevalence of this disease is related to social classes. Some hypothesis can be mentioned to explain these findings: adverse lifestyle such as nutritional habits, sedentary, and smoking among other have affected all socioeconomical levels, in developed countries, these adverse lifestyles are less common among high income population which may explain the decrease on the incidence of CHD in those countries17,18 but not in Mexico. In terms of medical care high income patients now have access to private care mostly through medical insurances (personal or as an employee) in which coronary care units (CCU) are now available. In 1954-648 treatment of AMI was given in the general wards of hospital, even at the INC ICh, in which the CCU was inaugurated in 1969,
In developed countries the educational level as a measured of social and economical opportunities, has been related to morbidity and mortality, people with more educational level have lower death rates than those with less education,19,20 this have change over the years, around 1950 these countries had similar or probably higher morbidity and mortality rates, especially from cardiovascular disease, in higher social classes than lower ones,21 there was suggested by Morgestern that the education and the CHD mortality relationship will vary depending upon a society's progress towards "modernization".22 In Mexico, morbidity and mortality is unevenly distributed depending on the wealth distribution, the educational level, the access and quality of health services.
Conclusions
The trends and patterns of disease may be determined by multiple factors, such as the personal once like physiological mechanisms, genetic information, and metabolism, but an important roll is played by socioeconomical factors which can make a difference among people form the same country living in different locations, or even increase the presentation of a some disease in certain socioeconomical levels. In this study social and economical factors showed significant differences among AMI patients treated at the INC-ICh.
Corresponding author: Maite Vallejo.
Juan Badiano No. 1. Col. Sección XVI, Tlalpan. México D.F. México 14080.
Fax: (55) 5573. Telephone: (55) 5573 2911 Ext. 1178 and 1514.
E-mail:maite_vallejo@yahoo.com.mx
accepted on January 3, 2011.