


Introducción: Hace algunos años, el motivo principal para la solicitud del diagnóstico parasitológico era la sospecha de una etiología de base parasitaria. En la actualidad, el motivo de consulta y la solicitud del diagnóstico se encuentran asociados con una comorbilidad hemato-oncológica, autoinmune, inmunodeficiente o una condición postrasplante.
Método: Se analizaron los resultados del laboratorio de parasitología clínica del Hospital Infantil de México Federico Gómez de enero de 1990 a diciembre del 2010, para obtener la frecuencia y distribución de parásitos y comensales por año y década.
Resultados: Se analizaron 211,600 muestras del periodo estudiado, con una media anual de 10,100 y desviación estándar de 3,500. El porcentaje de parásitos y comensales fue del 37.73%, y la frecuencia de positividad solo a parásitos fue del 21.4%. La diferencia de proporciones entre décadas resultó significativa, con una p < 0.0001.
Conclusiones: La tendencia en el comportamiento de las parasitosis intestinales durante el periodo estudiado mostró un cambio tanto en frecuencia como en género y especie de los agentes reportados. La generación de información de carácter epidemiológico es necesaria para conocer la tendencia de las parasitosis y de sus variaciones a través del tiempo.
Background: In recent years, the main reason for parasitological diagnosis was suspicion of a parasitic etiology. Currently, diagnosis and consultation are associated with co-morbidity with a hemato-oncological, autoimmune, immunodeficiency or post-transplant condition.
Methods: Results collected from the Parasitology Laboratory of the Hospital Infantil de Mexico Federico Gómez from January 1990 to December 2010 were analyzed to determine the frequency and distribution of parasites and commensals per year and decade.
Results: There were 211,600 samples analyzed with a statistical media of 10,100 and a standard deviation of 3,500 samples. Percentage of observations for parasitic structures as well as commensals was 37.73% according to Pearson Chi square with a significant difference among percentages between decades (p < 0.0001).
Conclusions: Behavioral tendency of intestinal parasitosis during the last two decades shows a change in frequency and genera from the agents that were reported at this pediatric healthcare level. The processing of epidemiologic information is important in order to determine the response of the parasitosis and its variations over time.
Pagina nueva 1
1. Introduction
In the decade of the 1980s, publications in Mexico reported the prevalence of intestinal protozoosis, which ranged from 14.9% in the state of Puebla1 up to 70% in the suburbs of the Distrito Federal (D.F.).2 This variability is dependent on the socioeconomic area, size of the sample studied, population studied, etc. Of the total children who presented for consultation at the HIMFG between 1990 and 1994 due to suspicion of parasitosis and who had stool tests for parasite concentration, a figure of 44.2% positive for Giardia lamblia was obtained, ranking this parasite as the parasite of greatest frequency among intestinal parasites at that time.3,4 These data were very similar to other contemporary data reported by other hospitals in the D.F.5
Distribution by age of patients positive for Giardia in the Hospital Infantil de México Federico Gómez (HIMFG) in 1992 was as follows: 21.4% in infants, 41.7% in pre-school children, 27.9% in students and 9% among adolescents. When a study was done for single or multiple parasitosis, 60.8% presented as single parasitosis, 27% were associated with another intestinal parasite, and 12.2% were accompanied by gastrointestinal parasites. When 183 children who were analyzed separately and whose principal reason for consultation was abdominal pain and diarrhea, the results were higher, with 62.7% positive for G. lamblia cysts. Frequencies reported for other intestinal parasites at the end of the 1980s and beginning of the 1990s in the parasitological laboratory of the HIMFG were the following: Entamoeba histolytica, 6.8%; Ascaris lumbricoides, 18.1%; Strongyloides stercolaris, 2%; Hymenolepis nana, 15.9%; Trichuris trichiura, 10%; Uncinarias, 1.2%; and Enterobius vermicularis, 1.8%.4 However, Blastocystis hominis, a protozoan whose taxonomy and pathogenicity still create controversy, began to be reported as an intestinal parasite around 1995 and quickly replaced G. lamblia6-8 for first place in frequency of occurrence. Another emergent group of protozooses were the intestinal coccidian led by Cryptosporidium sp., which was recognized as a human pathogen in 1976. Since then, its reporting has increased, particularly in individuals who are immunocompromised and due to epidemic outbreaks as a result of ingestion of contaminated water. HIV impacted its diagnosis showing a considerable increase.9,10 However, in the HIMFG, its report and association with diarrhea increased until the end of the 1990s.11,12
Currently, reports of helminthiosis have not disappeared, but isolated cases of hymenolepiasis and ascariosis have been possible during the last year. The former proposition prompts the following questions: is there a transition in the type and frequency of parasitosis? And what are the genera that currently have an effect on the pediatric population of a third-level care hospital? The objective of this work was to determine the frequency of parasites and commensals per year as well as to document the existence of a transition between the incidence of intestinal parasites in a third-level care pediatric hospital from 1990-2010.
2. Methods
2.1. Study period
The study period was limited to the months of January 1990 and December 2010, using work logs and laboratory reports from the parasitology clinic of the HIMFG. All results of the parasitological tests were taken into consideration: direct microscopic technique, concentration by flotation of Ferreira 1:10, concentration by sedimentation of Ritchie, Kinyoun stain, Graham stain, fresh ameba and Kato-Katz. The report of the genus and species of the parasite or commensal or their association reported at the time of the diagnosis were considered.
2.2. Data collection and analysis
Results according to patient and laboratory technique were recorded in daily logs of tests retained in the parasitological laboratory of the HIMFG. Data were collected by the corresponding counting and recording for each year. The results of the parasites reported are captured and processed in a database developed in Excel 2010 (Microsoft Corp.) Among the findings of the parasite stool test diagnosis, there is always the possibility of finding commensal organisms. These were also reported at the time of the diagnostic report by the laboratory and is also considered and discussed in this work. Descriptive statistics were done based on frequency of distribution of the parasite and commensal report per year.
2.3. Plan of analysis
To estimate the difference of proportions between the decades studied, Pearson χ2 was used with a confidence interval of 95% (95% CI). For comparing the difference of proportions, the hypothesis of contrast was used where Ho was the equality of the proportions between the decades studied and Ha represented its difference.
3. Results
3.1. Parasitological diagnosis
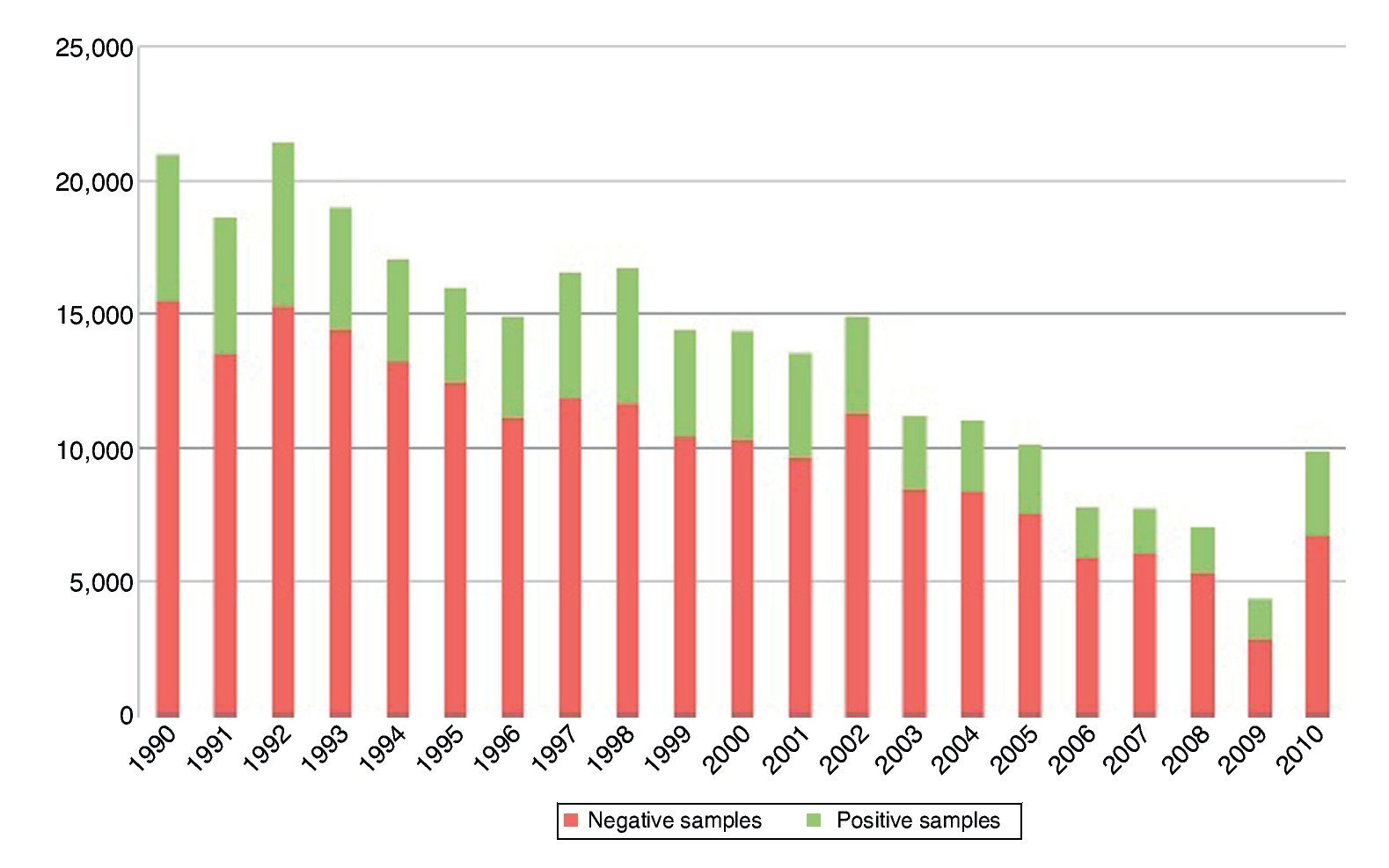
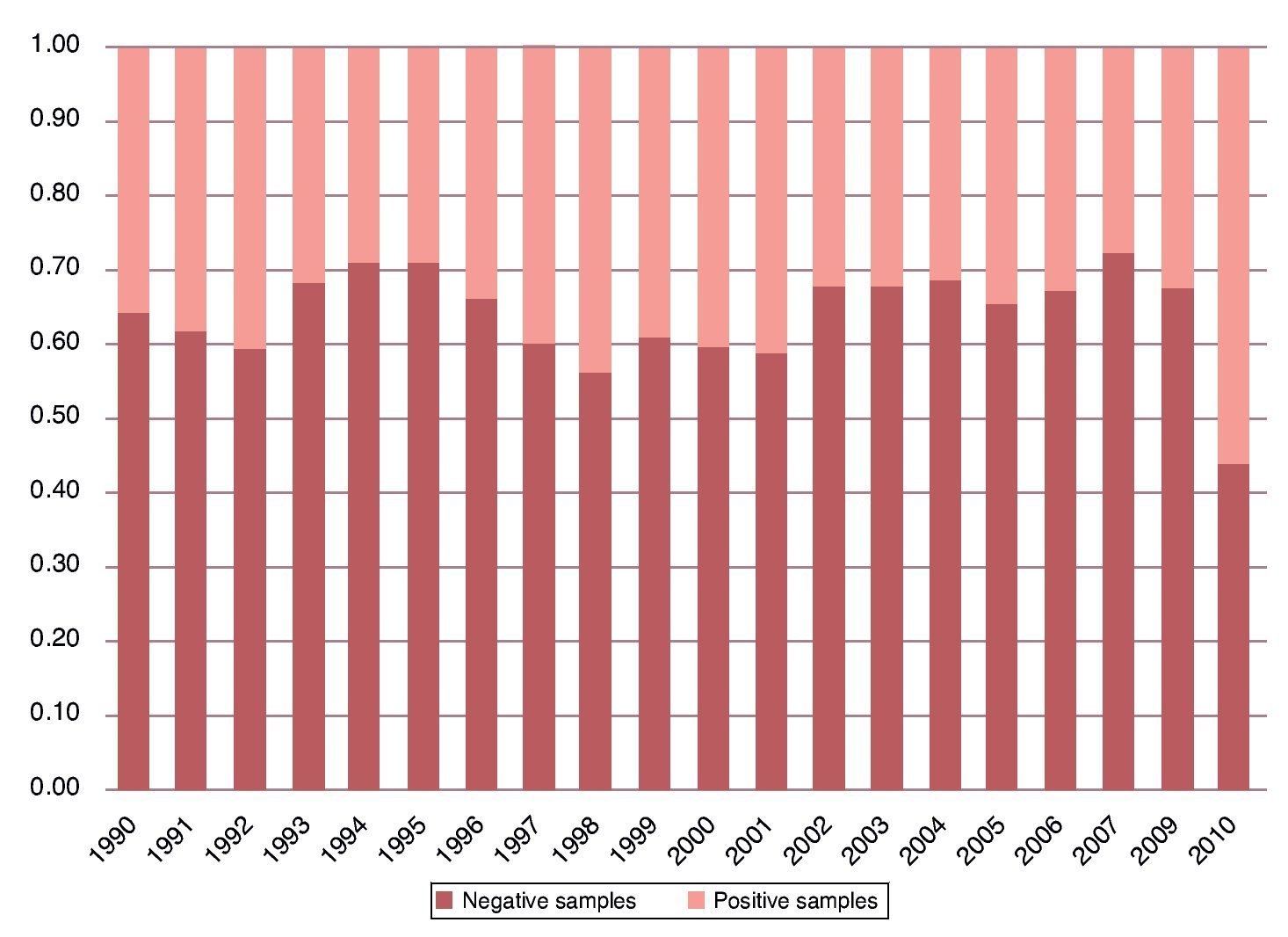
Taking into consideration the two decades studied, the total sample number was 211,600. The average number of samples processed per year was 10,100, with a standard deviation close to 3500 (Fig. 1). The percentage of observation of structures, both parasitic as well as commensal, was 37.73% of the total sample. The percentage observed of parasites alone was 21.4% in the two decades (Fig. 2).
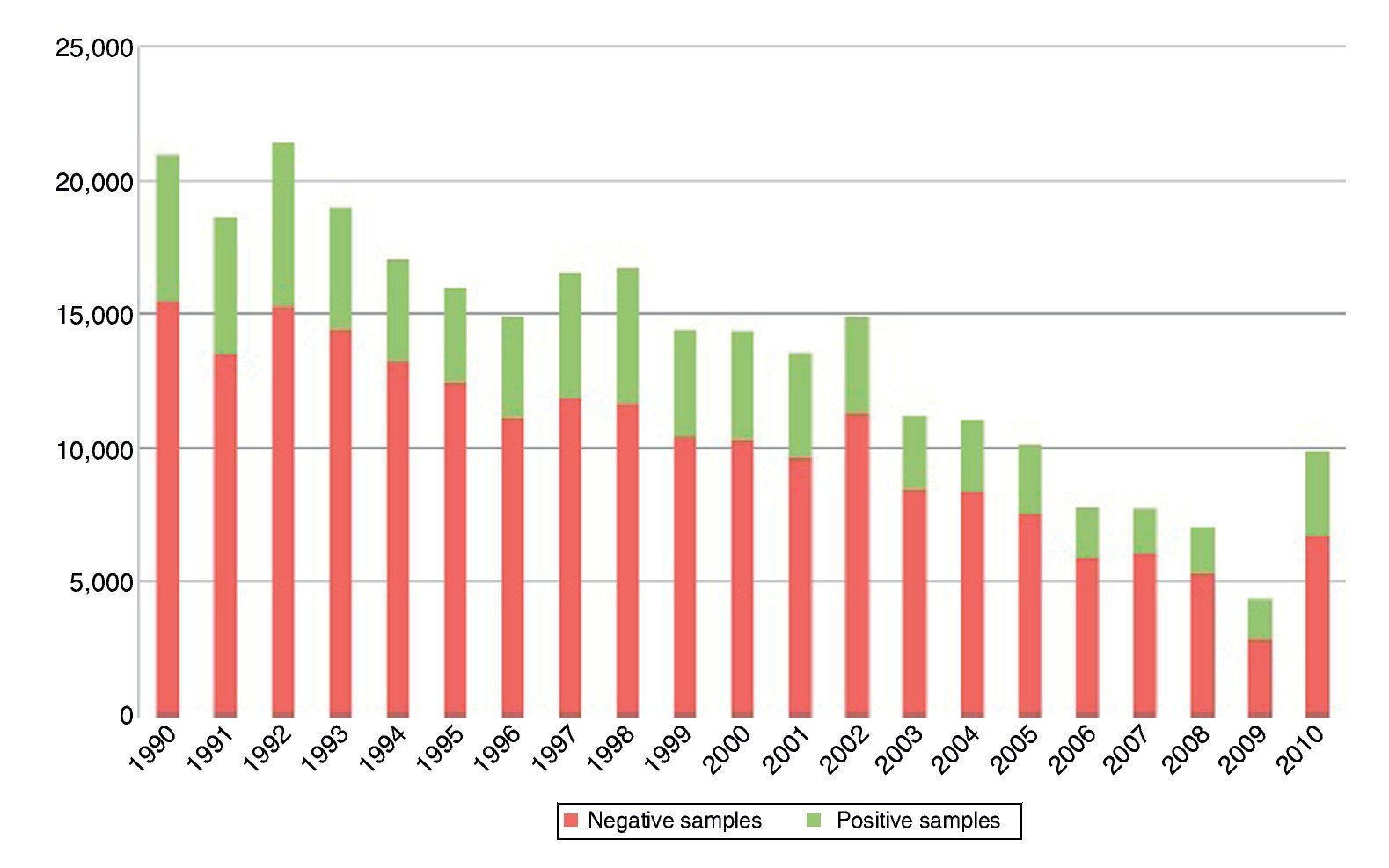
Figure 1 Frequency of positivity to parasitosis and commensals according to year.
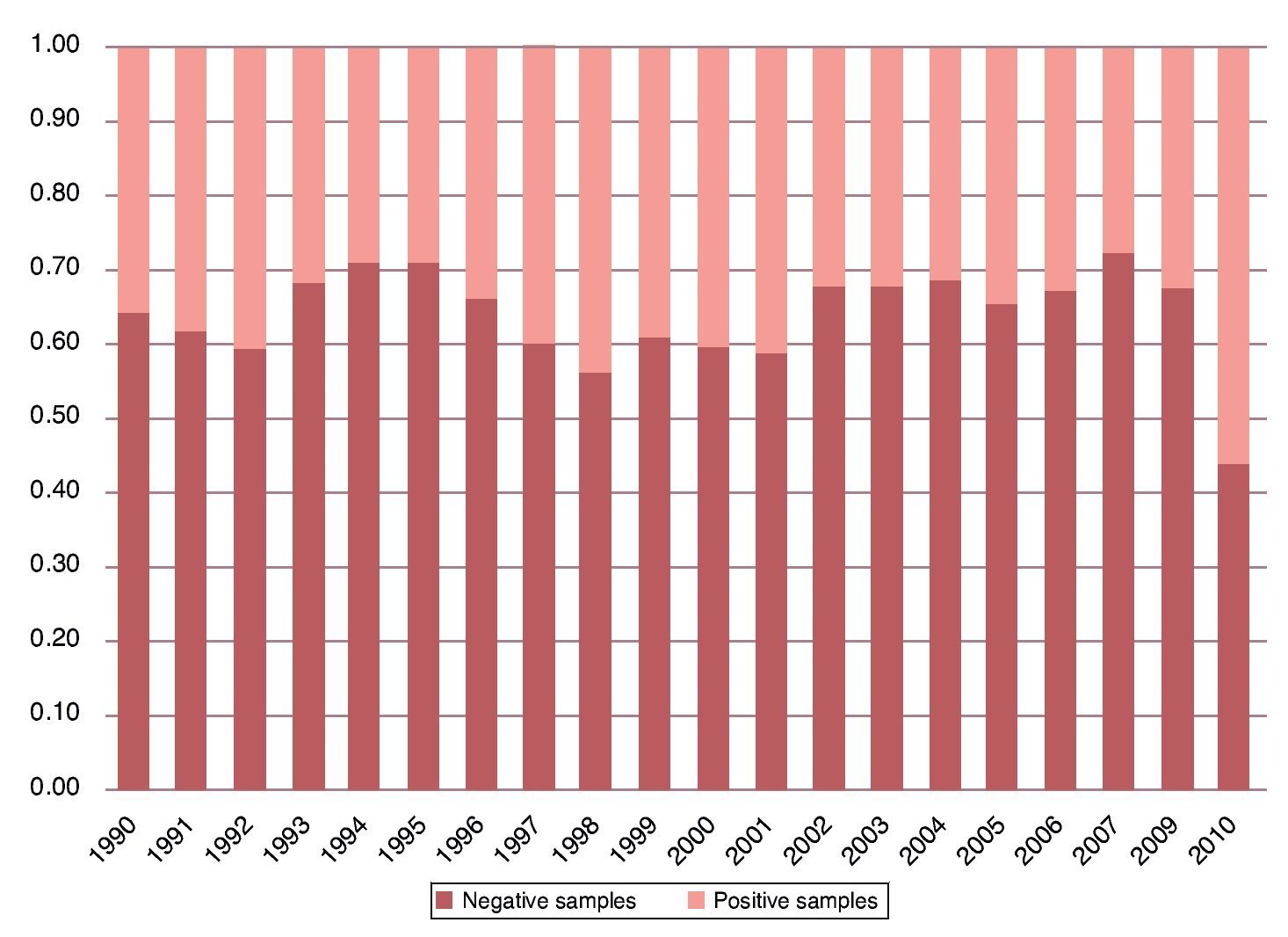
Figure 2 Distribution of proportions according to year.
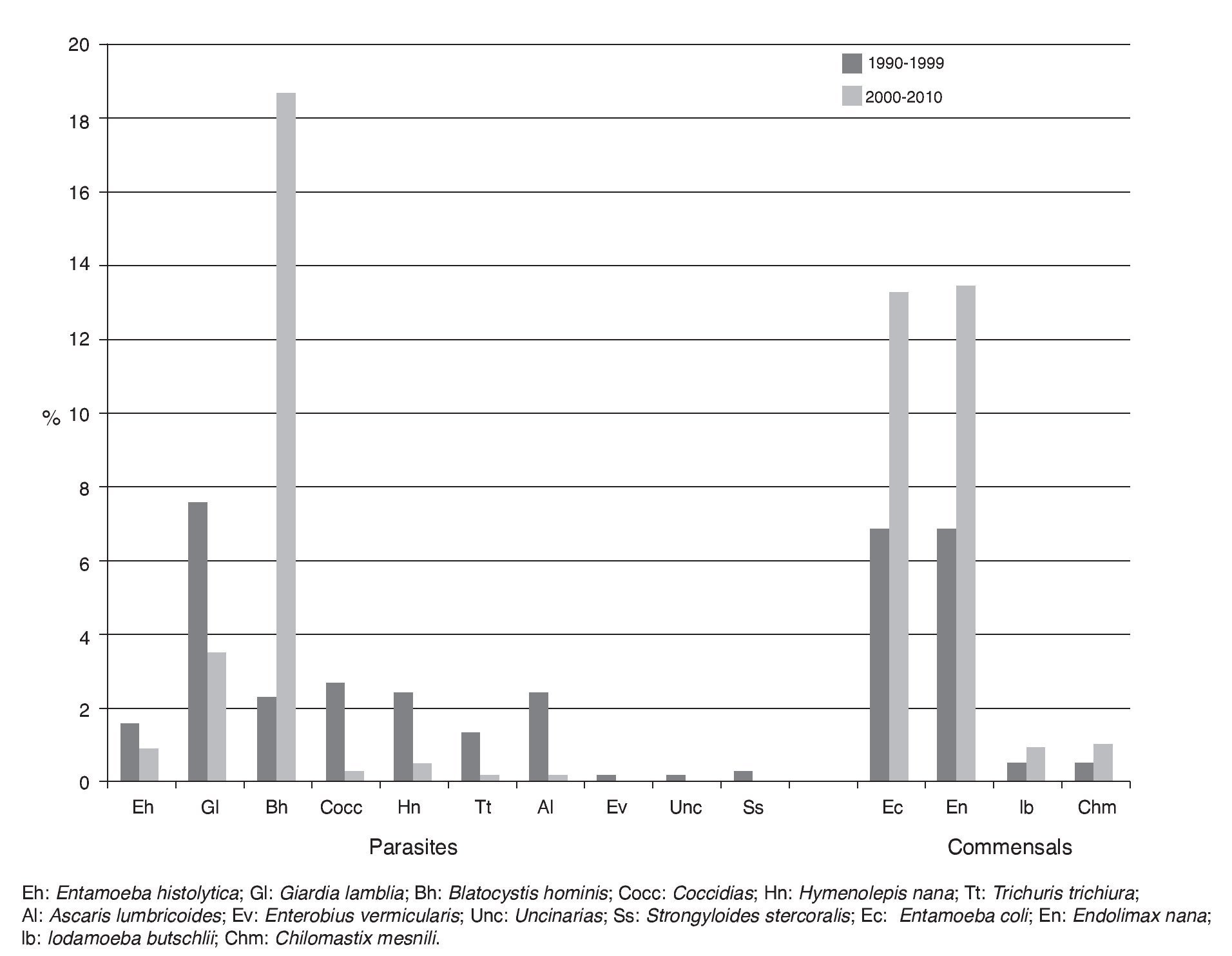
The protozoan parasite observed with greatest frequency was Blastocystis hominis (21.8%) followed by G. lamblia (17.3%), Cryptosporidium (5.4%), and finally E. histolytica (3.9%). It should be noted that 73.7% of the total positivity for Cryptosporidium sp. was reported between 1996 and 1999. Until 1998 there were no reports of B. hominis, but positivity has shown a sustained increase. So much so that from 1999 it displaced G. lamblia from first place among the protozoans. The most common commensals were Endolimax nana (18.6%), E. coli (16.4%), Chilomastix mesnili (1.3%) and Iodamoeba buschtlii (1.09%) (Fig. 3).
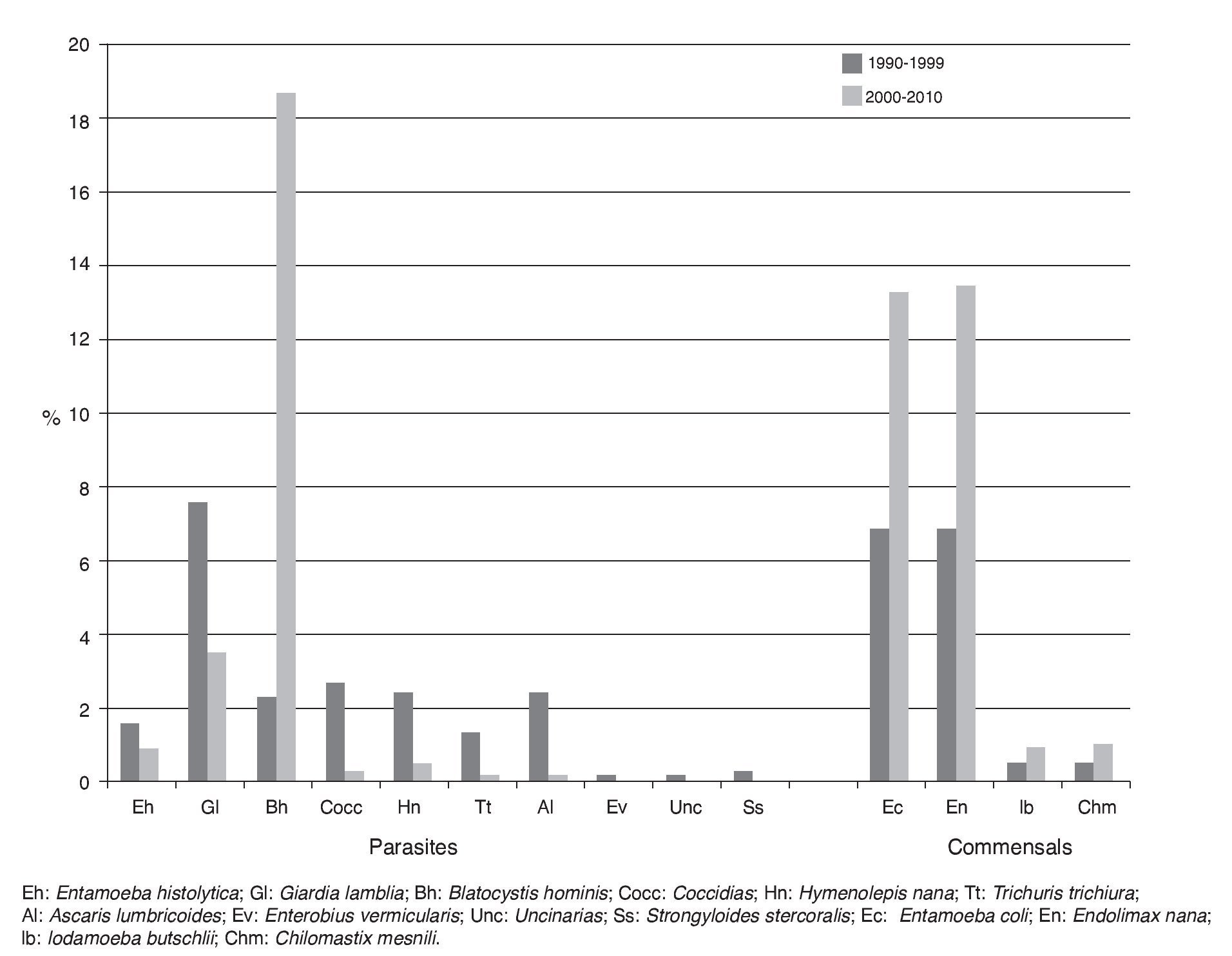
Figure 3 Distribution of frequencies according to decade and type of parasite or commensal.
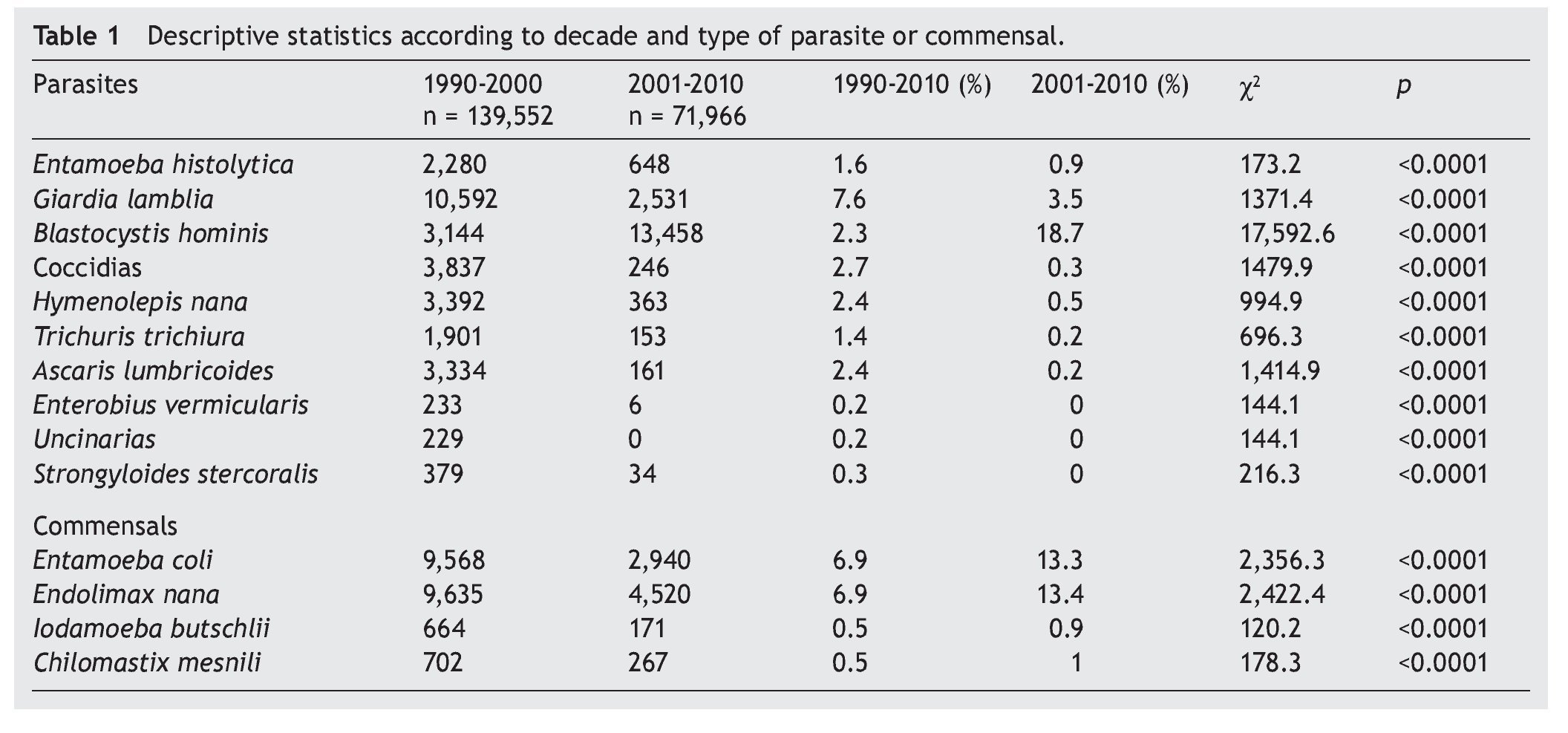
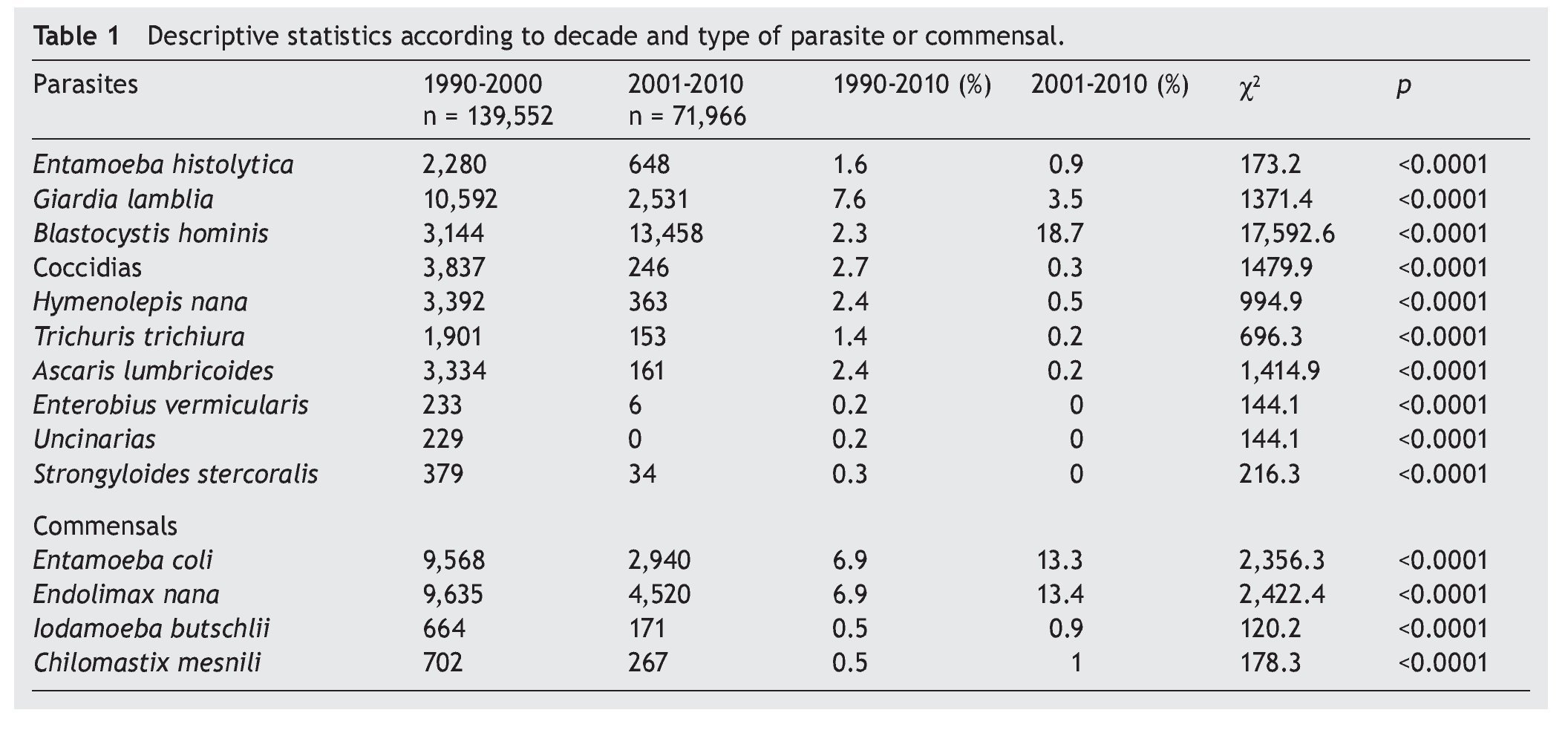
With regard to the presentation of parasitosis alone, it was identified in 65% of the cases, 13% were associated with other parasites and 22% associated with commensals. With regard to the distribution of parasites by gender, 53% corresponded to males and 47% to females. Positivity for platyhelminthes was 1.8% and for nematodes was 2.9%. It should be noted that 99.4% of the cestodiosis was attributed to the finding of Hymenolepis nana, whereas 54.3% of the nematodiosis was due to Ascaris lumbricoides followed by Trichuris trichiura (32%). The highest frequency of helminths corresponded to H. nana (4.9%) followed by Ascaris lumbricoides (4.6%), T. trichiura (2.7%), Strongyloides stercolaris (0.5%), Enterobius vermicularis (0.3%), Uncinaries (0.3%) and in last place, Fasciola hepatica (0.03%). It should be noted that the 92.3% positivity to helminthiosis was due to a recount up to the year 1999, to later show a remarkable decrease. Table 1 shows the descriptive statistics per decade and type of parasite or commensal.
4. Discussion
The trend in the behavior of intestinal parasitic infections throughout the two decades studied showed changes, both in frequency as well as in the genus and species of the agents, which were reported at this level of pediatric health care. These changes can be clearly observed in the frequency of distribution graphs. The change in parasitosis is clear, both for protozoans as well as helminths. In the case of protozoosis, a frank displacement was observed between genus and species. G. lamblia changed from being the protozoan of highest frequency reported to second place when B. hominis was recognized as an intestinal pathogen and was intentionally searched from the second half of the 1990s.13-16
In the case of E. histolytica, although it never showed a significantly high number, a decrease in its diagnosis has been recorded with the actual consideration and adherence to the WHO criteria of reporting it as E. histolytica/dispar and not only as E. histolytica (as was done towards the beginning of the last decade).17-19 This fact attests that increasingly a better parasitic diagnosis can be established. For example, for cases where it is desirable to arrive at the level of the species and the morphology does not allow it, current techniques can be used with an immunological or molecular basis that allow for the correct identification of the parasite in order to lead the way for adequate treatment and control.
Helminthiosis reveals that, even from the decade of the 1990s, these were not found among the most common parasitosis. As a result of personal communications it is known that in previous decades these occupied a dominant place in the report of the diagnosis of this service and, in general, in the country.20-22 Unfortunately this evidence was not documented. In this study the report of helminths is basically reduced to isolated cases of intestinal ascariosis and hymenolepiosis, and the trend towards a decrease of these cases has been consistent up to now.
This parasitic transition can be supported on at least three acts that have been added over the years. The first two are attributable to health policy because it considered the typical intestinal parasitosis (giardiosis, amebiasis or helminthiosis) as a priority public health issue, and public health strategies were implemented to reduce their incidence. Historically, the first fact that operationally impacted the open population were the campaigns of mass deworming from the decade of the 1990s23-25 when the government began to offer a single antiparasite dose to each child vaccinated during the national health weeks. This action has warranted both supporters as well as detractors.26,27
Over time, it has been demonstrated that although the intestinal parasite populations were abated, they have not been eliminated completely, and the surviving populations (although diminished in quantity) preserve their reproductive potential and are sufficient to be maintained endemically.28 The following health policy with impact in the control of enteroparasitosis was promoted worldwide by the WHO at the beginning of 2000.29 The strategy was to provide health education together with the introduction of health infrastructure measures to vulnerable areas and therefore endemic for parasitosis. In our country, the program of “firm footing” against geohelminthiosis has had a great impact on the incidence and prevalence of these parasitoses.30,31 The third argument that could justify the parasitic transition is the fact that this study was developed in a third-level institution. In this hospital, the patients referred were previously screened in institutions of lower levels of care. For these, typical intestinal parasites were filtered from the time of diagnosis until treatment, such that in general, upon arriving at the third-level care institution, we are dealing with concomitant findings as a result of other diseases of different etiologies (almost always originating from chronic-degenerative, oncological, genetic or autoimmune diseases).32 In another vein, increase in the frequency of non-communicable diseases in the pediatric population is documented, which is the target population of care in this hospital and promotes conditions for development of opportunistic organisms including some protozoans such as intestinal coccidia and microsporidia.33-35 These protozoa had an upsurge in frequency and reporting but, at the time of this study, showed a downward trend. This is associated with different factors such as the cellular immune response of the patients, which has improved along with the experience acquired by physicians with regard to antiretroviral drugs (particularly in the case of HIV), so that these parasitoses become less common over time.36
Although parasitological diagnosis should be performed routinely at the institutional basic level of care, this diagnosis should also be kept in mind at the tertiary level of care. This report demonstrates that structures were identified, both parasitic as well as commensals, in 37.73% of the samples analyzed. The report of commensals in this population is no less important because it indicates fecal contamination in the environment of the patient. Recommendations for the surveillance of hygienic/dietary conditions should be provided.
It is very important to know the frequency and distribution of parasites in the pediatric population. Considering that HIMFG is a leader in medical care, it is imperative to know the behavior of parasitic diseases associated with complex diseases treated at a third-level care facility. The generation of epidemiological information is necessary to understand the behavior of parasites and their variations over time.
Ethical disclosures
Protection of human and animal subjects. The authors declare that the procedures followed were in accordance with the regulations of the responsible Clinical Research Ethics Committee and in accordance with those of the World Medical Association and the Helsinki Declaration.
Confidentiality of data. The authors declare that no patient data appears in this article.
Right to privacy and informed consent. The authors declare that no patient data appears in this article.
Funding
None.
Conflict of interest
The authors declare no conflict of interest of any nature.
Received 27 May 2015;
accepted 1 June 2015
☆ Please cite this article as: Tapia-Romero R, Martínez-Méndez LG, Dávila-Solís BL, López-Martínez B, Parra-Ortega I. Transición parasitaria: experiencia en un hospital pediátrico de tercer nivel (1990-2010). Bol Med Hosp Infant Mex. 2015. http://dx.doi.org/10.1016/j.bmhimx.2015.06.002
* Corresponding author.
E-mail:i_parra29@hotmail.com (I. Parra-Ortega).