


Introducción: El síndrome de Down (SD) o trisomía 21 es la causa genética más frecuente de retraso mental. Clínicamente presenta una serie de características bien definidas. Se ha asociado la edad materna avanzada con la presencia de SD.
Métodos: Se conjuntaron las bases de datos de los certificados de nacimientos vivos y de muerte fetal. Se seleccionaron los códigos con base en la Clasificación Internacional de Enfermedades décima revisión (CIE-10) del capítulo XVII: «Malformaciones congénitas, deformidades y anomalías cromosómicas».
Resultados: Se construyó una base de datos con 8,250,375 nacimientos ocurridos durante el periodo 2008-2011. El 99.2% correspondió a nacidos vivos y el 0.8% a defunciones fetales. Se diagnosticaron 3,076 casos con SD.
Conclusiones: La importancia de este trabajo radica en iniciar una vigilancia epidemiológica del recién nacido con SD a nivel nacional y por entidad federativa, utilizando sistemas de información censales disponibles en el país a partir del 2008. Se observó un aumento en el riesgo de tener un hijo con SD a partir de los 35 años de edad materna, como ha sido reportado en otros estudios.
Background: Down syndrome (DS) or trisomy 21 is the most common genetic cause of mental retardation with the clinical presentation of a series of well-defined characteristics. Advanced maternal age has been associated with DS.
Methods: The databases of all the certificates of live births and fetal deaths in Mexico were combined. Codes based on the International Classification of Diseases 10th Revision (ICD-10) in Chapter XVII ‘‘Congenital malformations, deformations and chromosomal abnormalities’’ were selected.
Results: A database of 8,250,375 births during the period 2008-2011 was constructed: 99.2% were live births with 0.8% of fetal deaths and 3,076 cases diagnosed with DS.
Conclusions: The importance of this report is to initiate an epidemiological surveillance of newborn cases of DS nationwide and by state using census information systems available in the country since 2008. An increased risk has been observed for having a child with DS since the mother is ≥ 35 years, as has been reported in other studies.
1. Introduction
Down Syndrome (DS) or trisomy 21 is the best known human chromosomal disorder. It was described in 1866 by John Langdon Down.1 It is the first human chromosomal disorder described caused by the presence of an additional chromo-some 21.2 There may also be a partial trisomy of chromosome 21 of the q22.1 distal band at the proximity of q22, which corresponds to the critical region for DS.3 It has the highest frequency in live newborns and constitutes the most common genetic cause for mental delay. It causes spontaneous abortions and only 20-25% of newborns survive at birth.4
DS has a series of clinical characteristics such as brachycephaly, ascending oblique palpebral fissures, epicanthus, Brushfield spots, dysplastic ears, depressed nasal bridge, narrow palate, short neck, excess skin of the back of the neck, hyperflexibility, wide hands, brachydactyly and trans-verse palmar fold. The main characteristic is mental delay. There may also be congenital heart diseases in up to 50% of the cases, frequent respiratory infections and gastrointestinal tract obstruction. There is an increased risk of acute megakaryoblastic leukemia, and Hirschprung and Alzheimer diseases.5
Advanced maternal age is the risk factor that has been primarily associated with DS.6 Oogenesis starts in the third month of intrauterine life in females and the meiotic division stops, which makes possible the segregation of the chromosomes to be altered7; 90% of the cases of trisomy 21 originate in the first maternal meiotic division; the remaining 10% are of paternal origin. The risk of recurrence for numeric alterations is 1%. The risk of DS increases with maternal age—the risk of DS at maternal age 30 years is 1/1,000 and at maternal age of 40 years is 9/1,000.1
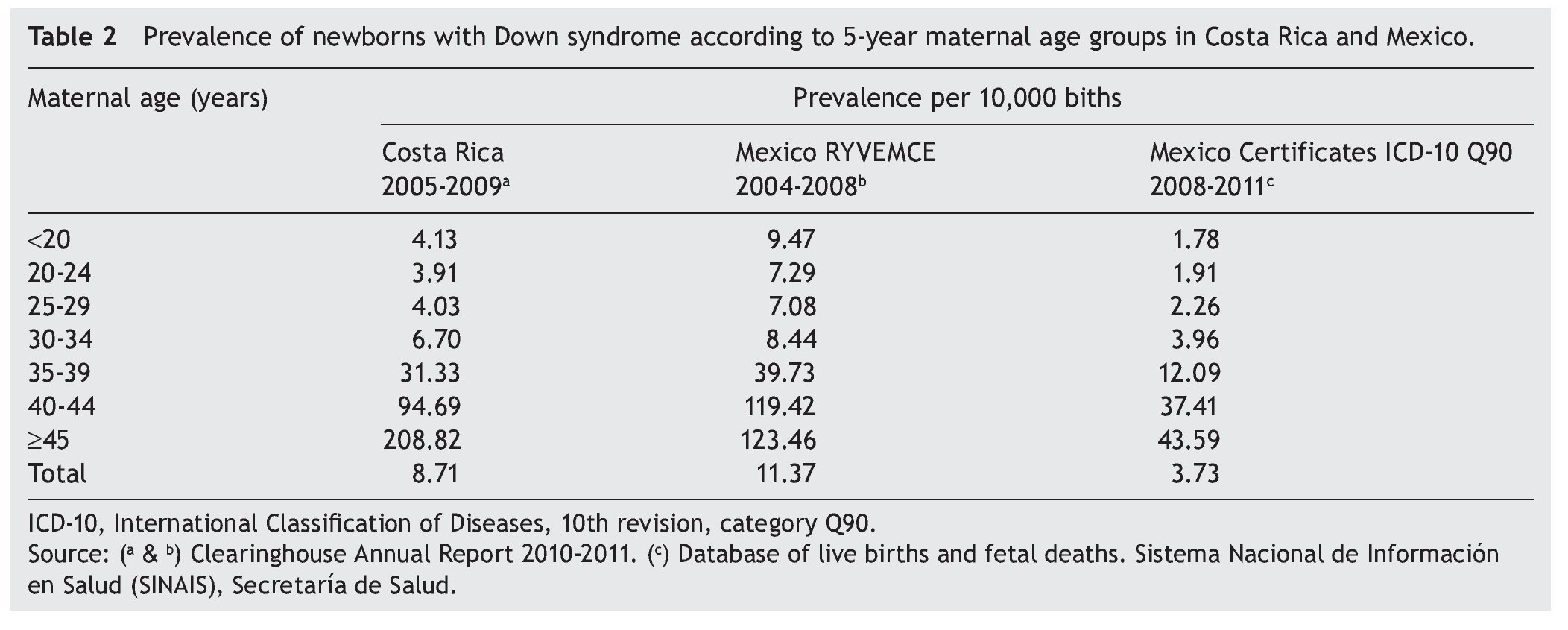
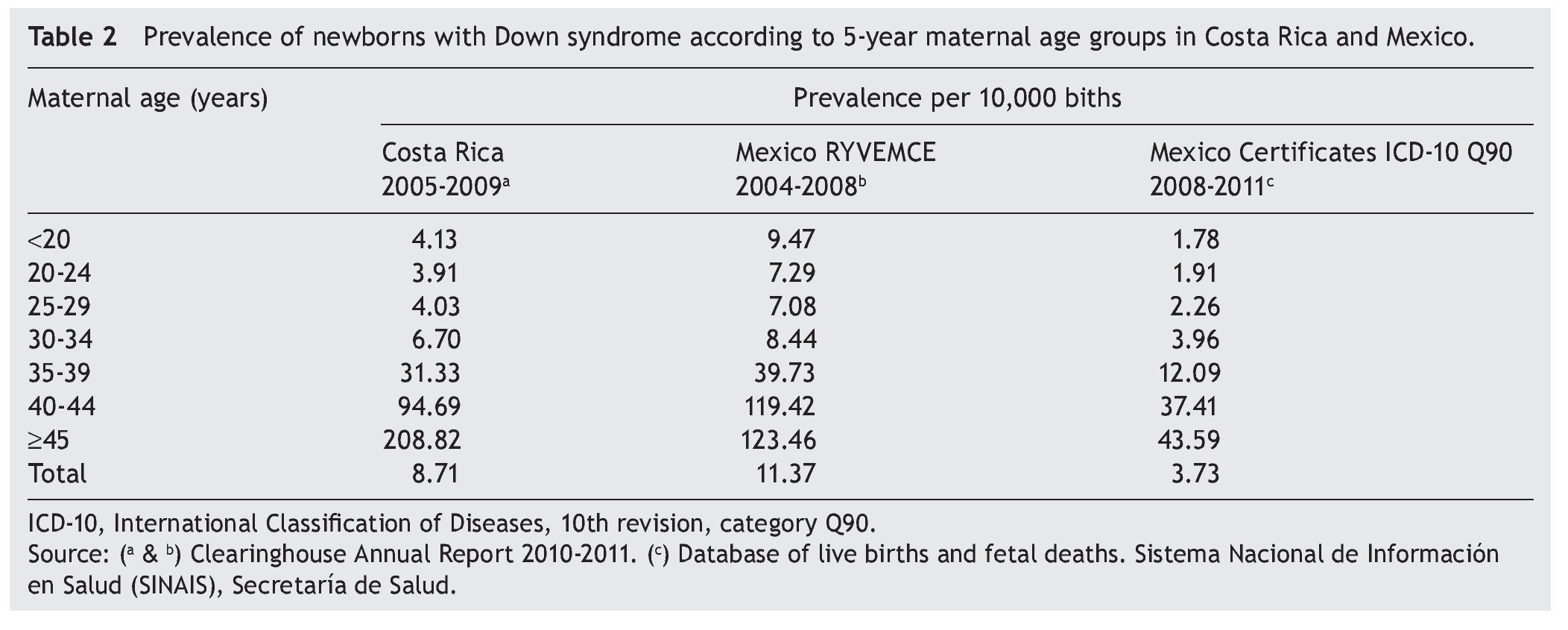
The Registry and Epidemiological Surveillance of Congenital Malformations (RYVEMCE) reported a prevalence of 11.37/10,000 births for the period 2004-2008 in the Mexican population.8 Costa Rica, during the period from 2005-2009, registered a prevalence of 8.71/10,000 births. This registry was population based and covered 98% of the 75,000 annual births and is classified as a national registry.9
In Mexico, from 2004-2008, the RYVEMCE obtained information from 21 hospitals representing 11 cities in Mexico. Participation was voluntary. The annual number of births was 62,000, which corresponded to 3.5% of all births in Mexico. Included were stillbirths of 20 weeks or more of gestation or 500 g birth weight.8 Hospital characteristics included in the information system are unknown.
Other countries that use national population bases are Canada with 330,000 annual births and a rate of DS of 14.41/10,000 births,10 Czech Republic with 110,000 births and a rate of DS of 21.03/10,000 births,11 Finland with 60,000 births and a rate of DS of 29.94/10,000 births,12 Hungary with 100,000 births and a rate of DS of 17.40/10,000,13 and Switzerland with 100,000-120,000 births and a rate of DS of 28.91.14
The estimated ratio of cases of DS is from 1/1000 to 1100 live births according to the World Health Organization (WHO).15 The Department of Health, through the Centers for Gender Equality and Reproductive Health, in its Technical Guidelines for Complete Care of the Person with DS, reports that in Mexico there is an estimated one case of DS/650 live newborns.16
Registries that have been established in Mexico have been based on isolated hospital samples and there is no national coverage in any of these hospitals. During mid-2007, the Department of Health established at the national level a subsystem of information on births (SINAC) through the “birth certificate” (live). This is an official, nontransferable individual document that certifies the live birth at the time of its occurrence, providing the mother with this proof.17 This subsystem, by having a registry of all births in the country, allows for estimating the prevalence of DS and other congenital malformations, as well as to have the information according to federal, municipal and locality entities.
In this study, data present in the recently implemented subsystem were analyzed and compared with population database registries. For this, the national prevalence for DS by 5-year maternal age groups was estimated. The objectives of this study were the following:
— Estimate the prevalence of births with DS nationally by federal entity and by 5-year maternal age groups based on the national registries of live births and fetal deaths in Mexico from 2008-2011
— Estimate the ratio index between cases and non-cases of DS by 5-year maternal age groups and by federal entity
— Compare the prevalence of DS with other studies
2. Methods
Databases from all live birth and fetal death certificates registered in Mexico nationally for the period from 2008-2011 were combined in relation to the common variables. The universal study was comprised based on live births and deaths from 22-45 weeks gestation and with a birth weight ≥500 g. Also taken into consideration was that the mother’s actual residence was Mexico. For the first two variables, cases with incomplete data and foreign residents were excluded from the study.
With regard to the diagnosis of DS, codes were used from the International Classification of Diseases, 10th Revision (ICD-10),18 chapter XVII “Congenital malformations, deformi ties and chromosomal anomalies”. These were classified according to category of three characters such as Down’s syndrome (Q90) and by subcategories of four characters such as trisomy 21 due to lack of meiotic disjunc tion (Q90.0), mosaic trisomy 21 due to lack of mitotic disjunction (Q90.1), trisomy 21 due to translocation (Q90.2), and unspecified DS not (Q90.9). It was decided to use with the first diagnosis noted on the birth certificates and the basic cause of fetal death. According to the birth certificates a diagnosis was made in the years 2008 and 2009 and two diagnoses in the years 2010 and 2011 for the variable “congenital anomalies, diseases or lesions of the live newborn”. Fetal death certificates only listed the basic cause of death. Similarly, maternal age at the time of the birth was included in the analysis.
3. Results
A database was constructed with 8,250,375 births that occurred nationally during the period from 2008-2011; 99.2% corresponded to live newborns and 0.8% to fetal deaths. The number of resultant congenital malformations was 62,871; of these, 91.4% were live newborns and 8.6% fetal deaths. The proportion of congenital malformations in live newborns was 0.7% and for fetal deaths was 8.3% in relation to the corresponding total. Distribution of congenital malformations according to gender was 55.9% for males and 43.3% for females; in 0.8% these were not recorded. The general prevalence of resulting congenital malformations was 76.2/10,000 births. According to gender it was 83.5 and 67.6 for males and females, respectively.
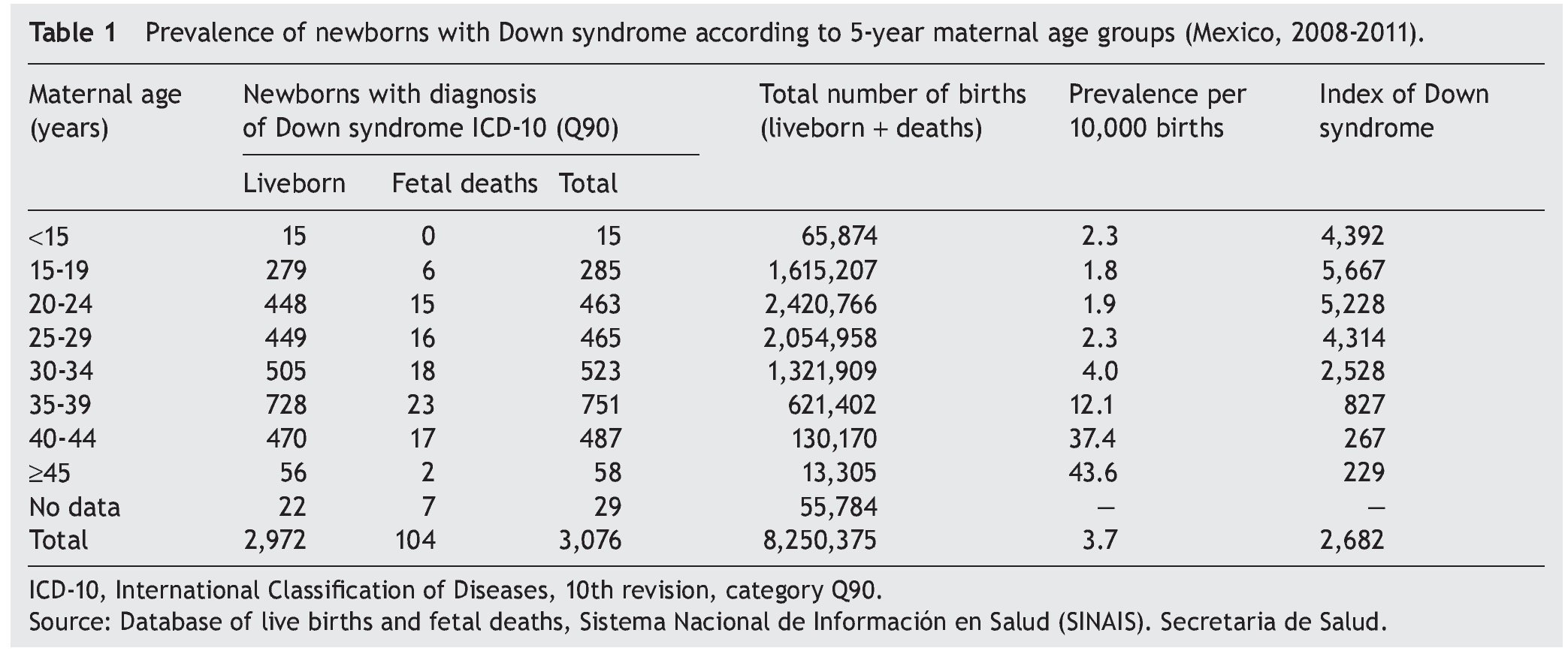
There were 3076 cases with DS diagnosed (Table 1) that represented 4.9% in relation with the total congenital malformations. Of these, 96.6% were live newborns and 3.4% fetal deaths. According to gender, 1451 were males (47.2%) and 1619 females (52.6%). In six cases the information was not recorded (0.2%).
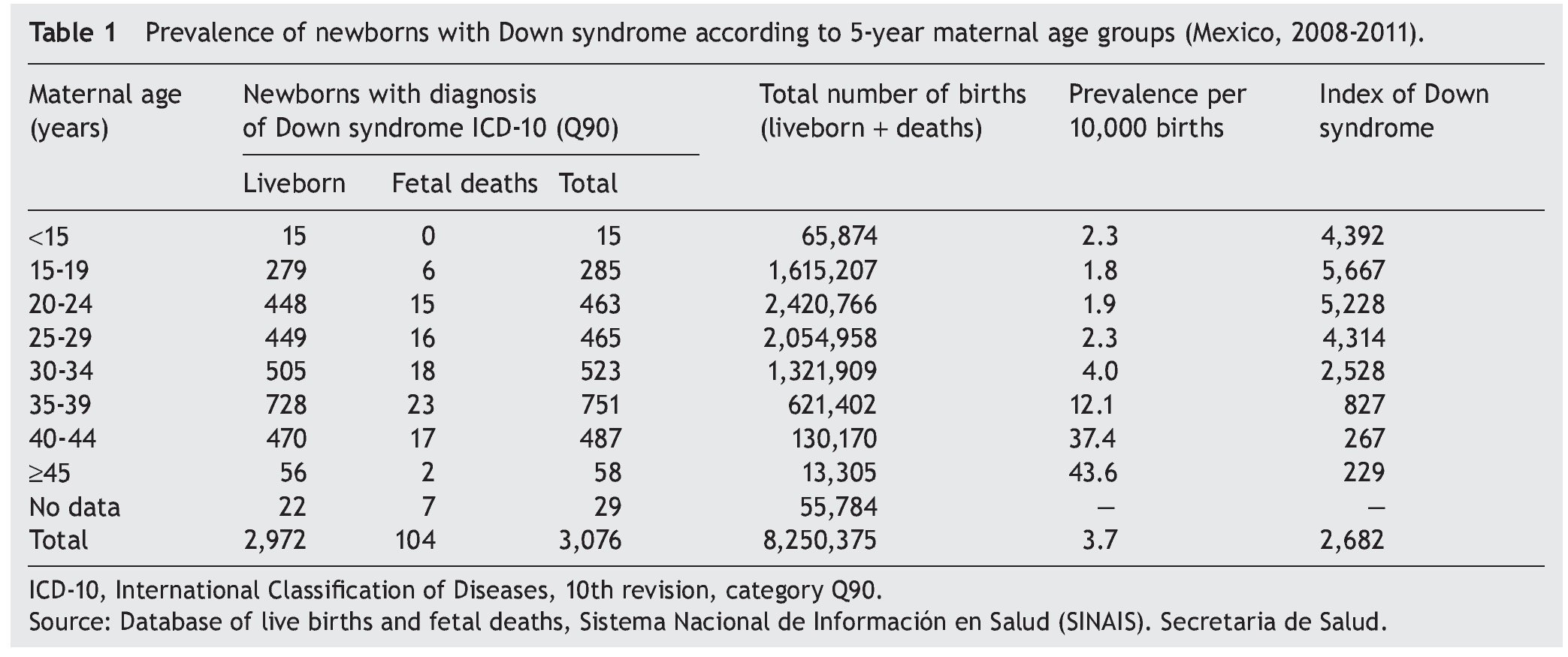
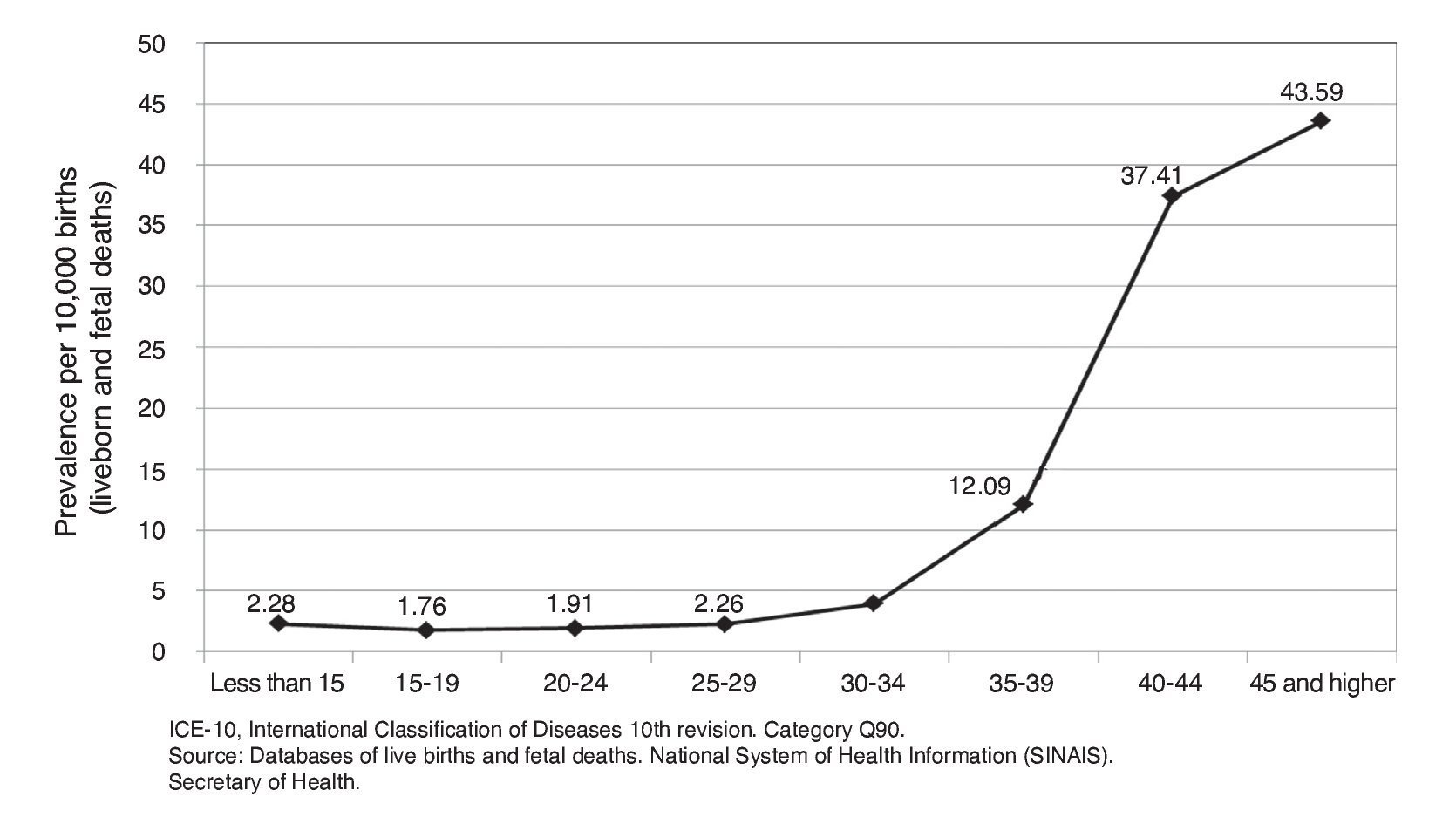
The prevalence of DS was 3.73/10,000 births during the analysis period. With respect to the results for 5-year maternal age groups, the higher the age the higher the rate of DS. The last three age groups were notable: 35-39 years, with 12.09/100,000 births; 40-44 years with 37.41/100,000 births; and >45 years with 43.59/10,000 live births (Fig. 1). These three groups account for the 42.1% of the cases.
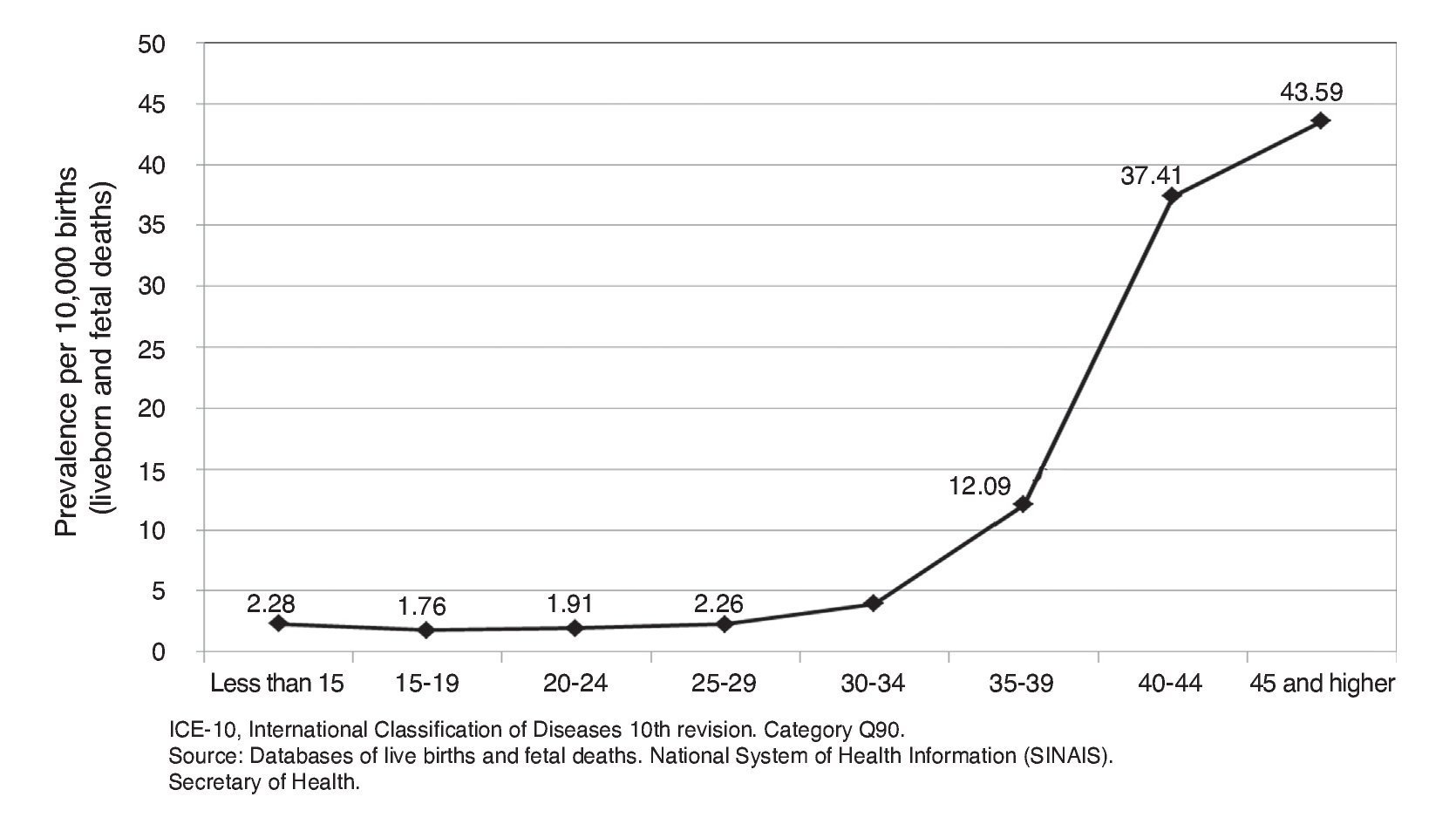
Figure 1 Prevalence of newborns with Down syndrome according to maternal age groups (Mexico, 2008-2011).
The index of DS is the number of births with DS in relation to births without DS of the corresponding age group. It is observed that the opposite occurs for prevalence, i.e., in the younger age group the number of births is greater for a case to present itself. This index at the national level was 1/2682 births (Table 1). The results according to subcategories showed the following: trisomy 21 due to lack of meiotic disjunction (Q90.0), 250 cases (8.1%); mosaic trisomy 21 due to lack of mitotic disjunction (Q90.1), 68 cases (2.2%); trisomy 21 due to translocation (Q90.2), 246 cases (8.0%); and unspecified DS (Q90.9), 2512 cases (81.7%).
When the prevalent numbers of DS according to different sources are analyzed, it was observed that, in Mexico, RYVEMCE for the total recorded a rate of 11.37/10,000 births8 and Costa Rica,9 8.71/10,000 births (Table 2). This is three and two times higher, respectively, to what is reported in this study (3.73). According to maternal age groups the prevalence is very similar.
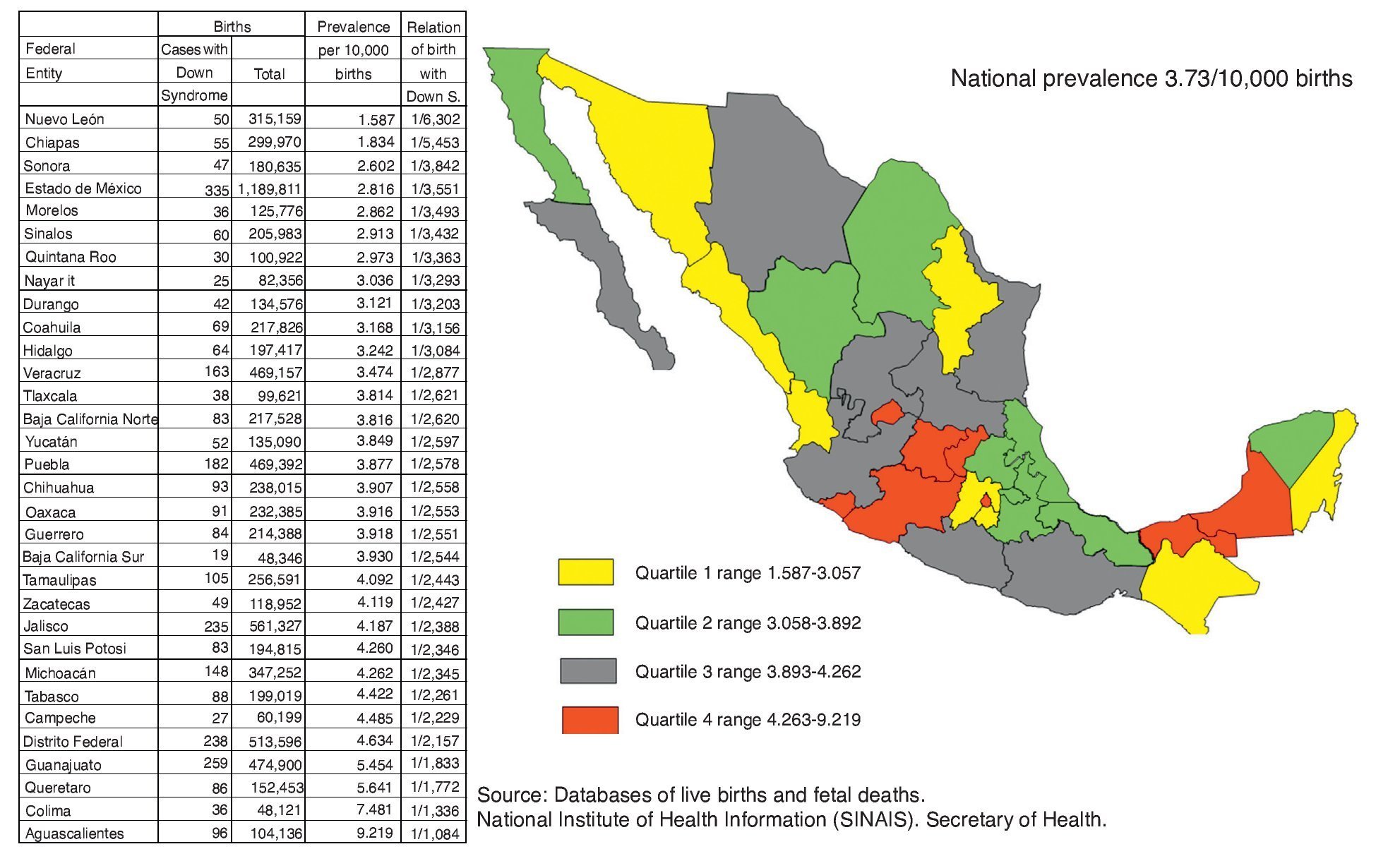
Analysis of the prevalence rates according to federal entity reflects a wide range from 1.587 to 9.219/10,000 births for the corresponding entity (Fig. 2). When the prevalence in the fourth quartile is stratified with a range of 4.262-9.219/10,000 births, in this group the federal entities of Michoacan, Federal District, Guanajuato, Queretaro, Colima and Aguascalientes are located, which correspond to the center of the country and Tabasco and Campeche in the southeast of Mexico, to the Gulf of Mexico. Also, in the third quartile are Guerrero, Zacatecas, Jalisco and San Luis Potosí, also near the central zone (Fig. 2).
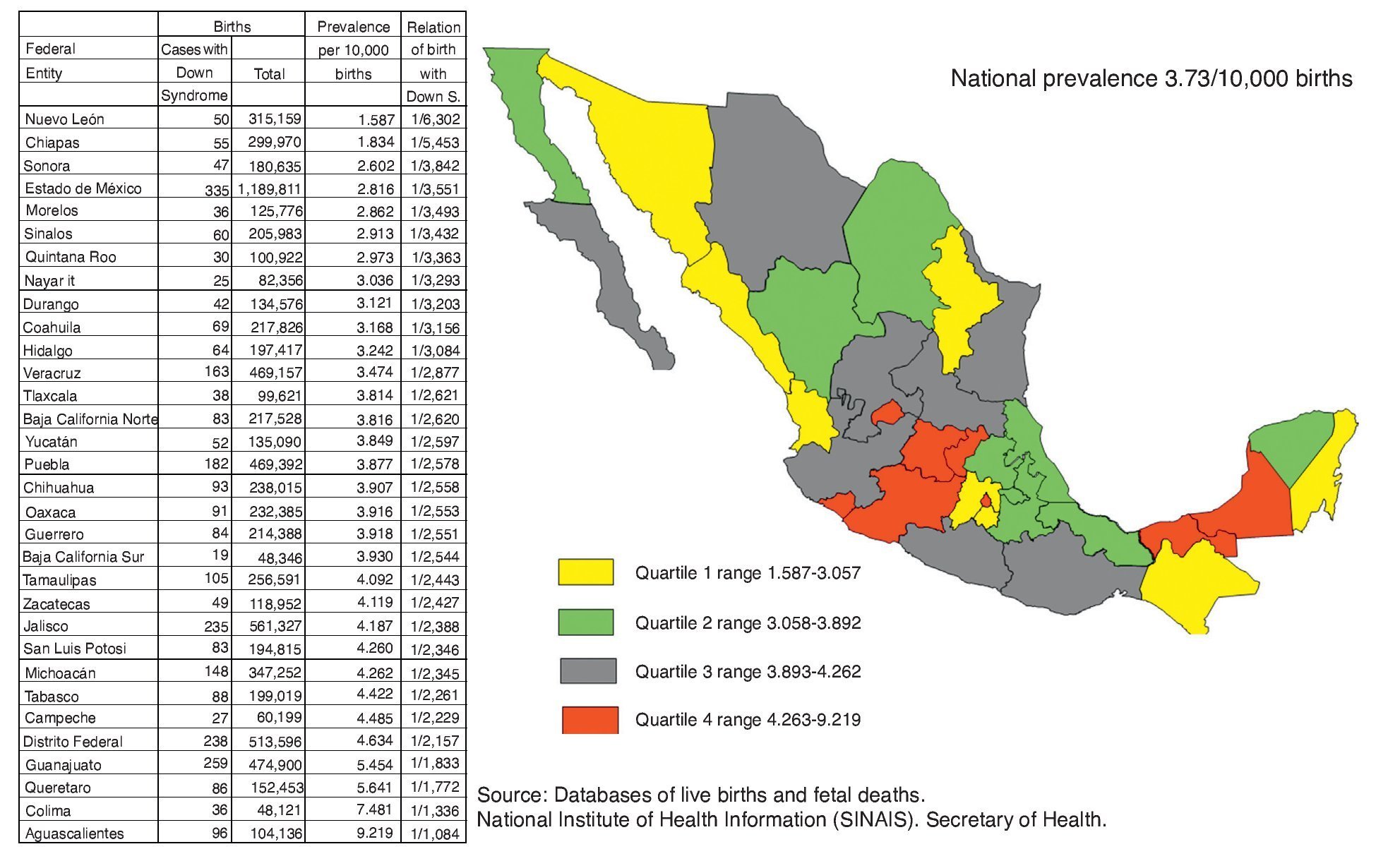
Figure 2 Prevalence of newborns with Down syndrome and relation of cases with Down syndrome vs. cases without Down syndrome according to federal entity (Mexico, 2008-2011).
4. Discussion
The results of the present study correspond to the first 4 years after the Ministry of Health implemented a subsystem of information of live newborn children that contains a variable of “congenital malformations, diseases or injury” at birth and represents a national record of those children born with DS and other pathologies.
The prevalence of DS in the present study was 3.73/10,000 births. This figure results in being three times lower than what is reported by the RYVEMCE8 and two times lower than what is reported in Costa Rica.9 According to maternal age group, the behavior is very similar.
Even when the results of this study with regard to prevalence are discordant with those reported by RYVEMCE in Mexico and with a registry system based on data at the national level similar to the present study, in Costa Rica the data coincide with the same pattern of behavior by age group.
This study showed the increased risk of maternal age for children born with DS for the group ≥35 years of age. This information coincides with the international consensus that the increase in maternal age is associated with an increase in the prevalence of DS. In the group ≥35 years of age, 42.1% of the births with DS are concentrated; 47.2% are found in births of mothers of the ideal reproductive age, 9.7% in those <20 years and 1.0% had no age recorded.
The range in the rate of prevalence of DS according to federal entity is wide. The most elevated rates are present in the center of the country. The differences observed may be due to various reasons: 1) the program was recent in its implementation, 2) possible under reporting due to the difficulty making the clinical diagnosis of DS in the neonatal stage or 3) diversity of the personnel who completed the live birth and fetal death certificates.
The relevance of this work is based on the opportunity to initiate an epidemiological monitoring of the newborn with DS at the national level, federal entity, municipality, and according to locality, using census information systems available in the country.
Even when the validity of the diagnosis was in doubt, in this regard we noted that personnel who completed the live birth certificates were very diverse; 66.9% of the certificates were completed by a physician, whereas 31.7% were completed by other health care personnel, 1.0% by authorized personnel (nurse, midwife, civil authority or other authorized person) and in 0.4% there was absence of data. The figures found in this study are below what is expected. As previously mentioned, this may be due to problems inherent in the new system-wide information system with a national character and a large population as is the case of Mexico. However, its main strength is its population base.
Ethical disclosures
Protection of human and animal subjects. The authors declare that the procedures followed were in accordance with the regulations of the responsible Clinical Research Ethics Committee and in accordance with those of the World Medical Association and the Helsinki Declaration.
Confidentiality of Data. The authors declare that no patient data appear in this article.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Conflict of interest
The authors declare no conflict of interest of any nature.
Received 24 June 2014;
accepted 30 September 2014
* Corresponding author.
E-mail: macarmensierra@hotmail.com (M.C. Sierra Romero).