



Intestinal obstruction in children may be congenital, acquired, intrinsic or extrinsic. Most intestinal obstructions in children are the result of postoperative adhesions. Those caused by anomalous congenital band are extremely rare.
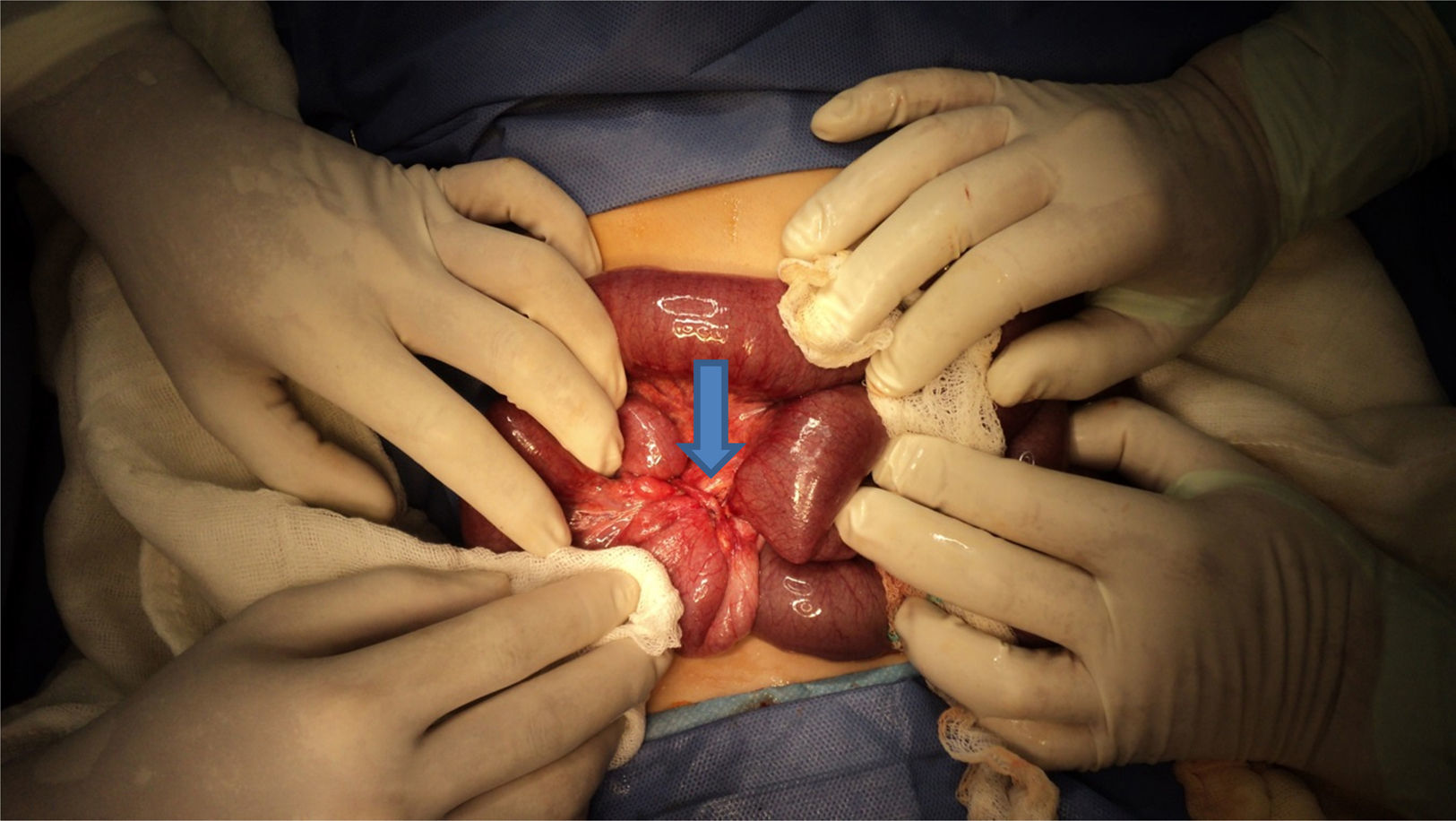
Clinical casePatient of a 1-year-old male, with no previous history of abdominal surgery or trauma. He suffered with vomiting of bile content and loss of appetite at home three days before admission. On physical examination, he was irritable, with abdominal distention, absence of peristalsis and abdominal tenderness, with no signs of peritoneal irritation being found. The blood count reported leucocytosis and the x-rays show dilated small bowel loops, fluid levels and absence of air in rectal ampulla. An open laparotomy was subsequently performed, and the intraoperative findings were consistent with a congenital band extending from the anti-mesenteric wall of the jejunum to the root of mesentery, compressing the ileum at 50cm from the ileocecal valve, causing ischaemia. The band was ligated and divided, with an uneventful postoperative course. He was discharged 4 days later without complications.
ConclusionsThe anomalous congenital band is not associated with abdominal problems, such as remnants of previous laparotomies or embryological structures, such as vitelline vessels or omphalomesenteric yolk duct. These bands seem to have a congenital origin and cause bowel obstruction by trapping between the band and the mesentery. The diagnosis of anomalous congenital band is extremely difficult and no imaging study is useful for the diagnosis, and only exploratory laparotomy or laparoscopy is useful for diagnosis and treatment of this problem.
Las obstrucciones intestinales en los niños pueden ser: congénitas y adquiridas, intrínsecas o extrínsecas. La mayoría de las obstrucciones intestinales en los niños son resultado de adherencias postoperatorias. Las ocasionadas por bandas congénitas anómalas son raras.
Caso clínicoMasculino de un año de edad, sin antecedente de cirugías previas o de traumatismos. Su padecimiento lo inició 3 días previos a su ingreso con vómito de contenido biliar e hiporexia. En la exploración se encontró irritable con: distensión abdominal, peristalsis disminuida y dolor a la palpación en mesogastrio, sin signos de irritación peritoneal. En la biometría hemática se reportó leucocitosis y las radiografías mostraron asas de intestino delgado dilatadas, niveles hidroaéreos con ausencia de aire en ámpula rectal. Se realizó laparotomía exploradora encontrando una banda fibrosa que iba del íleon terminal al mesenterio y que comprimía el íleon a 50cm de la válvula ileocecal con datos de isquemia. Se cortó y ligó la banda fibrosa. Fue egresado a los 4 días después del procedimiento, sin complicaciones.
ConclusionesLas bandas congénitas anómalas son aquellas que no tienen relación con problemas abdominales previos como laparotomías o remanentes de estructuras embriológicas como los vasos vitelinos o el conducto onfalomesentérico. Estas bandas, al parecer, tienen un origen congénito y causan obstrucción al atrapar el intestino entre la banda y el mesenterio. El diagnóstico de la obstrucción intestinal por bandas congénitas anómalas es extremadamente difícil y ningún estudio de imagen ayuda para el diagnóstico, únicamente la laparotomía exploratoria o la laparoscopia son útiles para el diagnóstico y el tratamiento de este problema.
Intestinal obstructions in children can be classified as congenital and acquired, intrinsic or extrinsic. Intrinsic congenital intestinal obstructions include: atresia, membrane, stenosis, ileus and meconium plug obstruction. Extrinsic congenital obstructions can be caused by: annular pancreas, volvulus, internal hernia, intestinal duplications, retroperitoneal tumours and anomalous congenital band or embryonic remnants.1 Invagination and adhesions, and postoperative adherences or secondary inflammatory problems are the principal causes of extrinsic acquired intestinal obstructions.
Most intestinal obstructions in children are the result of postoperative or inflammatory adherences. Fewer than 1% are extrinsic congenital and of these, obstructions caused by anomalous congenital band are extremely rare.2–4
A literature review was carried out for this study from the following bases: MEDLINE, ENBASE, COCHRANE LIBRARY and CONRICyt, the keywords with the different boolean operators were as follows: intestinal obstruction, children and congenital adhesions. The review period was the past 25 years. No national publication was found.
A case of intestinal obstruction is presented caused by anomalous congenital band, which extended from the terminal ileum to the mesentery.
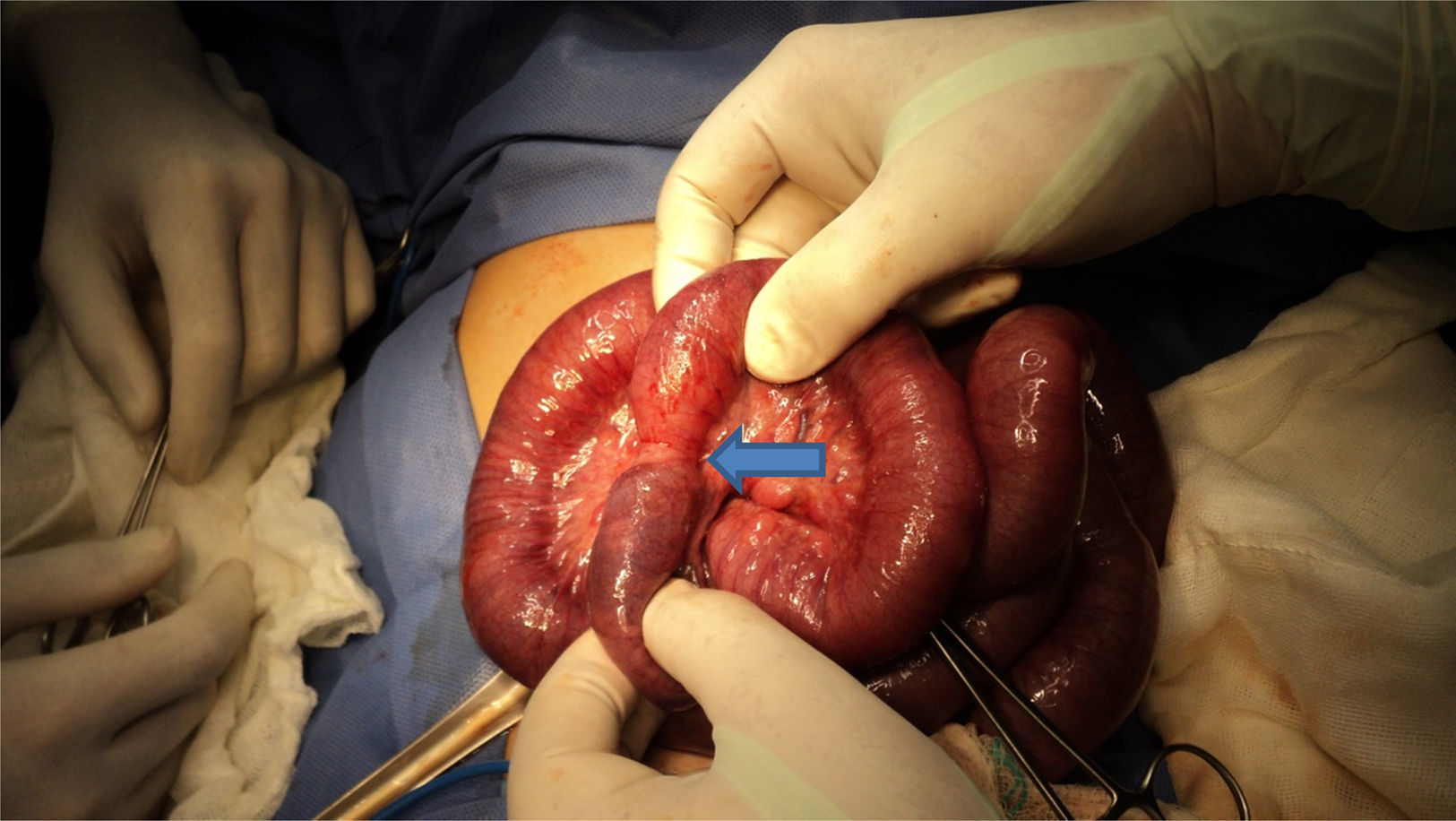
Clinical caseA 1-year-old male, delivered by caesarean section at term, at normal weight and size. The child had no history of previous surgery or trauma. The condition started 3 days prior to admission with frequent vomiting of bile content. He was attended by a private doctor who indicated treatment with analgesics and anti-emetics. Due to persistent vomiting and oral intolerance, he was taken to a health-sector children's hospital where antibiotic, anti-spasmodic and anti-emetic treatment was started, and he was sent home. He came to our hospital since there was no improvement in his condition. He was irritable on physical examination and his vital signs were: heart rate 110 per minute, respirations 28 per minute, temperature 37°C, blood pressure 90/50mm/Hg; his eyes were sunken, oral mucosa dry and capillary refill 4–5s. The patient had a distended abdomen, reduced peristalsis and was tender on palpation in the mesogastrium, with no signs of peritoneal irritation. Rectal examination revealed an empty rectal ampulla. A nasogastric tube was placed which drained gastro-biliary content and parenteral solutions were started. Complete blood count with leukocytes 29.4 (103μL−1), segmental neutrophils 89, bands 1, haemoglobin 14g/dl, haematocrit 42.50%, platelets 529 (103μL−1). Abdominal X-rays showed dilated small bowel loops, air-fluid levels and an absence of gas in the rectal ampulla (Fig. 1). Ultrasound reported dilated bowel loops and the presence of free fluid. An exploratory laparotomy was decided, abundant yellow-citrine fluid was found on opening the cavity and a fibrous band that went from the terminal ileum to the mesentery, compressing the ileum at 50cm from the ileocaecal valve, which showed signs of ischaemia (Fig. 2). The fibrous band was cut and ligated. After resecting the adhesion, circulation to the intestine recovered satisfactorily (Fig. 3). No further pathology was found in the intestine, and therefore the cavity was closed. The patient made satisfactory progress, tolerating oral feeding, and was discharged from hospital 4 days later.



Anomalous congenital band has no relationship with previous abdominal problems, such as laparotomies, inflammatory bowel disease, peritonitis or embryonic remnants, such as the vitelline vessels or omphalomesenteric duct. These bands seem to be congenital in origin5,6 and cause obstruction when the intestine becomes trapped between the band and the mesentery, which can cause an internal hernia.4
In our review of the literature, we found 16 reported cases in children aged from 2 days to 16 years, 14 male and 2 female, and 19 cases in adults between 17 and 76 years of age.1–10
The aetiology of anomalous congenital band is obscure and has no identifiable embryonic cause, since its location is not similar to that of remnants.
The origin at the insertion of the bands found suggests an anomaly of the mesentery rather than of the intestine. At about 28 days of intrauterine life, the ventral and dorsal mesentery divides the peritoneal cavity into two halves, right and left, the ventral mesentery usual disappears except around the liver and in front of the stomach. As the intestine takes its final position, the mesentery remains in the posterior part of the abdomen. The mesentery of the ascending colon fuses with the parietal peritoneum and disappears. The bands between the ascending colon and the terminal ileum found in these patients might be the result of the fusion of part of the mesentery of the ascending colon with the medial structures of the posterior wall of the abdomen. The bands between the mesentery and liver might be remnants from a failure in the reabsorption of the ventral mesentery.5
With regard to their location, anomalous congenital bands can go from the terminal ileum or its mesentery to the ascending colon, ligament of Treitz, right liver lobe and bladder. Most of the reports consulted refer to obstruction in the left side of the abdomen, between 15 and 150cm from the ileocaecal valve with an average of 120 cm2,4,7; others locate it at the level of the colon.2,5
It predominates in males, at ages varying from 2 days to 7 years, with a mean of 2 years,1,2,4–6 although some cases are reported in adults.8–10
The main symptoms reported are: abdominal distension, bile-type vomiting, absence of stools and acute or chronic abdominal pain, with a progression time of 2–5 days.2–5
The most significant sign is leukocytosis and dilation of the loops and air-fluid levels can be seen on X-ray.4,5
Histopathological studies of the bands show connective tissue, vessels and nerves.4,5,11
Management should be surgical as promptly as possible, either by laparotomy or laparoscopy, in order to prevent irreversible ischaemia and to reduce morbidity and mortality.4,9,10,12
Most of the patients studied underwent resection of the adhesion alone, the remainder required intestinal resection and anastomosis or caecostomy due to intestinal necrosis. Mortality occurred in only one child aged 9 days with perforated colon and sepsis secondary to peritonitis. There was no recurrence of the intestinal obstruction.2,4,5
ConclusionsAlthough this entity is rare, the possibility of anomalous congenital band should be taken into account in every child with signs of intestinal occlusion with no history of previous surgery or abdominal trauma.
It is extremely difficult to diagnose intestinal obstruction due to anomalous congenital band and no imaging study is helpful. Only exploratory or laparascopic laparotomy can be used for the diagnosis and treatment of this problem.
Surgical treatment should be as prompt as possible to prevent ischaemia and reduce morbidity and mortality.
According to our literature review, this is the first case of anomalous congenital band as a cause of mechanical intestinal obstruction, in a 1-year-old Mexican child, and operated successfully.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflict of interestsThe authors have no conflicts of interest to declare.
Please cite this article as: Galván-Montaño A, Trejo-Ávila M, García-Moreno S, Pérez González A. Banda congénita anómala una patología rara de obstrucción intestinal en niños. Caso clínico. Cir Cir. 2017;85:164–167.