





The goal of conservative surgical treatment of laryngeal cancer is to obtain oncological control with preservation of laryngeal function. The concept of laryngeal function preservation should be understood as the preservation of the patient's ability to breathe normally with neither tracheostomy nor aspiration, and maintaining intelligible speech. This can be achieved by a balance between two fundamental aspects, proper patient selection (based on tumour extension and preoperative laryngeal function), and an adequate histopathological analysis of the surgical specimen. Supracricoid subtotal laryngectomy is the voice conservative surgical technique that offers the best possibility of control in patients with locally advanced laryngeal cancer. The proper histopathological analysis allows staging and selecting patients for adjuvant therapy, avoiding unnecessary ones as well as designing monitoring and surveillance programs based on risk factors.
ObjectiveTo highlight key points in the histopathological evaluation of the surgical specimen of a subtotal laryngectomy.
ConclusionThe proper communication between the surgeon and pathologist, offering complete information on preoperative clinical evaluation and the knowledge of the key points in the evaluation of the surgical specimen (sites of tumour leakage and surgical resection margins) are fundamental parameters to achieve a proper histopathological evaluation of the surgical specimen.
La finalidad del tratamiento quirúrgico conservador del cáncer laríngeo es obtener control oncológico con preservación de la función laríngea; a su vez, la preservación de la función debe entenderse como la conservación de la capacidad del paciente para ventilar por vía normal sin traqueotomía y sin aspiración, manteniendo habla inteligible. Este propósito se logra manteniendo el balance entre 2 aspectos fundamentales: la adecuada selección del paciente (con base en la extensión tumoral y la función laríngea preoperatoria) y un adecuado análisis histopatológico de la pieza quirúrgica. La laringectomía subtotal supracricoidea es la técnica quirúrgica conservadora de la voz que oncológicamente ofrece la mejor posibilidad de control en pacientes con cáncer localmente avanzado de laringe; su adecuado análisis histopatológico permite estadificar y seleccionar a los pacientes candidatos a tratamiento adyuvante, evitando terapias innecesarias, y permite diseñar un programa de seguimiento y vigilancia con base en los factores de riesgo.
ObjetivoSeñalar los puntos clave en la evaluación histopatológica de la pieza de laringectomía subtotal.
ConclusionesLa adecuada comunicación entre el cirujano y el patólogo, el ofrecer información completa de la evaluación preoperatoria clínica y el conocimiento de los puntos clave en la evaluación de la pieza (sitios de probable fuga tumoral y márgenes de sección quirúrgica) son parámetros fundamentales para lograr la adecuada evaluación histopatológica del espécimen quirúrgico.
Epidermoid cancer is the most frequent tumour to start in the laryngeal epithelium. GLOBOCAN1 reports 151,000 new cases of laryngeal cancer per year worldwide; it ranks 17th among solid tumours, with a prevalence of 1.1% and standard mortality rate by age of 1.2/100,000.
In Mexico, the Dirección General de Epidemiología reported a total of 855 cases of laryngeal cancer in 2008. The rate was 0.8 per 100,000 inhabitants, and represented 0.2% of total deaths and 1.3% of total tumours.2
The major aetiological factor in the development of laryngeal cancer is tobacco use.3,4
The larynx has different embryological origins, and may be divided into 3 regions: supraglottis (above the vocal folds), glottis (vocal folds and anterior commissure) and subglottis (below the vocal folds). The most common site of tumour origin is the glottic region and vocal fold plane, where the tumour starts and spreads mainly to the supraglottic region.5
The aim of treatment for laryngeal cancer is to achieve the right balance between oncologic control, phonation preservation and natural ventilation. Treatment of laryngeal cancer depends on the tumour stage and general patient conditions.
In patients with laryngeal cancer who are indicated for laryngeal function preservation, the functionality of the cricoarytenoid unit is essential. This unit is formed by the arytenoids cartilage, the cricoids cartilage, the posterior and lateral cricoarytenoid muscles, the interarytenoid muscles and the lower and upper laryngeal nerves; preservation of these structures during functional surgery enables physiological success, since it is this unit which governs correct phonation and swallowing without aspiration.5,6
In initial (T1-2) tumours, a single treatment is normally indicated; this may be either endoscopic resection with laser, radical radiotherapy to the voice box or open surgery aimed at voice preservation. However, in local or advanced local and regional tumours, mutilating surgery is the standard treatment, which involves voice box removal and definitive tracheotomy. Patients with “intermediate stage” cancer, i.e. patients with tumours which may be locally advanced but which do not involve any major impairment of phonation or swallowing, where voice is of an acceptable quality and vocal fold and/or adenoid mobility is sufficient, are usually classified as T2 or T3 and a few at T4a stage, and for them the normal treatment is total laryngectomy, followed by radiotherapy or chemo and radiotherapy, depending on diagnosis.
It is for this patient group that supracricoid subtotal laryngectomy with laryngeal reconstruction with cricohyoidoepiglottopexy has been designed. The aim of this treatment is the same as that guiding therapy for laryngeal cancer: to obtain a balance between natural phonation-ventilation and satisfactory cancer control, with a cure rate equal to total laryngectomy followed by radio therapy.6–9
Supracricoid subtotal laryngectomy with laryngeal reconstruction with cricohyoidoepiglottopexy is indicated in patients with advanced tumours but correct laryngeal function, in patients who would otherwise be indicated for total laryngectomy, if treatment were standard. Supracricoid subtotal laryngectomy with laryngeal reconstruction with cricohyoidoepiglottopexy is a step prior to total laryngectomy and a last attempt at laryngeal function preservation.8–10
Suitable patient selection9 is required, as is appropriate assessment of the operative specimen to enables us to ensure complete removal of the tumour and this is the key to reducing the tumour recurrence rate.
The aim of this paper is to expose the major key points for the appropriate histopathological study of the specimen from supracricoid subtotal laryngectomy in patients with laryngeal epidermoid cancer.
Supracricoid subtotal laryngectomyThis procedure was initially reported by Majer and Rieder,11 and popularised by Piquet12 in Lille, France; the technique is currently considered as a safe and functional alternative to total laryngectomy in patients with locally advanced cancer of the larynx (Fig. 1). It is a conservative procedure, designed for patients with tumours which invade the paraglottic space but which preserve ipsilateral arytenoid cartilage; for patients with anterior commissure tumours which penetrate in the submucosa portion of the tumours of the hyoidthyroepiglttic space, and for patients with tumours which invade the bottom of the epiglottis, but which do not spread to its laryngeal side, with no mass invasion of the hyoidthyroepiglttic space or with invasion of the lower third of the epiglottis without suprahyoid invasion.10

This technique is contraindicated in tumours with subglottic infiltration, arytenoid adherence, bilateral foldial adherence, tomographic infiltration of the hyoidthyroepiglttic space, extralaryngeal tumour and major infiltration of the thyroid cartilage.10
The prognosis of patients who undergo supracricoid subtotal laryngectomy depends on histological findings from the surgical specimen. One of the most important factors in prognosis of local recurrence is the staging of surgical resection margins. The presence of tumour infiltration in resection is associated with between 22% and 70% of local recurrence. The presence of dysplasia in surgical resection margins is associated with disease recurrence in a shorter period of time, compared with patients without dysplasia in resection margins.13,14
To identify prognostic factors in the surgical specimen of the supracricoid subtotal laryngectomy the following is required: systematic assessment15 of the real tumour size, of the presence or absence of tumour infiltration to nearby structures, and tumour spread to different anatomical regions of the larynx, mainly the paraglottic region.
The spread of a laryngeal tumour depends on the sub-site of origin; supraglottic tumours therefore invade the preepiglottic area and the supraventricular paraglottic space. Glottic and subglottic tumours invade the infraventricular paraglottic space, from the anterior commissure to the bottom of the epiglottis, its laryngeal side and they spread outwards infiltrating the keel of the thyroid cartilage.
Recommendations for the management of supracricoid subtotal laryngectomy specimensOnce the anatomical structures of the specimen have been recognised, the specimen must be sent for histopathological assessment with suitably appropriate guidance regarding the anatomical structures of the tumour site in an outline or a sketch showing where the tumour started (Fig. 2), the surgical resection margins and information relating to the preoperative laryngeal kinetics (vocal fold and arytenoid mobility).

It is highly important the surgeon's direct communication with the pathologist during the procedure to assess the surgical resection margins transoperatively; the presence of a visible tumour in the surgical sites may alter any decisions regarding the extent of surgery and on occasion abort the conservative procedure, with total laryngectomy being performed instead; this situation would arise if the tumour had spread more extensively than assessed preoperatively.
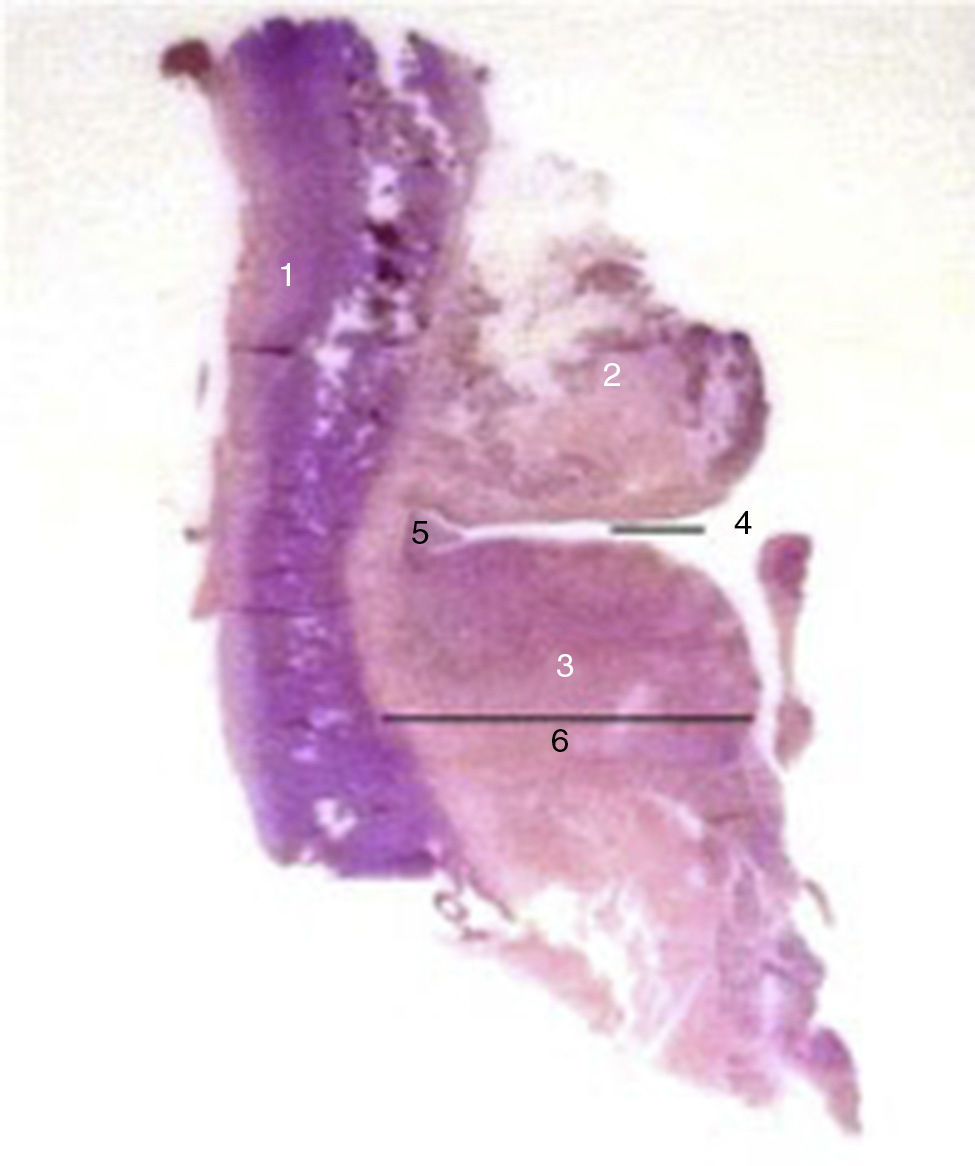
The supracricoid subtotal laryngectomy specimen (Fig. 3) includes: total thyroid cartilage and bilateral paraglottic space, both vocal folds, both Morgagni ventricles, both ventricular bands, the anterior commissure, the bottom of the epiglottis section along its limit with the upper edge of the thyroid cartilage (suprathyroid portion), and may or may not include the arytenoid cartilage of the same side as the fold with tumour growth.
 Anterior view. (B) Posterior view. 1: Posterior wall of thyroid cartilage; 2: Ventricle band; 3: Vocal fold; 4: Morgagni ventricle; 5: Anterior commissure; 6: Paraglottic area.")
The surgical edges are identified and dyed with different colours. The upper margin corresponds to the mucous membrane of the bottom of the epiglottis, the bottom of the mucous membrane covering the upper edge of the cricoids cartilage along its margin with the thyroid cartilage (cricoidthyroid membrane) and the back of the posterior segment of the vocal fold in the cricoids-vocal ligament, occasionally including the ipsilateral arytenoids cartilage.
Fresh tumour measurements must be made and the distance from surgical edges and its location must be identified, including both longitudinal and horizontal extension. The specimen is formalin-fixed at 10% for 24h. 3mm thick sagittal slices are made and photographed to compare with histological cross-sections; if the thyroid cartilage is calcified, the cuts may be made with a hacksaw or plain scissors and decalcified for 24h. A parallel cut along the posterior edge of approximately 3–4mm is made, which is then cut lengthwise to increase the surface area to be assessed.
The sagittal slices taken enable assessment of the upper and lower surgical margins, the band and vocal fold, the ventricle, the paraglottic space and the thyroid cartilage; the central slice shows the anterior commissure, and the most posterior slice shows the posterior third of the vocal fold (fold-arytenoid region) or the arytenoid cartilage. Each slice enables an assessment to be made as to whether the tumour has infiltrated those structures.
All sagittal slices must be included in histopathological study (Fig. 4). Examination of the specimen under the microscope must determine the histological type of malignancy, the level of differentiation, maximum thickness, infiltration to paraglottic space, infiltration to anterior commissure and thyroid cartilage, vascular invasion, perineural invasion, the presence of dysplasia or in situ carcinoma in adjacent mucosa, and lastly surgical margin status. There is positive margin outcome if the tumour cells are in contact with the surgical margin dye.16

The histopathological report of the supracricoid subtotal laryngectomy specimen must include: (1) specimen sent and type of procedure performed; (2) location of malignant tumour (anatomical sites infiltrated by the tumour); (3) histological type; (4) histological degree; (5) tumour size; (6) tumour thickness (vertical growth towards paraglottic space measured in millimetres from the basement membrane of the epithelium lining); (7) tumour spread; (8) infiltration or non infiltration of anterior commissure; (9) infiltration or non infiltration of the thyroid cartilage; (10) vascular invasion; (11) perineural invasion; (12) presence or absence of in situ dysplasia in adjacent mucosa membrane; (13) surgical margin status.17,18
The sites where infiltrated resection margins are most frequently infiltrated by tumours are: the junction of the vocal fold with the arytenoid mucosa membrane (posterior slice site) or the arytenoids themselves if they were included in surgery; tumour presence here involves tumour spread into the interarytenoid area and there is great risk of residual tumour in the remaining arytenoids; the mucosa membrane located below the anterior commissure; the lower surgical margin site, where the glottis connects with the subglottis and the mucous membrane below the vocal folds, which would involve subglottic tumour infiltration.16–18
ConclusionsSupracricoid subtotal laryngectomy is a therapeutic alternative in patients with locally advanced epidermoid cancer of the larynx where laryngeal function is satisfactory. Patient selection for this technique is based on 3 criteria: identification of the anatomical laryngeal sites invaded by the tumour, assessment of laryngeal function prior to surgical intervention and histopathological study of the surgical specimen.
Specimen analysis requires constant communication between the surgeon and the pathologist, so that the highest possible information relating to tumour status, laryngeal kinetics and determinable resection margins is maintained; correct pathological staging of the tumour depends on this and from here we are able to design a follow-up programme or possible adjuvant therapy.
Inappropriate pathological assessment may lead to the need for unnecessary surgical re-intervention for the patient, with excessive excisional consequences, or unnecessary postoperative radiotherapy with further damage to laryngeal function.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: García-Sánchez M, Romero-Durán E, Mantilla-Morales A, Gallegos-Hernández JF. Evaluación histopatológica del espécimende laringectomía subtotal. Cir Cir. 2015;83:537–542.