




In patients diagnosed with anal fistula, knowing the quality of life specifically related to the disease can help coloproctology specialists to choose the most appropriate therapeutic strategy for each case. The aim of our study is to analyze and describe the factors related to the specific quality of life in a consecutive series of patients diagnosed with anal fistula.
MethodsObservational, cross-sectional study carried out from March 2015 to February 2017. All patients were assessed in the colorectal surgery unit of a hospital in southeast of Spain. After performing an initial anamnesis and a physical examination, patients diagnosed with anal fistula completed the Quality of Life in patients with Anal Fistula Questionnaire (QoLAF-Q). This questionnaire specifically measures quality of life in people with anal fistula and its score range is the following: zero impact=14 points, limited impact=15 to 28 points, moderate impact=29 to 42 points, high impact=43 to 56 points, and very high impact=57 to 70 points.
ResultsA total of 80 patients were included. The median score obtained in the questionnaire for the sample studied was 34.00 (range=14–68). Statistically significant differences between patients with “primary anal fistula” (n=65) and “recurrent anal fistula” (n=15) were observed (mean rank=42.96 vs mean rank=29.83, P=.048). Furthermore, an inverse proportion (P=.016) between “time with clinical symptoms” and “impact on quality of life” was found (<6 months: mean rank=45.55; 6–12 months: mean rank=44.39; 1–2 years: mean rank=37.83; 2–5 years: mean rank=22; >5 years: mean rank=19.00). There were no statistically significant differences (P=.149) between quality of life amongst patients diagnosed with complex (mean rank=36.13) and simple fistulae (mean rank=43.59).
ConclusionsAnal fistulae exert moderate-high impact on patients’ quality of life. “Shorter time experiencing clinical symptoms” and the “presence of primary fistula” are factors that can be associated with worse quality of life.
En pacientes diagnosticados de fístula anal, conocer la calidad de vida específicamente relacionada con la misma puede ayudar a los especialistas en coloproctología a elegir la estrategia terapéutica más adecuada para cada caso. El objetivo de nuestro estudio es analizar y describir los factores relacionados con la calidad de vida específica en una serie consecutiva de pacientes diagnosticados de fístula anal.
MétodosEstudio observacional transversal realizado entre marzo del 2015 y febrero del 2017 con pacientes diagnosticados de fístula anal. Tras la anamnesis y la exploración inicial, los pacientes completaron el Quality of Life in patients with Anal Fistula Questionnaire. Este cuestionario mide específicamente la calidad de vida en personas con fístula anal. Su rango de valores es: 14 puntos = impacto nulo; 15-28 puntos = impacto limitado, 29-42 puntos = impacto moderado, 43-56 puntos = impacto alto, y 57-70 puntos = impacto muy alto.
ResultadosSe incluyó a un total de 80 pacientes. La puntuación mediana obtenida en el cuestionario por la muestra estudiada es de 34.00 (rango = 14-68). Se observaron diferencias estadísticamente significativas entre pacientes con «fístula primaria» y «fístula recurrente» (rango medio = 42,96 vs rango medio = 29,83; p = 0,048). Se establece una relación inversamente proporcional (p = 0,016) entre el tiempo con síntomas clínicos y la afectación de la calidad de vida en los pacientes (< 6 meses: rango medio = 45,55; 6-12 meses: rango medio = 44,39; 1-2 años: rango medio = 37,83; 2-5 años: rango medio = 22; > 5 años: rango medio = 19,00). No se encontraron diferencias estadísticamente significativas (p = 0,149) en la calidad de vida entre pacientes con fístulas complejas (rango medio = 36,13) o simples (rango medio = 43,59).
ConclusionesLos pacientes con fístula anal presentan una afectación de moderada a alta en su calidad de vida. Un menor tiempo con síntomas clínicos y la presencia de fístula primaria son factores asociados a peor calidad de vida.
An anal fistula is an abnormal tract or cavity that communicates the perineal skin with the anal canal or rectum through an identifiable internal orifice.1,2 The majority appear as a result of cryptoglandular infection.3 The literature shows a wide range in the incidence of anal fistula (3.4: 100,000 inhabitants in Spain,4 8.6: 100,000 inhabitants5 in northern Europe), representing 10%–30% of coloproctology procedures and more frequent in adults aged 30–60.6 The symptoms are usually preceded by drainage of a perianal abscess and include, mainly, suppuration, bleeding and anal pain.6–8
According to the Standards Committee for the American Society of Colon and Rectal Surgeons, following the classification by Parks et al.,3simple fistulae are low intersphincteric or transsphincteric fistulae that include less than 30% of the external sphincter.9 Meanwhile, complex fistulae include: transsphincteric lesions with more muscle mass, suprasphincteric fistulae, anterior fistulae in women, recurrent fistulae, and fistulae associated with preexisting anal incontinence, inflammatory bowel disease or radiation.9 This classification helps choose the most appropriate surgical technique, establish an individualized treatment prognosis and perform a comparative evaluation between results reported in the series of the literature.
Fistulotomy is the ideal treatment for simple fistulae,9 with a cure rate greater than 90%.10 Complex fistulae can be treated with different techniques; however, while the intention is to preserve continence, results are controversial.11–16 For this reason, in patients in whom it is not easy to find a definitive surgical solution, the choice of therapeutic strategy should be aimed at improving quality of life.17
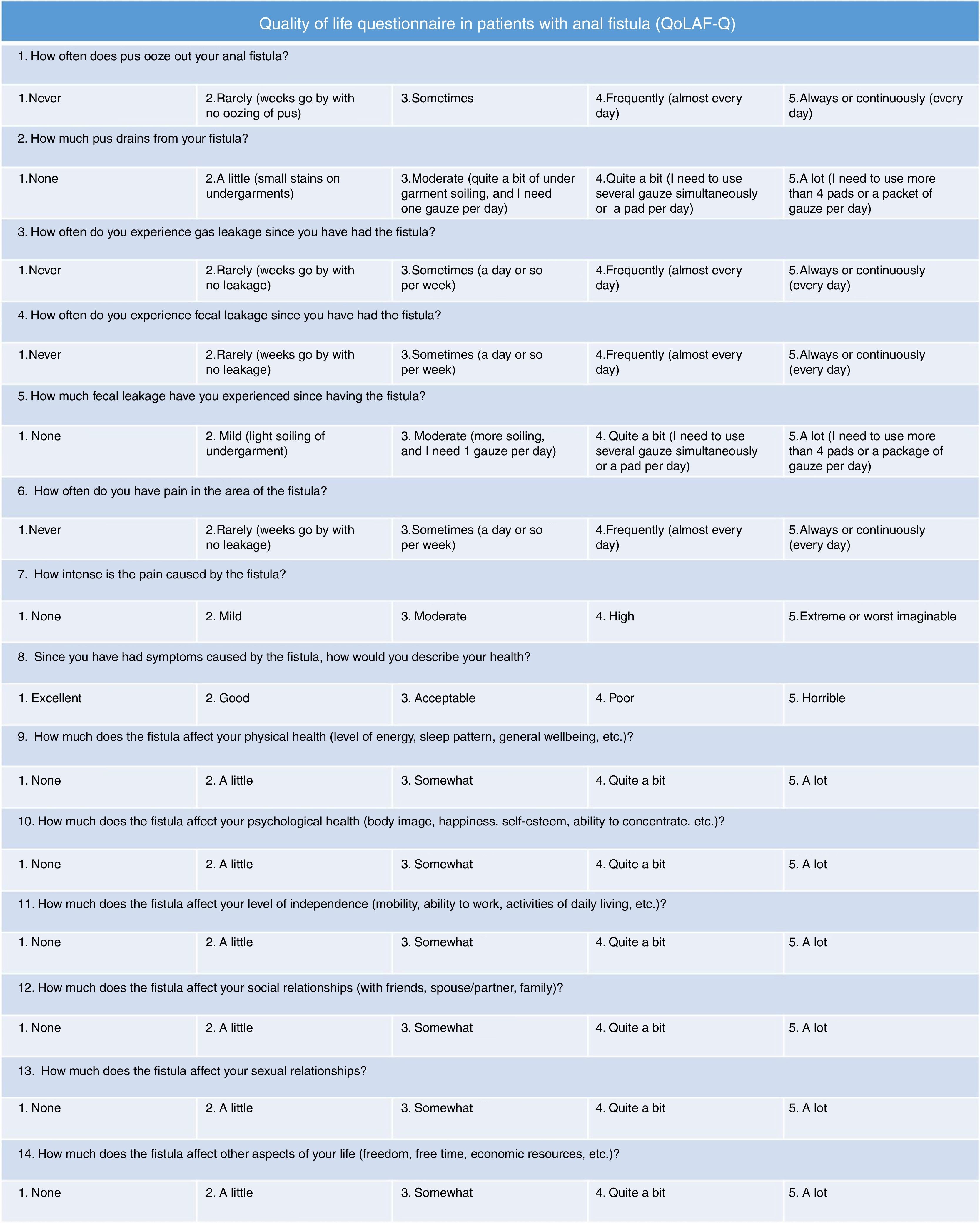
To date, published studies measuring quality of life in patients with perianal fistula use general questionnaires (SF-12, SF-36)17–20 or incontinence-related scores (St Mark's Incontinence Score17,19 Wexner Score,21 FIQL,21 Cleveland Incontinence Score22). Recently, a questionnaire has been published to specifically measure the quality of life of patients diagnosed with perianal fistula (Quality of Life in patients with Anal Fistula Questionnaire [QoLAF-Q])23 (Fig. 1). Therefore, the aim of our study is to describe the specific quality of life in a consecutive series of patients diagnosed with perianal fistula and to analyze which factors are related with a poorer quality of life in this type of patients.
MethodsStudy Design, Participants and Sample Size.")
A cross-sectional observational study was conducted between March 2015 and February 2017. Inclusion criteria were: age over 18, diagnosis of anal fistula (clinically for simple fistulae, or using endoanal ultrasound in uncertain cases or complex fistulae) and sign an informed consent. The exclusion criteria were: cognitive alterations that prevented completing the questionnaire, and diagnosis of inflammatory bowel disease (IBD).
In the calculation of the sample size, quality of life was defined as the main variable (measured with the QoLAF-Q) and the expected change in said variable (the interval range between QoLAF-Q categories) was set at 7 points. In addition, a confidence level of 80% and a margin of error of 5% were accepted. Based on all these criteria, the necessary sample size calculated for this study was 66 subjects. After adding an extra 20% to compensate for possible losses, the final sample size was 80 subjects.
Ethical ConsiderationsThe project was approved by the hospital Ethics Committee (ESVIFISPE). Patients who met the inclusion criteria were invited to participate and received a document with information about their rights, study objectives and research plan. All the documents collected were managed in accordance with European data protection legislation.
Data Collection ProtocolThe patients came to the consultation after referral from the Emergency Department or Primary Care. They received information about the study and gave their informed consent. Next, a detailed medical history was taken and patients were examined thoroughly. Endoanal ultrasound was order when the clinical examination did not yield conclusive data (pain or difficult clinical assessment) or when it indicated the presence of a complex fistula. During the interview, patients completed the QoLAF-Q questionnaire and the Wexner test (in case of incontinence). A surgeon and a resident of the Colorectal Surgery Unit administered the test and resolved any questions the patient might have.
Variables and InstrumentsThe variables studied were: sex, age, obstetric history and previous perianal surgeries, symptoms and time with clinical symptoms, presence of seton, fistula characteristics (classification, number and location of the EO and IO, palpable tract), manometry study and Wexner and QoLAF-Q questionnaires. The Parks et al. classification3 was used to define the fistulae. Fistulae that could not be classified optimally and with guarantees (due to pain during the examination or technical problems) were classified as indeterminate. Recurrent fistulae were those that had been treated for their solution on one or more occasions (not including the drainage of perianal abscesses with the placement of a seton).
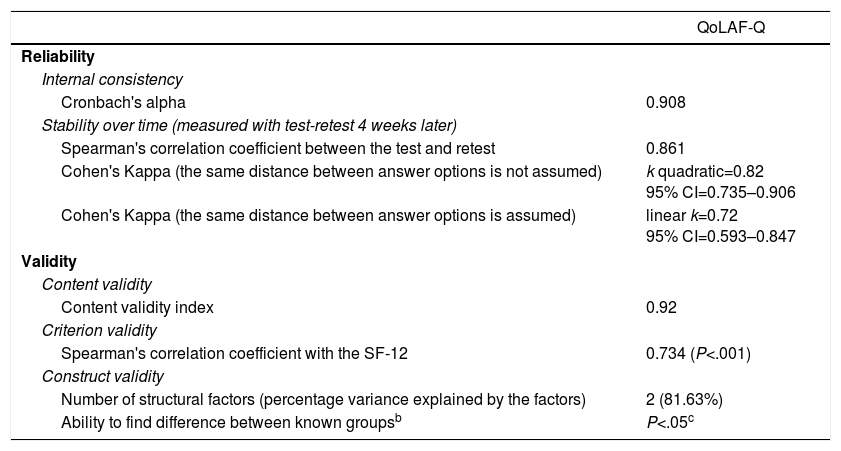
The QoLAF-Q was used to measure the quality of life of patients diagnosed with anal fistula.23 The QoLAF-Q consists of 14 questions with different response options following 5-point Likert scale. Its range of values is: 14 points=zero impact; 15–28 points=limited impact; 29–42 points=moderate impact; 43–56 points=high impact, and 57–70 points=very high impact. The QoLAF-Q was developed following a rigorous methodological protocol. First, the researchers created an initial version of the questionnaire in accordance with WHO guidelines.23 Second, the researchers sent this version of the questionnaire to experts in order to assess the relevance of the items included. Third, the researchers applied the changes indicated by the experts and eliminated items that were not considered pertinent to measure quality of life in patients diagnosed with anal fistula. Finally, the QoLAF-Q was administered to a sample of patients with anal fistula, meticulously evaluating all psychometric properties23 (Table 1). The final version of the QoLAF-Q has 2 dimensions: (1) “physical impact” of the anal fistula; and (2) “psychosocial impact” of the anal fistula. While the first dimension measures the intensity and frequency of clinical symptoms associated with the fistula, the second measures how the fistula affects the psychosocial health of the patient.
Psychometric Properties of the QoLAF-Q Questionnaire.a
| QoLAF-Q | |
|---|---|
| Reliability | |
| Internal consistency | |
| Cronbach's alpha | 0.908 |
| Stability over time (measured with test-retest 4 weeks later) | |
| Spearman's correlation coefficient between the test and retest | 0.861 |
| Cohen's Kappa (the same distance between answer options is not assumed) | k quadratic=0.82 95% CI=0.735–0.906 |
| Cohen's Kappa (the same distance between answer options is assumed) | linear k=0.72 95% CI=0.593–0.847 |
| Validity | |
| Content validity | |
| Content validity index | 0.92 |
| Criterion validity | |
| Spearman's correlation coefficient with the SF-12 | 0.734 (P<.001) |
| Construct validity | |
| Number of structural factors (percentage variance explained by the factors) | 2 (81.63%) |
| Ability to find difference between known groupsb | P<.05c |
The data were analyzed with the SPSS v.22.0 program. The nominal qualitative variables were analyzed through the study of frequencies and percentages. The quantitative variables (ordinal and interval) were analyzed through the study of measures of central tendency and dispersion (mean, standard deviation [SD], median and range). Before making comparisons between groups, the distribution of data was analyzed for all variables. Normal probability plots (histograms, Q-Q plots) and the Shapiro–Wilk test demonstrated that none of the variables followed normal distribution. Therefore, the Mann–Whitney U test was used to compare the medians of 2 independent groups and the Kruskal–Wallis test was used to make comparisons between the medians of more than 2 independent groups. The differences between groups whose value was P<.05 were considered significant.
ResultsDescription of the Sample80 individuals were included in the analysis (3 were excluded due to IBD). The QoLAF-Q was completed by 58 men and 22 women with a mean age of 46.5 (range=18–78 years; SD=11.8). 12.5% presented diabetes, 163% hypertension and 6.2% (5 women) presented a history of vaginal births with no obstetric injuries. Most of the sample (73.7%) had had some type of previous anal surgery (16.4% on 3 or more occasions), the most frequent being perianal abscess drainage (52.5%).
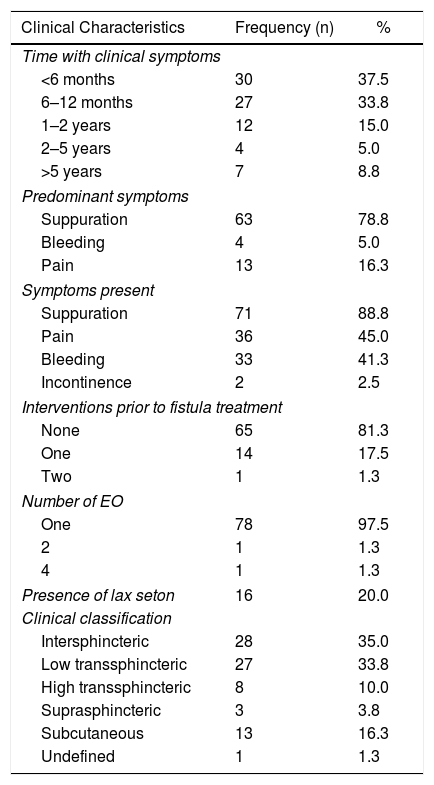
The main clinical characteristics of the fistulae are presented in Table 2. Time with clinical symptoms was less than 12 months in 71.3% of patients, and the predominant clinical manifestation was suppuration (78.8%), followed by pain (16.3%). Two patients in the sample (2.5%) presented mild incontinence symptoms (scores of 2 and 5 on the Wexner scale, respectively, and normal manometry). 97.5% had a single fistula orifice and 20% presented drainage seton placement. Among the patients with recurrent fistulae (n=15), the surgeries previously performed were: 4 fistulotomy, 7 partial fistulectomy plus seton placement, 2 ligations of intersphincteric fistula tract (LIFT), one advancement flap and one infiltration of platelet growth factors.
Clinical Characteristics of the Fistulae.
| Clinical Characteristics | Frequency (n) | % |
|---|---|---|
| Time with clinical symptoms | ||
| <6 months | 30 | 37.5 |
| 6–12 months | 27 | 33.8 |
| 1–2 years | 12 | 15.0 |
| 2–5 years | 4 | 5.0 |
| >5 years | 7 | 8.8 |
| Predominant symptoms | ||
| Suppuration | 63 | 78.8 |
| Bleeding | 4 | 5.0 |
| Pain | 13 | 16.3 |
| Symptoms present | ||
| Suppuration | 71 | 88.8 |
| Pain | 36 | 45.0 |
| Bleeding | 33 | 41.3 |
| Incontinence | 2 | 2.5 |
| Interventions prior to fistula treatment | ||
| None | 65 | 81.3 |
| One | 14 | 17.5 |
| Two | 1 | 1.3 |
| Number of EO | ||
| One | 78 | 97.5 |
| 2 | 1 | 1.3 |
| 4 | 1 | 1.3 |
| Presence of lax seton | 16 | 20.0 |
| Clinical classification | ||
| Intersphincteric | 28 | 35.0 |
| Low transsphincteric | 27 | 33.8 |
| High transsphincteric | 8 | 10.0 |
| Suprasphincteric | 3 | 3.8 |
| Subcutaneous | 13 | 16.3 |
| Undefined | 1 | 1.3 |
The types of fistula present in the study were: 16.3% subcutaneous fistulae (n=13), 35.0% intersphincteric fistulae (n=28), 43.8% transsphincteric fistulae (n=35), 3.8% suprasphincteric fistulae (n=3) and 1.3% undefined fistulae (n=1). In other words, 51.25% of the fistulae presented by the sample were simple (n=41), and 47.5% were complex.
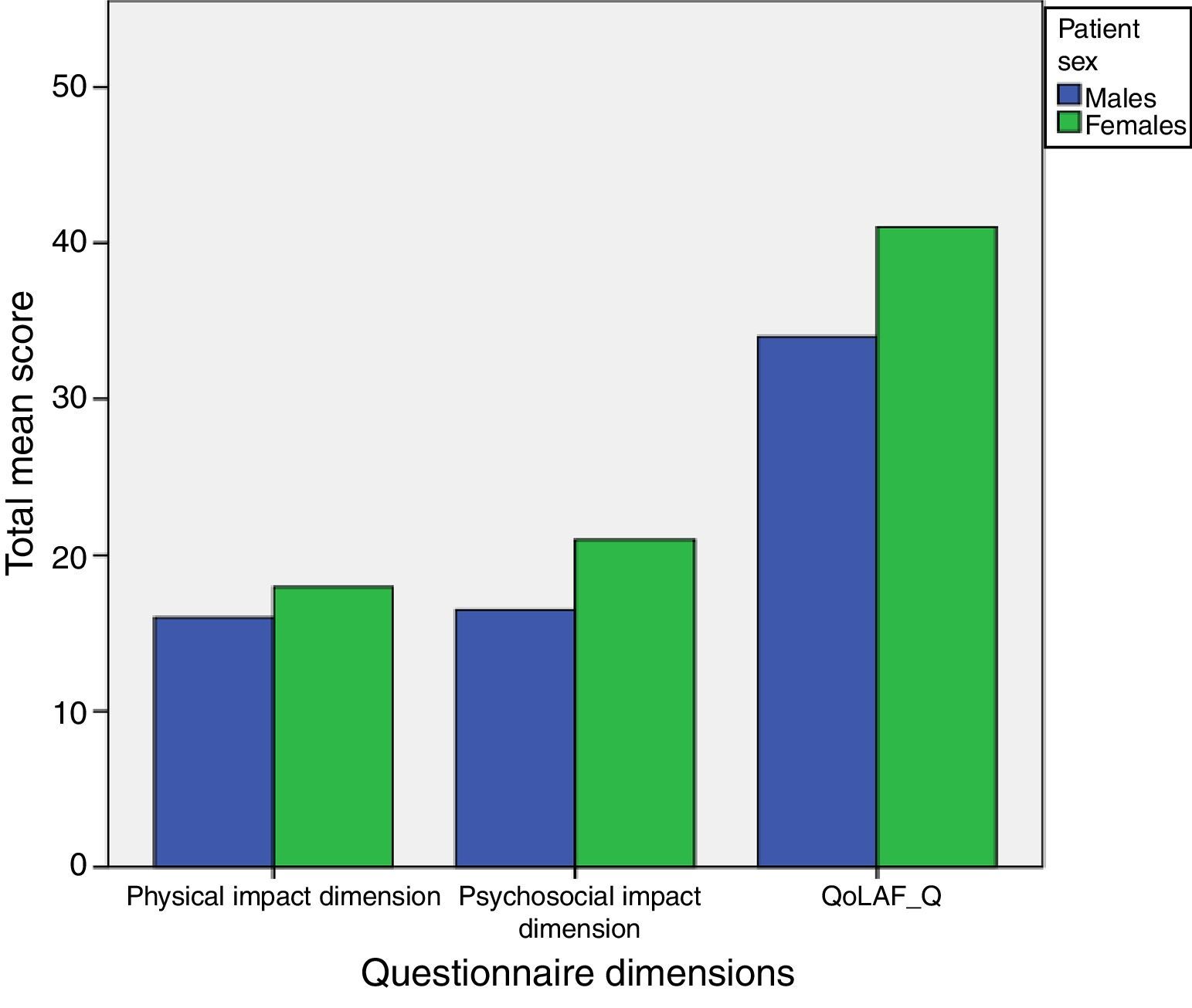
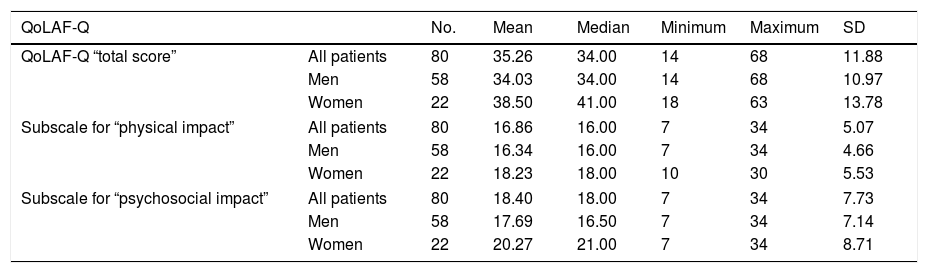
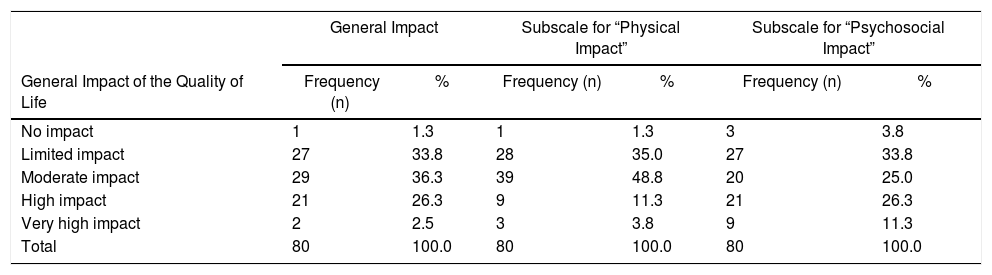
Factors Related With Anal Fistulae and Their Impact on Patient Quality of LifeThe scores of the participants in the QoLAF-Q can be seen in Table 3, and the differences between the medians of men and women are in Fig. 2 (men=34.00, range=14–68; women=41.00, range=18–63). In general, 1.3% said their quality of life was not affected, 33.8% had limited impact, 36.3% moderate impact, 26.3% high impact and 2.5% very high impact (Table 4). Statistically significant differences were observed in quality of life (P=.048) between patients with primary fistula (n=65, range mean=42.96) and recurrent fistula (n=15, range mean=29.83). The physical impact of the fistula was significantly greater in patients with primary fistula (range mean=43.18 vs range mean=28.90, P=.032).
Score of the QoLAF-Q questionnaire (total and by subscales).
| QoLAF-Q | No. | Mean | Median | Minimum | Maximum | SD | |
|---|---|---|---|---|---|---|---|
| QoLAF-Q “total score” | All patients | 80 | 35.26 | 34.00 | 14 | 68 | 11.88 |
| Men | 58 | 34.03 | 34.00 | 14 | 68 | 10.97 | |
| Women | 22 | 38.50 | 41.00 | 18 | 63 | 13.78 | |
| Subscale for “physical impact” | All patients | 80 | 16.86 | 16.00 | 7 | 34 | 5.07 |
| Men | 58 | 16.34 | 16.00 | 7 | 34 | 4.66 | |
| Women | 22 | 18.23 | 18.00 | 10 | 30 | 5.53 | |
| Subscale for “psychosocial impact” | All patients | 80 | 18.40 | 18.00 | 7 | 34 | 7.73 |
| Men | 58 | 17.69 | 16.50 | 7 | 34 | 7.14 | |
| Women | 22 | 20.27 | 21.00 | 7 | 34 | 8.71 | |

Impact of Quality of Life in the Population.
| General Impact | Subscale for “Physical Impact” | Subscale for “Psychosocial Impact” | ||||
|---|---|---|---|---|---|---|
| General Impact of the Quality of Life | Frequency (n) | % | Frequency (n) | % | Frequency (n) | % |
| No impact | 1 | 1.3 | 1 | 1.3 | 3 | 3.8 |
| Limited impact | 27 | 33.8 | 28 | 35.0 | 27 | 33.8 |
| Moderate impact | 29 | 36.3 | 39 | 48.8 | 20 | 25.0 |
| High impact | 21 | 26.3 | 9 | 11.3 | 21 | 26.3 |
| Very high impact | 2 | 2.5 | 3 | 3.8 | 9 | 11.3 |
| Total | 80 | 100.0 | 80 | 100.0 | 80 | 100.0 |
An inversely proportional relationship (P=.016) was found between “time with clinical symptoms” and “effect on quality of life”. The patients who had lived longer with clinical fistula symptoms reported better quality of life (<6 months [n=30]: median range=45.55; 6–12 months [n=27]: median range=44.39; 1–2 years [n=12]: median range=37.83; 2–5 years [n=4]: median range=22; >5 years [n=7]: median range=19.00). However, when comparing quality of life in patients without seton (n=16) versus with seton (n=64), non-significant differences were observed (median range=41.72 vs median range=35.63; P=.322). However, significant differences were found (P=.044) in pain intensity between patients with (median range=30.50) versus without seton (median range=43.00).
When analyzing quality of life according to predominant symptoms, no statistically significant differences were found despite the fact that the patients whose main symptom was suppuration (n=63) presented lower values than the patients whose main symptom was bleeding (n=4) or pain (n=13) (median ranges of 38.87, 61.75 and 41.85, respectively; P=.127).
No statistically significant differences were found for fistula type: complex fistulae (n=38) presented lower values (median range=36.13), while simple fistulae (n=41) presented higher values (median range=43.59, P=.149). When assessed for the presence of one or more EO, no significant differences were observed (P=.496) between patients with one EO (n=78; mean=40.20) and those with 2 or more (n=2; mean=52.25). In addition, no significant differences (P=.478) were found in the quality of life of continent patients (n=78, mean=52.75) versus incontinent patients (n=2, mean=40.19).
DiscussionWe present the first study conducted with the QoLAF-Q.23 The main results show a moderate to high effect on the quality of life of patients diagnosed with anal fistula.
The only curative treatment for anal fistula is surgery. It is intended to eliminate the fistula, relieve symptoms, prevent recurrence and preserve sphincter function.10 Fistulotomy is considered the best treatment for simple fistulae.9,10 On the other hand, complex fistulae are treated with “sphincter-sparing techniques”13,24–30 that attempt to find a compromise between resolution and the risk of incontinence. These techniques do not reach the desired cure rates and aggressive surgical treatment can have a negative impact on the quality of life of patients. Thus, it is essential to define the quality of life of patients with anal fistula before choosing a treatment,31 and therefore the QoLAF-Q23 was used.
In this study, we found that the anal fistula exerts a moderate to high impact on the quality of life of the participants (higher in women than in men). These results are comparable with those by Owen et al.,17 which show a reduction in the quality of life compared to the population without anal fistula. However, Sailer et al.32 indicate that anal fistula is relatively well tolerated, which is corroborated by the fact that patients with a “time with clinical symptoms” of less than 6 months have a worse quality of life than those who have had these symptoms longer. This could be due to the existence of a mechanism of adaptation to the anal fistula as a chronic disease, which should be considered before starting intensive treatment as time seems to play in favor of the patient. Furthermore, it was observed that primary fistulae are associated with poorer quality of life, which suggests that patients with recurrent fistulae (longer time with symptoms) are more adapted to this situation. Nevertheless, these results are far from those presented by Owen et al.,17 where patients with recurrent fistula presented a poorer quality of life in physical function and emotional role.
The use of drainage setons is defended as a treatment and first step for definitive surgery as it facilitates drainage, decreases infection and facilitates fibrotic reaction.19,33–35 In this regard, Kelly et al.35 have reported good tolerance in 96% of their patients. Other authors19 defend that the type of lax seton is fundamental to improve quality of life and show how the use of “knot-free Comfort Drain” significantly improves quality of life in physical and mental health scores compared to the use of conventional lax seton. According to the visual analog scale used, patients with Comfort Drains experienced greater comfort, well-being, and less burning sensation and pruritus. Coinciding with other studies,17 our patients with drainage seton did not present significant differences in quality of life when compared with patients without seton, but they did report lower pain intensity.
Incontinence has a negative effect on continence in quality of life32,36,37 and the treatment of complex fistulae can make it worse.21,22 According to our results, patients with fistula associated with altered continence do not have a poorer quality of life than the rest, although the number of patients with incontinence was too small to obtain solid conclusions. The importance that patients give to the possibility of presenting incontinence after perianal fistula treatment is reflected in the Ellis study,38 which concludes that most patients select sphincter-sparing techniques, even though they present worse results.
The main limitation of the study is the relatively small sample size that, consequently, does not allow us to draw generalizable conclusions. However, the article presents for the first time a quality of life study in patients with anal fistula, using a score that was designed specifically for this type of patients. In future studies, this will allow us to assess the effect of different treatments on patients’ quality of life, which is essential for us to consider when guaranteeing the success or failure of a new therapeutic option. As conclusions, anal fistulae have a moderate to high effect on patients’ quality of life. The duration of clinical symptoms, as well as the presence of primary fistula, are factors that are associated with worse values in QoLAF-Q. In any event, larger future studies with more patients are necessary in order to observe greater correlations between different parameters associated with anal fistula.
Conflict of InterestsThe authors have no conflict of interests to declare.
Please cite this article as: Ferrer-Márquez M, Espínola-Cortés N, Reina-Duarte Á, Granero-Molina J, Fernández-Sola C, Hernández-Padilla JM. Análisis y descripción de la calidad de vida específica en pacientes con fístula anal. Cir Esp. 2018;96:213–220.
