




Complications after ileocecal resection for Crohn's disease (CD) are frequent. The aim of this study was to analyze risk factors for postoperative complications after these procedures.
Materials and methodsWe conducted a retrospective analysis of patients treated surgically for Crohn's disease limited to the ileocecal region during an 8-year period at 10 medical centers specialized in inflammatory bowel disease (IBD) in Latin America. Patients were allocated into 2 groups: those who presented major postoperative complications (Clavien-Dindo>II), the “postoperative complication” (POC) group; and those who did not, the “no postoperative complication” (NPOC) group. Preoperative characteristics and intraoperative variables were analyzed to identify possible factors for POC.
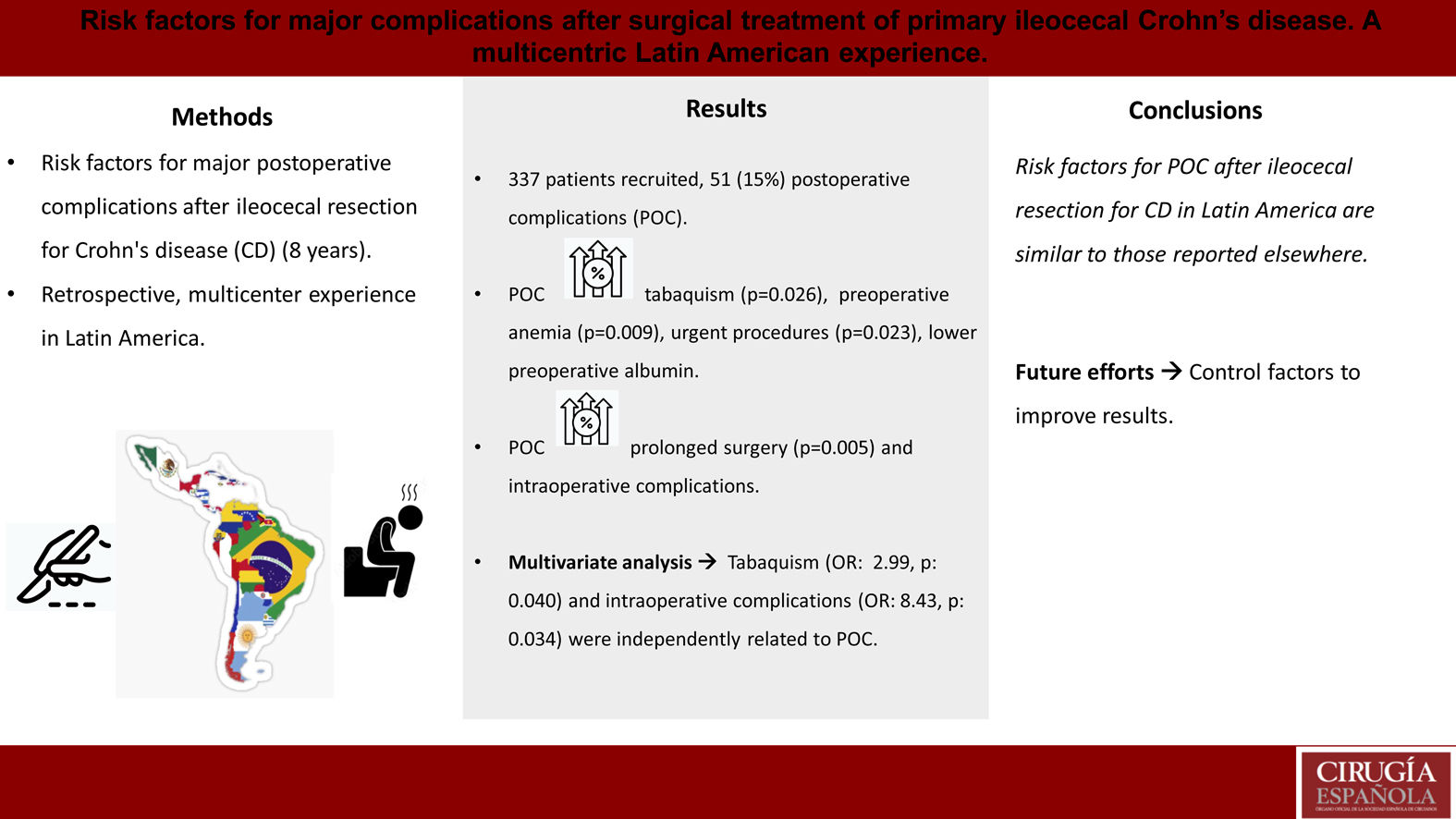
ResultsIn total, 337 patients were included, with 51 (15.13%) in the POC cohort. Smoking was more prevalent among the POC patients (31.37 vs 17.83; p=0.026), who presented more preoperative anemia (33.33 vs 17.48%; p=0.009), required more urgent care (37.25 vs 22.38; p=0.023), and had lower albumin levels. Complicated disease was associated with higher postoperative morbidity. POC patients had a longer operative time (188.77 vs 143.86min; p=0.005), more intraoperative complications (17.65 vs 4.55%; p<0.001), and lower rates of primary anastomosis. In the multivariate analysis, both smoking and intraoperative complications were independently associated with the occurrence of major postoperative complications.
ConclusionThis study shows that risk factors for complications after primary ileocecal resections for Crohn's disease in Latin America are similar to those reported elsewhere. Future efforts in the region should be aimed at improving these outcomes by controlling some of the identified factors.
Las complicaciones posteriores a resección ileocecal por enfermedad de Crohn (EC) son frecuentes. El objetivo de este estudio fue analizar los factores de riesgo para presentar complicaciones postoperatorias después de estos procedimientos.
Materiales y métodosSe realizó un análisis retrospectivo de los pacientes operados por EC limitada a la región ileocecal durante un período de 8 años en 10 centros especializados en enfermedad inflamatoria intestinal (EII) de América Latina. Los pacientes fueron divididos en 2 grupos, los que presentaron complicaciones postoperatorias mayores (Clavien-Dindo>II) (denominado grupo de complicaciones postoperatorias [POC]) y los que no (grupo sin complicaciones postoperatorias [NPOC]). Se analizaron las características preoperatorias y las variables intraoperatorias para identificar posibles factores relacionados con las POC.
ResultadosSe incluyeron 337 pacientes, 51 (15,13%) en el grupo con POC. El grupo POC presentó mayor índice de tabaquismo (31,37 vs. 17,83; p=0,026), quienes presentaron más anemia preoperatoria (33,33 vs. 17,48%; p=0,009), urgencias (37,25 vs. 22,38; p=0,023) y menores niveles de albúmina. Los procedimientos por enfermedad complicada se asociaron con una mayor morbilidad postoperatoria. Los pacientes con POC tuvieron un tiempo operatorio más largo (188,77 vs. 143,86min; p=0,005), más complicaciones intraoperatorias (17,65 vs. 4,55%; p<0,001) y menores tasas de anastomosis primaria. En el análisis multivariado, tanto tabaquismo como complicaciones intraoperatorias se asociaron de forma independiente con la aparición de complicaciones mayores postoperatorias.
ConclusiónEste estudio demuestra que los factores de riesgo de complicaciones posteriores a resecciones ileocecales primarias por EC en América Latina son similares a los reportados en otros lugares. Los esfuerzos futuros en la región deben estar dirigidos a mejorar estos resultados mediante el control de algunos de los factores identificados.
Crohn's disease (CD) is a chronic condition associated with transmural inflammation, which commonly affects the ileocaecal region.1 In these patients, repeated flares of the disease are associated with complications (fibrotic stenosis or fistulas), and despite significant advances in medical therapy, surgery is still needed in a significant proportion of patients.2
In Latin America, as in other parts of the world, the prevalence of Crohn's disease is rising, with some of the highest numbers reported in Brazil and Argentina, of approximately 24 and 15 patients/100,000 persons.3
Ileocaecal resections for complicated disease are associated with higher rates of postoperative complications, when compared to luminal disease.4,5 For this reason, different studies aimed to identify risk factors associated with higher postoperative morbidity.6
Data related to the surgical management of inflammatory bowel disease (IBD) in Latin America is scarce. Information about indications and outcomes of ileocaecal resections for CD, use of minimally invasive approach and types of anastomosis, as examples, are lacking.7
The aim of this study was to identify possible risk factors associated with postoperative complications in a large cohort of patients submitted to primary ileocaecal resections due to CD in different countries in Latin America.
Materials and methodsEthical considerationsThis study was approved by institutional review boards from all included centers, according to good clinical practice standards.
Study design and settingThis is a retrospective multicentric study. Consecutive patients primarily operated for CD, limited to the ileocaecal region, from ten IBD specialized, academic centers of 4 countries from Latin America (Argentina, Brazil, Chile and Colombia), during a 8-year period (2012–2020), were identified and included in the study.
A first analysis on this cohort was performed comparing outcomes of patients operated on for luminal affection only or for complications of the disease.8
ParticipantsInclusion criteria: Patients submitted to primary ileocaecal resections due to CD, by conventional or laparoscopic approach, with luminal, stenotic or penetrating phenotypes.
Exclusion criteria: Previous abdominal procedures related to CD, missing data in electronic charts, and age younger than 18 years old.
Patient stratificationPatients were allocated into 2 groups, according to the presence of major postoperative complications (Clavien-Dindo>II)9 within 30 days from the procedure (POC: with complications, NPOC: without complications).
Data collection and managementInformation regarding patients’ comorbidities and operative procedures were collected in an electronic database, which was validated by three experts in colorectal surgery and biostatistics to identify key issues and to maximize completeness and accuracy of data. Local investigators fulfilled their specific databases, which were combined by the primary author (NA). The lead investigators (NA and PGK) checked the accuracy of all cases to ensure data quality. When missing data were identified, the local lead investigator was contacted and asked to complete the records.
Variables analyzedPreoperative variables included patients’ demographics (comorbidities stratified by Charlson's comorbidity score), smoking status, preoperative anemia and albumin levels, ASA score and history of previous abdominal procedures.
Variables associated to Crohn's disease included time from CD diagnosis to surgery (disease duration), Montreal classification, exposure to biological agents before surgery and within 12 weeks of the operative procedure, history of perianal disease, previous exposure to corticosteroids at the time of surgery (defined as receiving more than 20mg/day of Prednisolone for more than 6 weeks),10 and requirement of preoperative nutritional optimization before the procedure (defined as patients who needed to be hospitalized in order to receive enteral or parenteral nutrition before surgery). Proportions of early surgery (for luminal affection as defined by Maruyama et al.)11 or surgery for complications of the disease (stenoses or fistulas) were also evaluated.
Intraoperative factors included operative time, character of surgery (urgent or elective), operative approach and conversion rate, presence of intraoperative complications and their respective stratification according to CLASSIC Classification,12 requirements of associated procedures and rates of primary anastomosis. Decisions regarding the specific type of anastomosis and management of the colonic stump in patients who did not receive an anastomosis were also considered between the 2 groups.
Postoperative factors included length of hospitalization, readmission, reoperation rates, and mortality within 30 days of the procedure.
OutcomesThe main outcome of the study was to compare preoperative and intraoperative characteristics between POC and NPOC groups, aiming for identification of possible risk factors associated with 30-day postoperative major complications.
Statistical analysisStatistical analysis was performed using Stata Software (v11.1, Statacorp, College Station, Texas, USA). The categorical variables were described as percentages whereas numerical variables were described as mean or median (accordingly) with their range. The normality of each numerical variable was evaluated visually and with the Kolmogorov–Smirnov test.
We used the chi square or Fisher exact tests, as appropriate, for the comparison of categorical variables, and the Student's T or Fisher's exact test for continuous variables. OR with respective 95% CI were also calculated.
A multivariable analysis using a logistic regression model was performed including all the variables compared with a p value of less than 0.05 and those variables considered clinically significant by the investigators. A p value below 0.05 was considered statistically significant. Our primary outcome variable was the presence of major postoperative complications.
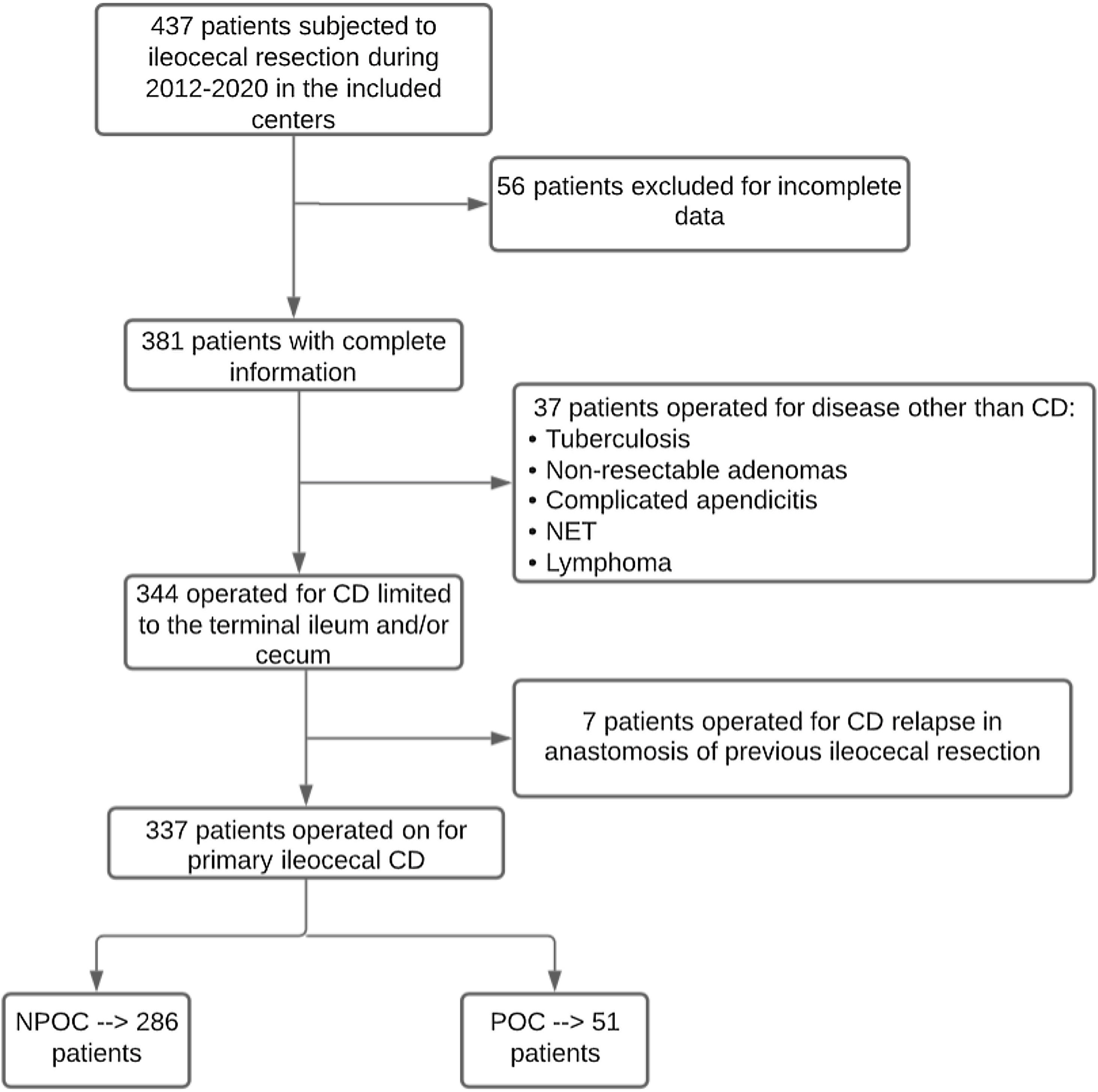
ResultsOverall, 337 patients met the inclusion criteria, of which 51 (15.13%) presented major complications and comprised the POC group. Fig. 1 describes the patient selection process, and Appendix 1 describes the number of patients included per center.
Preoperative variables
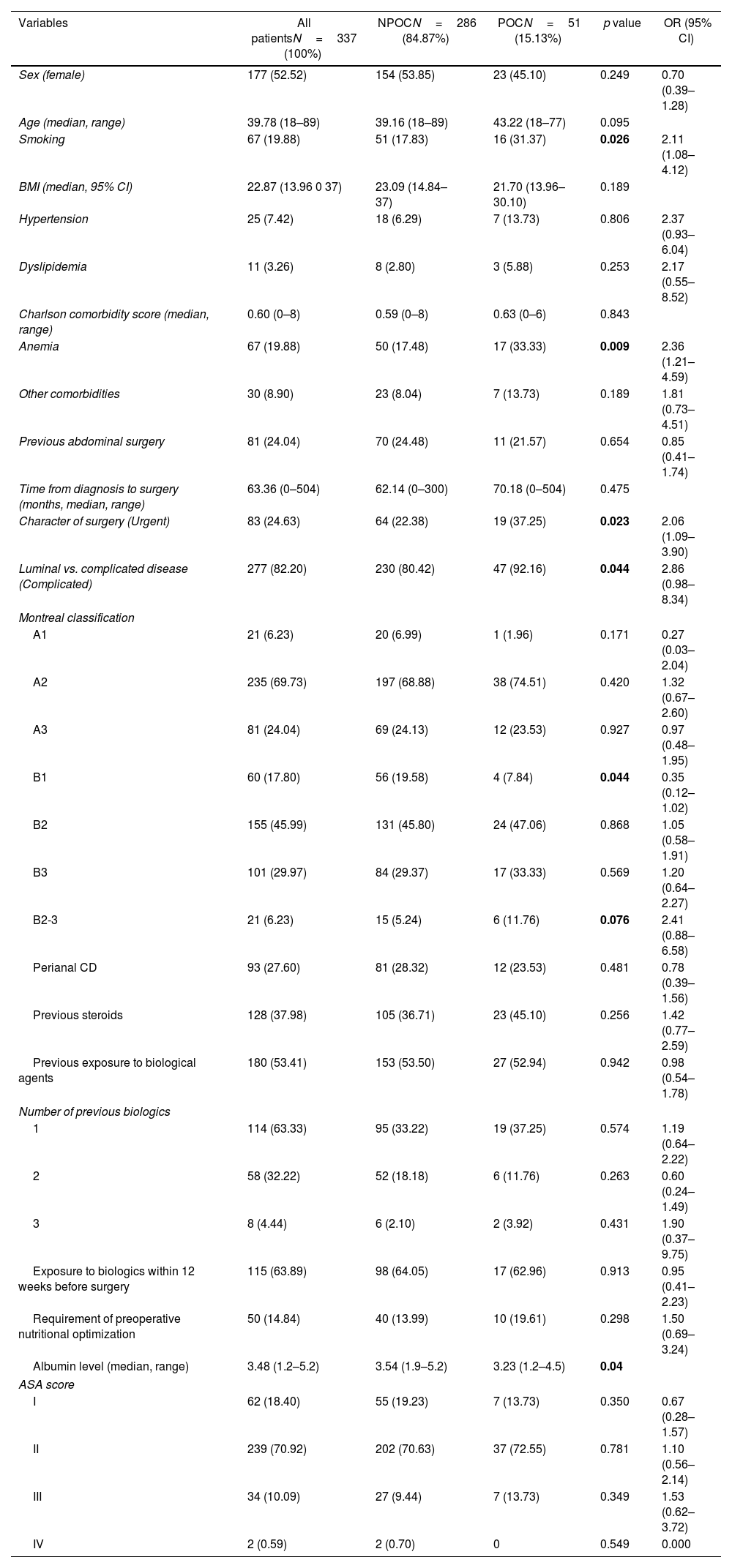
Information of included patients prior to surgery are described in detail in Table 1. No differences between POC and NPOC groups were identified in relation to sex, Charlson comorbidity score, other comorbidities, ASA score, previous abdominal procedures, and time from CD diagnosis to surgery.
Preoperative variables.
| Variables | All patientsN=337 (100%) | NPOCN=286 (84.87%) | POCN=51 (15.13%) | p value | OR (95% CI) |
|---|---|---|---|---|---|
| Sex (female) | 177 (52.52) | 154 (53.85) | 23 (45.10) | 0.249 | 0.70 (0.39–1.28) |
| Age (median, range) | 39.78 (18–89) | 39.16 (18–89) | 43.22 (18–77) | 0.095 | |
| Smoking | 67 (19.88) | 51 (17.83) | 16 (31.37) | 0.026 | 2.11 (1.08–4.12) |
| BMI (median, 95% CI) | 22.87 (13.96 0 37) | 23.09 (14.84–37) | 21.70 (13.96–30.10) | 0.189 | |
| Hypertension | 25 (7.42) | 18 (6.29) | 7 (13.73) | 0.806 | 2.37 (0.93–6.04) |
| Dyslipidemia | 11 (3.26) | 8 (2.80) | 3 (5.88) | 0.253 | 2.17 (0.55–8.52) |
| Charlson comorbidity score (median, range) | 0.60 (0–8) | 0.59 (0–8) | 0.63 (0–6) | 0.843 | |
| Anemia | 67 (19.88) | 50 (17.48) | 17 (33.33) | 0.009 | 2.36 (1.21–4.59) |
| Other comorbidities | 30 (8.90) | 23 (8.04) | 7 (13.73) | 0.189 | 1.81 (0.73–4.51) |
| Previous abdominal surgery | 81 (24.04) | 70 (24.48) | 11 (21.57) | 0.654 | 0.85 (0.41–1.74) |
| Time from diagnosis to surgery (months, median, range) | 63.36 (0–504) | 62.14 (0–300) | 70.18 (0–504) | 0.475 | |
| Character of surgery (Urgent) | 83 (24.63) | 64 (22.38) | 19 (37.25) | 0.023 | 2.06 (1.09–3.90) |
| Luminal vs. complicated disease (Complicated) | 277 (82.20) | 230 (80.42) | 47 (92.16) | 0.044 | 2.86 (0.98–8.34) |
| Montreal classification | |||||
| A1 | 21 (6.23) | 20 (6.99) | 1 (1.96) | 0.171 | 0.27 (0.03–2.04) |
| A2 | 235 (69.73) | 197 (68.88) | 38 (74.51) | 0.420 | 1.32 (0.67–2.60) |
| A3 | 81 (24.04) | 69 (24.13) | 12 (23.53) | 0.927 | 0.97 (0.48–1.95) |
| B1 | 60 (17.80) | 56 (19.58) | 4 (7.84) | 0.044 | 0.35 (0.12–1.02) |
| B2 | 155 (45.99) | 131 (45.80) | 24 (47.06) | 0.868 | 1.05 (0.58–1.91) |
| B3 | 101 (29.97) | 84 (29.37) | 17 (33.33) | 0.569 | 1.20 (0.64–2.27) |
| B2-3 | 21 (6.23) | 15 (5.24) | 6 (11.76) | 0.076 | 2.41 (0.88–6.58) |
| Perianal CD | 93 (27.60) | 81 (28.32) | 12 (23.53) | 0.481 | 0.78 (0.39–1.56) |
| Previous steroids | 128 (37.98) | 105 (36.71) | 23 (45.10) | 0.256 | 1.42 (0.77–2.59) |
| Previous exposure to biological agents | 180 (53.41) | 153 (53.50) | 27 (52.94) | 0.942 | 0.98 (0.54–1.78) |
| Number of previous biologics | |||||
| 1 | 114 (63.33) | 95 (33.22) | 19 (37.25) | 0.574 | 1.19 (0.64–2.22) |
| 2 | 58 (32.22) | 52 (18.18) | 6 (11.76) | 0.263 | 0.60 (0.24–1.49) |
| 3 | 8 (4.44) | 6 (2.10) | 2 (3.92) | 0.431 | 1.90 (0.37–9.75) |
| Exposure to biologics within 12 weeks before surgery | 115 (63.89) | 98 (64.05) | 17 (62.96) | 0.913 | 0.95 (0.41–2.23) |
| Requirement of preoperative nutritional optimization | 50 (14.84) | 40 (13.99) | 10 (19.61) | 0.298 | 1.50 (0.69–3.24) |
| Albumin level (median, range) | 3.48 (1.2–5.2) | 3.54 (1.9–5.2) | 3.23 (1.2–4.5) | 0.04 | |
| ASA score | |||||
| I | 62 (18.40) | 55 (19.23) | 7 (13.73) | 0.350 | 0.67 (0.28–1.57) |
| II | 239 (70.92) | 202 (70.63) | 37 (72.55) | 0.781 | 1.10 (0.56–2.14) |
| III | 34 (10.09) | 27 (9.44) | 7 (13.73) | 0.349 | 1.53 (0.62–3.72) |
| IV | 2 (0.59) | 2 (0.70) | 0 | 0.549 | 0.000 |
Univariate comparative analysis of preoperative characteristics between groups. Categorical variables described as percentages whereas numerical variables were described as mean or median (accordingly) with their range. Normality of each numerical variable was evaluated visually and with the Kolmogorov–Smirnov test. Chi square or Fisher exact tests, as appropriate, for the comparison of categorical variables, and the Student's T or Fisher's exact test for continuous variables. OR with respective 95% CI also calculated.
An additional analysis stratifying time from diagnosis to surgery into three categories (less than 2 years, 2–5 years, and more than 5 years) was performed, which also did not show differences between groups.
On the other hand, POC patients presented higher rates of smoking (31.37 vs. 17.83%, p=0.026, OR: 2.11), preoperative anemia (33.33 vs. 17.48, p=0.009, OR: 2.36), and operations in an urgent setting (37.25 vs. 22.38%, p=0.023, OR: 2.06). Operations for complicated disease (when compared to luminal phenotype) were also more frequent in the POC group. Albumin levels were lower in the POC group (3.23 vs. 3.54, p=0.04). The rate of exposure to steroids at the time of surgery was numerically higher in the POC group, but this difference was not statistically significant (45.10 vs. 36.71%, p=0.256). Previous perianal CD, previous use of biological agents, exposure to these drugs within 3 months of surgery, and requirements of preoperative nutritional optimization were similar in POC and NPOC patients. Lastly, no difference was seen as regards exposure to different types of biologic agents and the presence of complications.
Intraoperative variablesIntraoperative information is described in detail in Table 2.
Intraoperative variables.
| Variables | All patientsN=337 (100%) | NPOCN=286 (84.87%) | POCN=51 (15.13%) | p value | OR (95% CI) |
|---|---|---|---|---|---|
| Operative time (median, range) | 151.43 (45–420) | 143.86 (45–360) | 188.77 (60–420) | 0.005 | |
| Approach | |||||
| Laparoscopic | 173 (51.34) | 148 (51.75) | 25 (49.02) | 0.719 | 0.90 (0.49–1.63) |
| Conventional | 164 (48.66) | 138 (48.25) | 26 (50.98) | 0.719 | 1.11 (0.61–2.03) |
| Conversion rate | 18/173 (10.40) | 14/148 (9.46) | 4/25 (16) | 0.322 | 1.82 (0.54–6.11) |
| Requirement of associated procedures | 53 (15.73) | 41 (14.34) | 12 (23.53) | 0.097 | 1.84 (0.89–3.82) |
| Intraoperative complications | 22 (6.53) | 13 (4.55) | 9 (17.65) | 0.000 | 4.50 (1.78–11.38) |
| CLASSIC minor | 19/22 (86.36) | 13/22 (100) | 6/9 (66.67) | 0.025 | |
| CLASSIC major | 3/22 (13.64) | 0 | 3/9 (33.33) | 0.025 | |
| Primary anastomosis | 310 (91.99) | 268 (93.71) | 42 (82.35) | 0.006 | 0.31 (0.13–0.75) |
| Type of anastomosis | |||||
| Hand-sewn | 47/310 (15.16) | 38/268 (14.18) | 9/42 (21.43) | 0.223 | 1.81 (0.82–4.03) |
| Stapled | 263/310 (84.84) | 230/268 (85.82) | 33/42 (78.57) | 0.223 | 0.61 (0.27–1.37) |
| Hand-sewn | |||||
| One layer | 23/47 (48.94) | 18/38 (47.37) | 5/9 (55.56) | 0.882 | 1.11 (0.27–4.54) |
| Two-layer | 24/47 (51.06) | 20/38 (52.63) | 4/9 (44.44) | 0.477 | 0.60 (0.24–2.53) |
| Anastomotic configuration | |||||
| End-to-end | 28/310 (9.03) | 25/268 (9.33) | 3/42 (7.14) | 0.646 | 0.96 (0.31–3.00) |
| End-to-side | 30/310 (9.68) | 27/268 (10.07) | 3/42 (7.14) | 0.550 | 0.96 (0.31–3.00) |
| Side-to-side | 252/310 (81.29) | 216/268 (80.60) | 36/42 (85.71) | 0.429 | 1.44 (0.58–3.62) |
| Anastomotic orientation | |||||
| Isoperistaltic | 57/310 (18.39) | 51/268 (19.03) | 6/42 (14.29) | 0.461 | 1.41 (0.56–3.53) |
| Anti-peristaltic | 253/310 (81.61) | 217/268 (80.97) | 36/42 (85.71) | 0.461 | 0.82 (0.34–1.96) |
| Decision after resection | |||||
| Anastomosis w/o diversion | 292 (86.65) | 252 (88.11) | 40 (78.43) | 0.061 | 0.49 (0.23–1.05) |
| Diverted anastomosis | 18 (5.34) | 15 (5.24) | 3 (5.88) | 0.852 | 1.13 (0.31–4.06) |
| End ileostomy, intra abdominal stump | 7 (2.08) | 5 (1.75) | 2 (3.92) | 0.316 | 2.29 (0.43–12/22) |
| End ileostomy, subcutaneous stump | 13 (3.86) | 11 (3.85) | 2 (3.92) | 0.979 | 1.02 (0.22–4.76) |
| End ileostomy, mucous fistula | 7 (2.08) | 3 (1.05) | 4 (7.84) | 0.002 | 8.03 (1.70–37.96) |
| Postoperative antibiotics | 169 (50.15) | 130 (45.45) | 39 (76.47) | 0.000 | 3.90 (1.92–7.90) |
Univariate comparative analysis of intraoperative characteristics between groups. Categorical variables described as percentages whereas numerical variables were described as mean or median (accordingly) with their range. Normality of each numerical variable was evaluated visually and with the Kolmogorov–Smirnov test. Chi square or Fisher exact tests, as appropriate, for the comparison of categorical variables, and the Student's T or Fisher's exact test for continuous variables. OR with respective 95% CI also calculated.
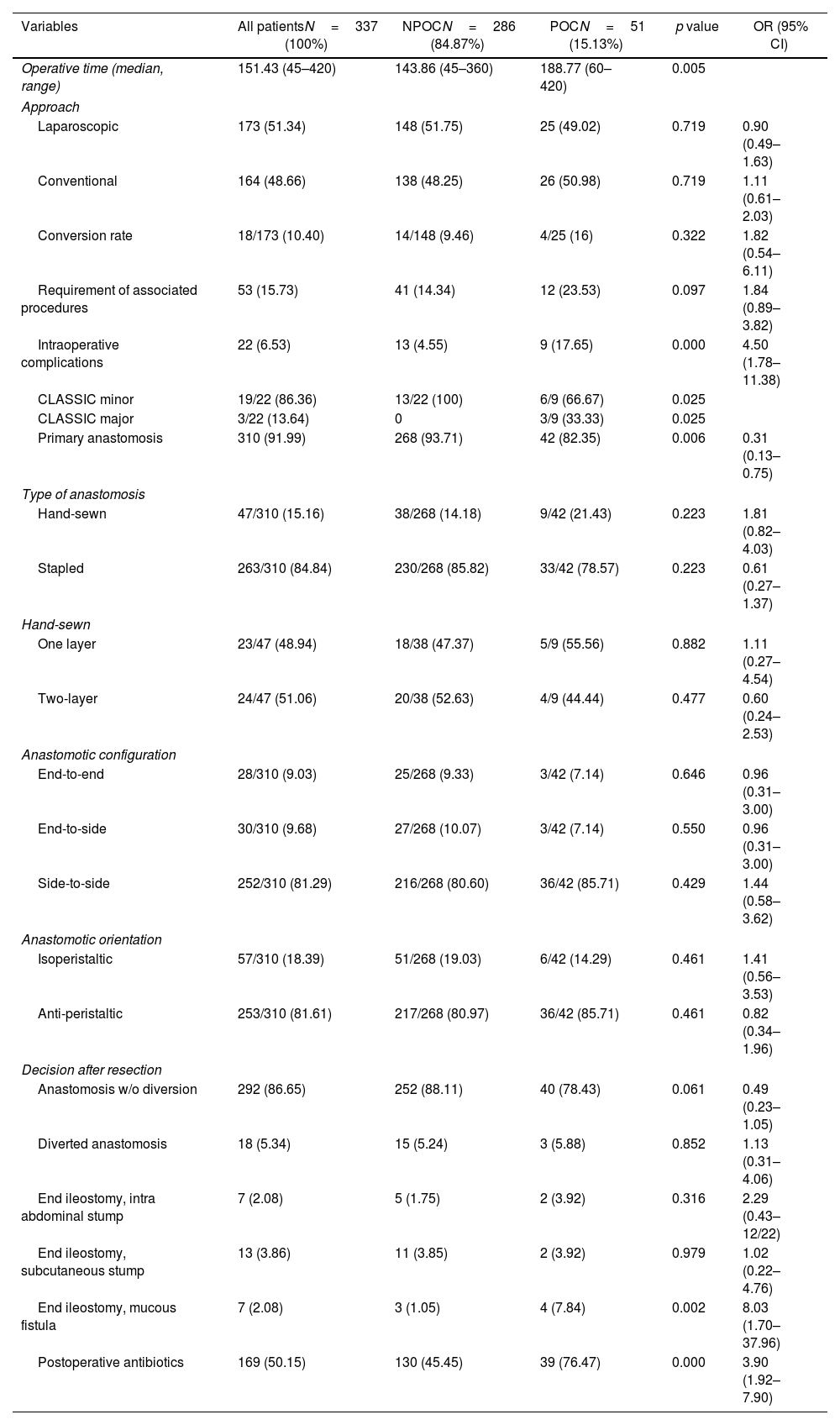
Patients from the POC group had a significantly longer operative time (188.77 vs. 143.86%, p=0.005), numerically higher rates of associated procedures (23.53 vs. 14.34%, p=0.097) and intraoperative complications (17.65 vs. 4.55, p<0.001). On the contrary, patients in the NPOC group presented a higher proportion of primary anastomosis (93.71 vs. 82.35, p=0.006) and lower need for postoperative antibiotics (45.45 vs. 76.47, p<0.001, OR: 3.90).
The overall proportion of minimally invasive surgery was 51.34%, with no difference between the groups in terms of initial laparoscopic approach. Even though conversion rates were numerically higher in the POC group, the difference was not significant (16 vs. 9.46%, p=0.322). Different types of anastomoses were included in the analysis. Side-to-side, anti-peristaltic stapled anastomosis was the most common anastomotic configuration. No differences were identified between the groups regarding the specific type of anastomosis. Lastly, regarding management of the colonic stump in patients without primary anastomosis, POC patients presented a higher proportion of ileostomy and colonic mucous fistula.
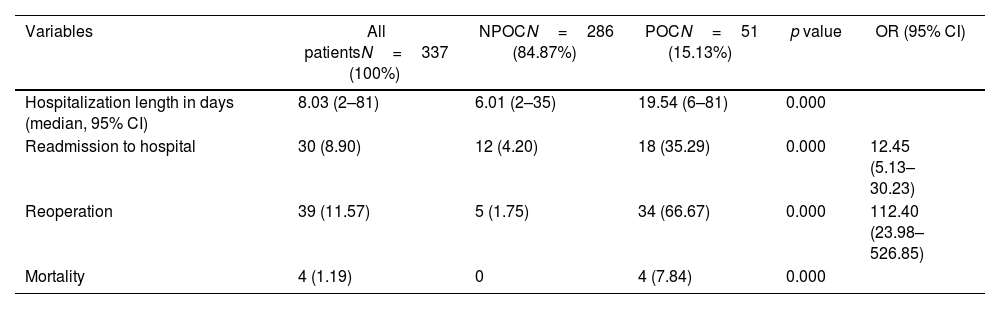
Postoperative outcomesPostoperative variables are detailed in Table 3. Patients from the POC group had significantly longer hospitalization stay (19.54 vs. 5.48 days, p<0.001), higher rates of readmissions to hospital (35.29 vs. 4.20, p<0.001), reoperations (66.67 vs. 1.75, p<0.001) and mortality (7.84 vs. 0, p<0.001) within 30 days of the index operation.
Postoperative variables.
| Variables | All patientsN=337 (100%) | NPOCN=286 (84.87%) | POCN=51 (15.13%) | p value | OR (95% CI) |
|---|---|---|---|---|---|
| Hospitalization length in days (median, 95% CI) | 8.03 (2–81) | 6.01 (2–35) | 19.54 (6–81) | 0.000 | |
| Readmission to hospital | 30 (8.90) | 12 (4.20) | 18 (35.29) | 0.000 | 12.45 (5.13–30.23) |
| Reoperation | 39 (11.57) | 5 (1.75) | 34 (66.67) | 0.000 | 112.40 (23.98–526.85) |
| Mortality | 4 (1.19) | 0 | 4 (7.84) | 0.000 |
Univariate comparative analysis of postoperative characteristics between groups. Categorical variables described as percentages whereas numerical variables were described as mean or median (accordingly) with their range. Normality of each numerical variable was evaluated visually and with the Kolmogorov–Smirnov test. Chi square or Fisher exact tests, as appropriate, for the comparison of categorical variables, and the Student's T or Fisher's exact test for continuous variables. OR with respective 95% CI also calculated.
16 patients (5.16%) presented an anastomotic leakage after surgery, and most of them required a reoperation.
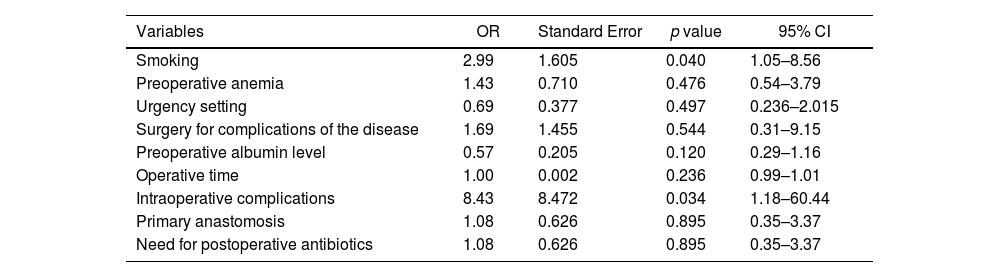
Multivariate analysisTable 4 described the results of multivariable analysis. Smoking (OR=2.99, p=0.040) and intraoperative complications (OR=8.43, p=0.034) were independently associated with the occurrence of postoperative major complications.
Multivariate analysis.
| Variables | OR | Standard Error | p value | 95% CI |
|---|---|---|---|---|
| Smoking | 2.99 | 1.605 | 0.040 | 1.05–8.56 |
| Preoperative anemia | 1.43 | 0.710 | 0.476 | 0.54–3.79 |
| Urgency setting | 0.69 | 0.377 | 0.497 | 0.236–2.015 |
| Surgery for complications of the disease | 1.69 | 1.455 | 0.544 | 0.31–9.15 |
| Preoperative albumin level | 0.57 | 0.205 | 0.120 | 0.29–1.16 |
| Operative time | 1.00 | 0.002 | 0.236 | 0.99–1.01 |
| Intraoperative complications | 8.43 | 8.472 | 0.034 | 1.18–60.44 |
| Primary anastomosis | 1.08 | 0.626 | 0.895 | 0.35–3.37 |
| Need for postoperative antibiotics | 1.08 | 0.626 | 0.895 | 0.35–3.37 |
Multivariable analysis using a logistic regression model including all the variables compared with a p value of less than 0.05 and those variables considered clinically significant by the investigators. A p value below 0.05 was considered statistically significant, using postoperative major complications as dependent variable.
The present study presents a large group of patients operated for primary ileocaecal CD and comprises one of the first international multicentric experiences regarding surgical treatment of CD patients from different countries of Latin America. In multivariable analysis, smoking and intraoperative complications were independently associated with higher rates of postoperative morbidity.
Since postoperative morbidity after resections still represents one of the major problems in the management of CD (especially when compared to other intestinal problems),13 several studies have been published in recent years, aiming to determine specific factors which could possibly affect postoperative outcomes. Some risk factors for major complications have been extensively described, as smoking,14 preoperative anemia,15,16 urgent procedures,14,17 penetrating disease,5,15,17–20 hypoalbuminemia20–22 and previous exposure to steroids.14,18,19,23 Our study presented similar findings in univariate analysis, as smoking, preoperative anemia, urgent surgery and complicated disease (stenotic or penetrating) were more frequently observed in patients with postoperative complications.
On the other hand, previous exposure to biological agents has been subjected to an endless debate as to its relation (or not) to worse postoperative outcomes. Despite some studies identifying a correlation between preoperative anti-TNF agents and higher rate of postoperative complications,16,23–25 a large meta-analysis including information of 18 non-randomized studies failed to find an association between Infliximab and overall complications.27 Furthermore, the prospective multicentric PUCCINI trial28 evaluated postoperative morbidity in IBD patients exposed to biologics and also did not demonstrate an association between these drugs and worse postoperative outcomes. Overall infections (18.1% vs 20.2%, p=0.469) and surgical site infections (12.0% vs 12.6%, p=0.889) rates were similar in patients previously exposed to anti-TNF agents and those unexposed. In multivariable analysis, current exposure to these agents was not associated with overall infections (OR, 1.050; 95% CI, 0.716–1.535) or surgical site infection (OR, 1.249; 95% CI, 0.793–1.960). Detectable concentrations of anti-TNF agents were not associated with infectious complications. In our study, preoperative exposure to biologics was observed in 52.94% of patients with postoperative major complications and 53.5% of those without morbidity (p=0.942), findings which are compatible with most retrospective studies and the prospective aforementioned PUCCINI trial. Guidelines still do not present specific formal recommendations regarding preoperative use of biologics,29 and more cause-effect relationship studies are warranted.
Few studies have investigated intraoperative factors in ileocaecal resections due to CD and their possible relation to postoperative complications. Our study identified that prolonged operative time and intraoperative complications negatively impacted postoperative morbidity, whereas receiving a primary anastomosis seemed to work as a protective factor. A possible reason for this finding is that surgeons, facing patients in worse conditions or requiring more complex procedures, could be less eager to perform a primary anastomosis (selection bias). Postoperative antibiotics were also more needed in patients with complications, which could be partially explained by the fact that this group faced more complex surgery, with longer operative time and more complicated disease.
In our study, the presence of postoperative major complications had a major impact in other postoperative indicators, including requirements of prolonged hospitalization and higher rates of reoperations, readmissions as well as mortality. This highlights the interest in defining preoperative risk factors for these events, with special interest in modifiable characteristics, such as smoking or delayed surgical indication.
Since this is one of the first multicentric Latin American studies looking into surgical treatment of CD patients, it is interesting to have a snapshot of operative characteristics. Initially, the overall 51% rate of laparoscopic procedures seems low in the minimally invasive surgery era. However, when looking at other studies, one can observe that the proportion of laparoscopic cases in these publications is below 60%.5,14–26,30 This could be due to the fact that the main indication for surgery in patients with CD is still represented by disease complications, such as long fibrotic stenosis, internal or external fistulas, and inflammatory masses which can limit decision toward a laparoscopic surgical approach.
Overall, the rate of primary anastomosis was high in our cohort of patients, and the most common type and configuration of the performed anastomoses (stapled, side-to-side) was compatible with what is suggested by international guidelines.29 Even though there is no consensus on the management of the colonic stump when a primary anastomosis is not performed, the tendency for exteriorization as a double-loop stoma or mucous fistula instead of an intra-abdominal stump which was observed in patients with complications can be explained by the fact that patients in poor general condition might be at risk of colonic stump leakages and consequent septic complications.
Our study is associated with some inherent limitations, such as its retrospective nature and the low number of patients with complications. Furthermore, practices may vary between the centers, and the surgeons’ experience and expertise were not evaluated in detail (some cases could be performed by junior, others by senior staff members, and some by residents under assistance). Minimally invasive resections were performed in 60% of cases, which reflects the reality of our continent in colorectal surgery in general. We also did not carry out possible differences between centers, as some centers included less patients than others and this was not the main purpose of our analysis. Groups were also not considered fully homogeneous, as some variables differed between patients with and without associated morbidity. Another limitation is that no specific sample calculation was possible, and we worked with a convenience sample.
On the other hand, the present study's main strength is that it represents the very first solid international multicentric analysis of postoperative outcomes from Latin America, which may assist in surgical management of CD in our continent.
In summary, smoking and the presence of intraoperative complications were identified as predictors of postoperative major complications after ileocaecal resections in CD and may have an important impact in different postoperative indicators. This international study focuses efforts in gathering more experience in the surgical management of CD in Latin America. More prospective research aiming identification of preoperative risk factors for postoperative complications is warranted, in order to properly optimize patients for ileocaecal resections in our region.
FundingThis study has not been funded.
Conflict of interestThe authors declare no conflict of interest.
The following are the supplementary data to this article:

