




Spontaneous hemoperitoneum secondary to intraabdominal metastasis is a very severe, rare emergency that is very difficult to diagnose. The symptoms and medical history of the patient should be considered from the onset.
Spontaneous intraabdominal bleeding is a very uncommon initial symptom in patients with intraabdominal metastases. Less than 2% of cases1 present this symptom, and there are few reports in the literature. The primary tumours that are responsible can be very varied (melanoma, testicular, colon, stromal, etc.).2 However, papillary renal cell carcinoma, with the intense microvascularisation of its metastases,3 is an entity to consider, as we present in the following case report. Given the atypical location of the metastasis, there are no previous reports of this type in the literature.
The patient is a 76-year-old male with a history of type 2 diabetes mellitus, dyslipidaemia and arterial hypertension under medical treatment, and an infrarenal aortic aneurism measuring 4.8cm that was under surveillance. In September 2014, the patient was diagnosed with type 2 papillary renal cell carcinoma and underwent laparoscopic right partial nephrectomy (pathology: pT1aN0). The patient's post-operative progression was favourable.
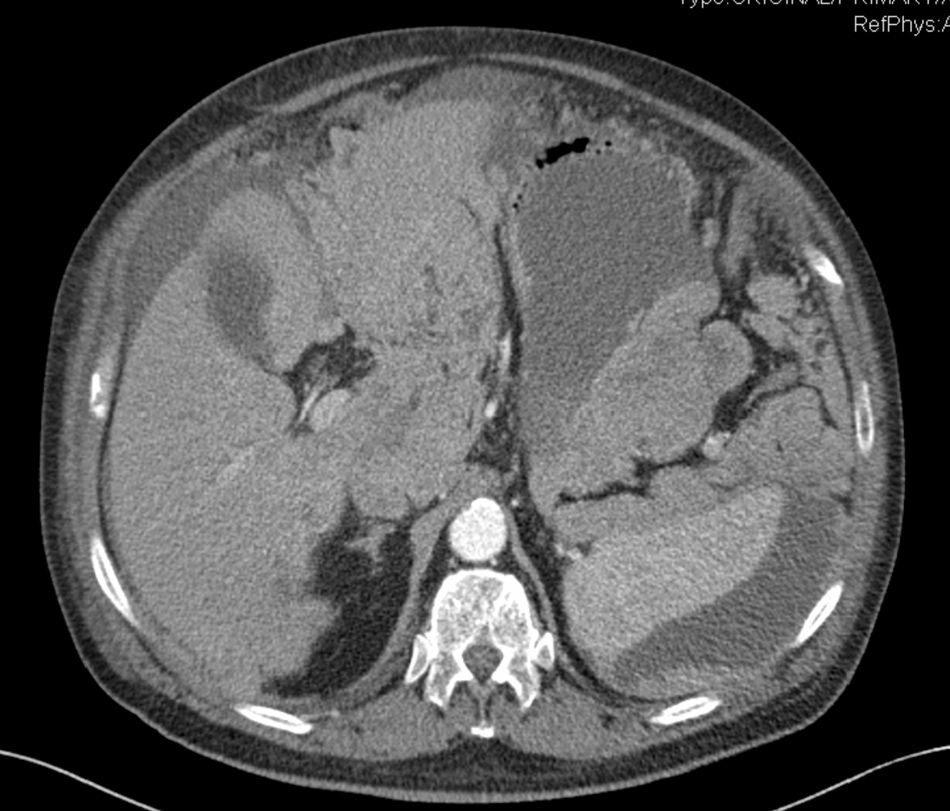
Six months after the surgery, the patient came to the emergency room with generalised abdominal pain, predominantly in the right hypochondrium and mesogastrium over the previous 24h, associated with sweating and dizziness. On physical examination, the patient presented hypotension at 100/40mmHg, 110bpm and a distended abdomen with diffuse pain and signs of peritoneal irritation. Blood work showed hemoglobin 8.4mg/dL, hematocrit 25%, and normal coagulation levels. Emergency CT scan reported anuncomplicated abdominal aortic aneurysm and widespread abundant free fluid, especially in the superior hemiabdomen and pelvis (probably related with hemoperitoneum), as well as a tumour-looking mass of the round ligament of the liver (Fig. 1).

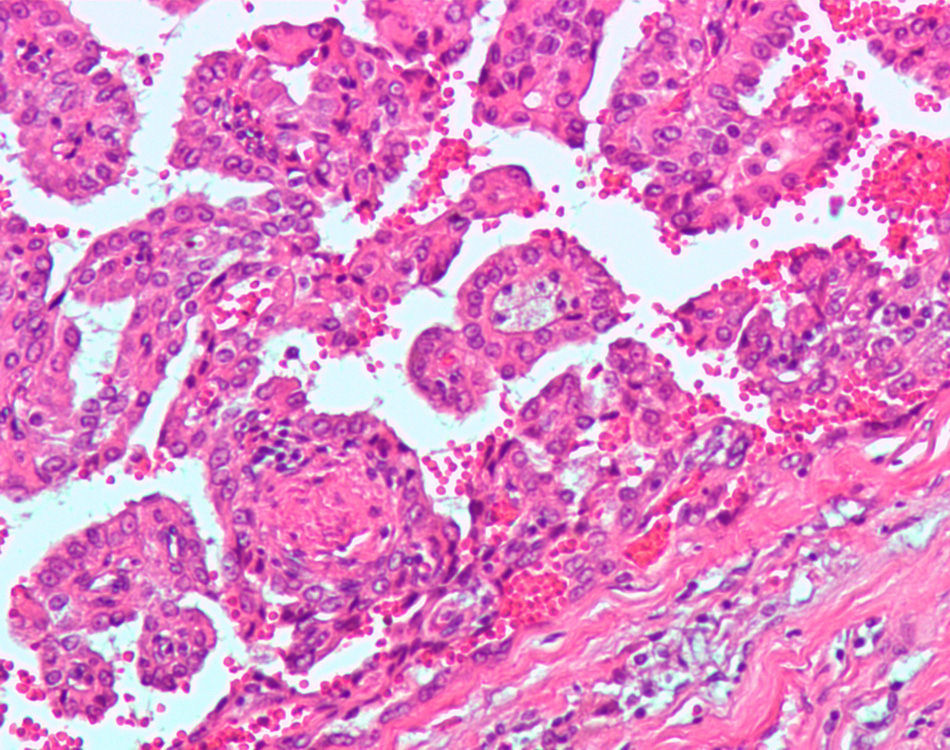
Given these findings, urgent exploratory laparotomy was indicated, which revealed diffuse hemoperitoneum of more than 3L, secondary to a metastatic mass measuring 10cm and encompassing the round ligament with signs of active bleeding and extension to the hepatic hilum. There was no involvement of the liver parenchyma. Hemostasis of the lesions was achieved, multiple biopsies were taken, and an intraabdominal drain was inserted. The patient required transfusion of 3 units of packed red blood cells due to a postoperative hemoglobin level of 7.4mg/dL, which later remained stable at around 10.5mg/dL. The postoperative evolution was favourable, although the pathology study of the round ligament lesion reported “metastasis of papillary renal cell carcinoma CD10+ with abundant hemorrhagic areas and neovascularisation” (Fig. 2). The patient was referred to the oncology department in order to initiate palliative chemotherapy treatment.

Spontaneous hemoperitoneum is an uncommon cause of acute abdominal pain and is defined as the presence of blood in the peritoneal cavity in the absence of previous trauma. This clinical condition carries a high mortality rate in the absence of a prompt diagnosis.4 There are multiple causes of spontaneous hemoperitoneum, including hepatic, splenic, gynaecological, vascular and altered coagulation states.5 Among the hepatic causes, hepatic adenoma and hepatocarcinoma in a cirrhotic liver are the most frequent causes of spontaneous hemoperitoneum.6 Massive bleeding due to tumour metastases is an uncommon condition1 that may originate in metastases in the colon, lungs, kidneys or testicles. Reports of metastasis in the round ligament are exceptional in the literature, and the only case described involved breast cancer metastasis.7 We have found no reports in the literature of hemoperitoneum due to bleeding lesions in this region. The location of papillary renal cell carcinoma metastases is very variable, but they most frequently affect the lungs (13%), bones (8%), skin (7%) and liver (6%). Because of their histopathology, they are highly vascularised tumours whose metastases tend to bleed,8 so they are an aetiology to keep in mind.
We the authors believe that the peculiarity of this case report lies not only in the origin or the atypical location of the bleeding but also in the importance of a proper differential diagnosis in situations of acute abdomen and anaemia in patients with a history of neoplasms, especially in tumours with a tendency to produce metastases in the liver or other richly vascularised organs.
Please cite this article as: Abellán I, González A, Bernabé A, González P. Hemoperitoneo espontáneo secundario a metástasis en el ligamento redondo hepático, una presentación atípica. Cir Esp. 2016;94:184–186.
