






Physicians, especially surgeons, are significatively affected by burnout. Duty-hour violation, as well as discrimination, abuse and sexual harassment may contribute to burnout. A study about this topic has been published in residents from United States, demonstrating a high incidence of burnout. Our objective is to know which is the situation in Spain and to compare it with United States.
MethodsCross-sectional observational study carried out in January-February 2020, based on the responses to a validated survey administered to General Surgery residents in Spain.
ResultsThere are 931 General Surgery Residents. 739 have entered in the survey and 452 (61.2%) eventually responded to it. In any occasion during the training period, 55.1% reported discrimination based on their gender, 8.8% reported racial discrimination, 73.9% reported verbal/psychological abuse, 7.1% reported physical abuse and 16.4% reported sexual harassment. Attending surgeons are the most frequent source of sexual harassment and physical and verbal abuse, whereas patients are the most frequent cause of gender discrimination. Burnout symptoms were reported by 47.6% of residents and 4.6% reported suicidal thoughts. 98% of residents reported duty-hour violations and 47% of them do not have the day off after to be on call. Both of these issues are burnout predictive factors.
ConclusionsMistreatment (discrimination, abuse and harassment) occurs among General Surgery residents during their training period in our country. Every kind of mistreatment is more frequent in Spain than in the United States, with the exception of racial discrimination. It is associated with exceeding weekly duty-hour. It is necessary to know these problems and to avoid them in order to improve work environment of General Surgery training period.
El desgaste profesional o burnout afecta significativamente a los médicos y, concretamente, a los cirujanos. El exceso de horas de trabajo, así como la discriminación, abuso y acoso sexual, pueden contribuir al desgaste profesional. Recientemente se ha publicado un estudio sobre este tema en residentes de Estados Unidos que demuestra una elevada incidencia de burnout. El objetivo de nuestro estudio es conocer cuál es la situación en España y compararla con lo que sucede en aquel país.
MétodosEstudio observacional, transversal, efectuado en enero-febrero del 2020, a través de una encuesta validada remitida a todos los residentes de Cirugía General y del Aparato Digestivo (CGAD) de España.
ResultadosDe los 931 residentes de CGAD, 739 accedieron a la encuesta y 452 (61,2%) la cumplimentaron. En alguna ocasión durante la residencia, el 55,1% de los residentes se han sentido discriminados por su género, el 8,8% por su país de origen, el 73,9% afirman haber experimentado abuso verbal/psicológico, el 7,1% abuso físico y el 16,4% acoso sexual. Los cirujanos adjuntos son la causa más frecuente de acoso sexual, abuso físico y verbal. Los pacientes son el origen más común de la discriminación por género. El 47,6% ha tenido síntomas de desgaste profesional y el 4,6% ha presentado ideas suicidas. El 98% ha excedido su jornada laboral y el 47% no libra las guardias. Estos dos últimos puntos son factores predictivos de desgaste profesional.
ConclusionesDurante el periodo de residencia en nuestro país, los residentes de CGAD han sufrido episodios de maltrato en forma de discriminación, abuso y acoso. Todos los tipos de maltrato son más frecuentes en España que en Estados Unidos, excepto la discriminación racial. Con ello se asocia el incumplimiento significativo en las horas de trabajo semanal. Es necesario reconocer estas anomalías y evitarlas para favorecer un ambiente adecuado para la formación profesional especializada en CGAD.
Professional burnout is a topic of interest today as it affects many professionals from various fields. Medicine, and surgery in particular, are especially affected by burnout. Its prevalence in the healthcare services is very variable, ranging from 0% to 80.5%.1
Professional burnout is defined as a situation of emotional exhaustion, depersonalization and decreased personal satisfaction related to work, which leads to physical and psychological fatigue.1,2 It is associated with depression, alcohol abuse, and suicide.3 This situation not only affects the health of the person who suffers from it, but their professional performance is also significantly affected as well. In the medical field, it has a negative impact on the quality of care offered to patients. Various studies show that burnout among medical professionals is associated with a higher incidence of medical errors and lower patient satisfaction.1
Mistreatment, including discrimination, abuse or sexual harassment, contributes to burnout. These forms of abuse are rather frequent in the medical field, especially among female residents.4 Recently, a study was published in The New England Journal of Medicine on discrimination, abuse, harassment and burnout in Gastrointestinal and General Surgery residents in the United States.5 They conducted a nationwide survey to assess the frequency and origin of such behaviors. They reported that, during residency, 31.9% of surgical residents had suffered sexual discrimination, 30.3% physical or verbal abuse, 10.3% sexual harassment, and 4.5% had had suicidal thoughts in the last year.
The evidence of burnout during the first years of work experience is a concern because it can affect the final objective, which is the training of medical specialists. Thus, we wondered about the situation in our setting. As a result, the Spanish Association of Surgeons (AEC) and the National Commission of Specialists in (CNE) designed a cross-sectional study based on a survey of all surgical residents in Spain.
The main objective of our study was to determine the situation of professional burnout in our country to be able to implement solutions if they are necessary. The secondary objective was to compare what happens in Spain versus the situation described in the United States.5
MethodsStudy designA cross-sectional study.
Setting and participantsThe study was conducted from January to February 2020. An anonymous survey was sent to all CGAD residents in Spain (Addendum I). It was the same survey used in the American study, sponsored by the American College of Surgeons and the Accreditation Council for Graduate Medical Education, after being previously validated.5,6 The delivery method was by email through the AEC.
VariablesDemographic variables included: year of residence, gender, year of birth, country of origin, number of hospital beds, number of residents per year, autonomous community where the hospital is located.
Variables about discrimination, harassment and abuse included: sexual discrimination, national origin discrimination, discrimination due to having been/being/intending to become pregnant or needing time to care for children, sexual harassment, physical abuse, verbal/psychological abuse, and the source of such discrimination/harassment/abuse.
Variables related to burnout: frequency with which “I think I treat my patients very effectively,” “I think I am treating my patients as if they were impersonal objects,” “I feel that my work is wearing me down emotionally,” “When I get up in the morning and face another day of work, I feel fatigued,” “I have become more insensitive since I started the residency,” “I think that with my work I am positively influencing the lives of my patients,” “Working all day with patients stresses me out,” “I don’t really care what happens to some of my patients,” “Working all day takes a lot of effort and is tiring.”
Other variables were: months in which the work hours had exceeded 60 hours per week in the last year, number of night duties per month on average in the last year, day off after night duty, and suicidal thoughts.
Data source and biasesThe surveys were sent blind, without knowledge of the result of other participants. For further motivation, the survey was resent a second time.
Study sample sizeIn February 2020, there were a total of 931 surgical residents from all years of residency training in hospitals across Spain. The survey was sent to each and every one of them in an attempt to achieve maximum representation nation-wide.
Through the company Imedia, hired by the AEC, the results of all the surveys were recorded and the initial descriptive study was carried out.
This is a cross-sectional observational study, based on a survey, adapted to the criteria of the Declaration of Helsinki. The STROBE guidelines for cross-sectional observational studies have been followed.
Statistical analysisThe SPSS program version 23 was used. All the variables analyzed have been categorical and have been described in absolute numbers and percentages. A multivariate logistic regression analysis was used to obtain a predictive model to identify the factors that predict burnout. Using forward and backward stepwise regression, a model was created with the predictive factors. Once the final prediction equation was established, the regression coefficients were converted to scores using test algorithms.
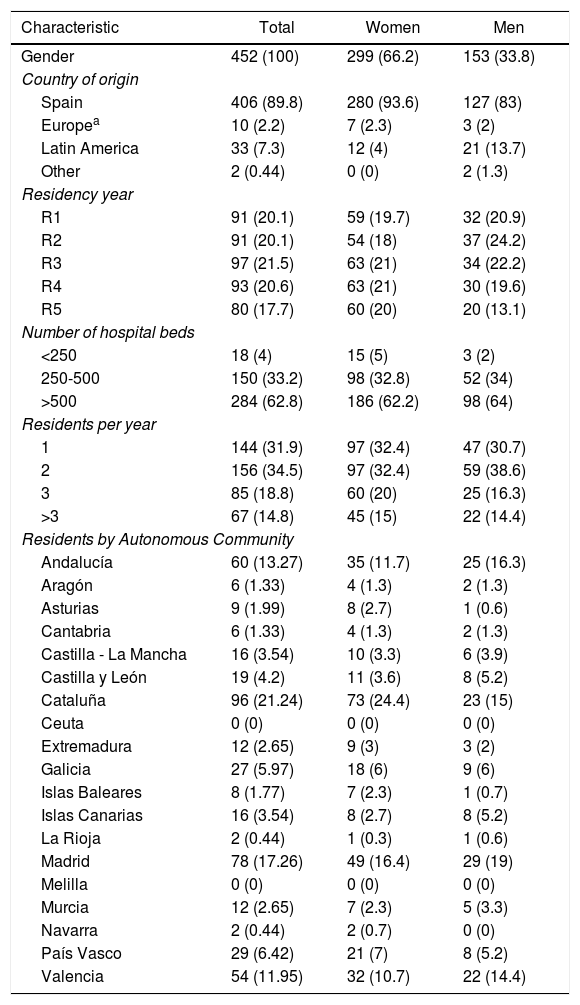
ResultsIn total, there are 931 surgical residents in Spain, 739 (79.4%) of whom accessed the survey through the link, and 452 (61.2%) completed the survey; 299 (66.2%) of the people who answered the survey were women. The demographic characteristics of the population studied are described in Table 1.
Demographic characteristics of Gastrointestinal and General Surgery residents in Spain.
| Characteristic | Total | Women | Men |
|---|---|---|---|
| Gender | 452 (100) | 299 (66.2) | 153 (33.8) |
| Country of origin | |||
| Spain | 406 (89.8) | 280 (93.6) | 127 (83) |
| Europea | 10 (2.2) | 7 (2.3) | 3 (2) |
| Latin America | 33 (7.3) | 12 (4) | 21 (13.7) |
| Other | 2 (0.44) | 0 (0) | 2 (1.3) |
| Residency year | |||
| R1 | 91 (20.1) | 59 (19.7) | 32 (20.9) |
| R2 | 91 (20.1) | 54 (18) | 37 (24.2) |
| R3 | 97 (21.5) | 63 (21) | 34 (22.2) |
| R4 | 93 (20.6) | 63 (21) | 30 (19.6) |
| R5 | 80 (17.7) | 60 (20) | 20 (13.1) |
| Number of hospital beds | |||
| <250 | 18 (4) | 15 (5) | 3 (2) |
| 250-500 | 150 (33.2) | 98 (32.8) | 52 (34) |
| >500 | 284 (62.8) | 186 (62.2) | 98 (64) |
| Residents per year | |||
| 1 | 144 (31.9) | 97 (32.4) | 47 (30.7) |
| 2 | 156 (34.5) | 97 (32.4) | 59 (38.6) |
| 3 | 85 (18.8) | 60 (20) | 25 (16.3) |
| >3 | 67 (14.8) | 45 (15) | 22 (14.4) |
| Residents by Autonomous Community | |||
| Andalucía | 60 (13.27) | 35 (11.7) | 25 (16.3) |
| Aragón | 6 (1.33) | 4 (1.3) | 2 (1.3) |
| Asturias | 9 (1.99) | 8 (2.7) | 1 (0.6) |
| Cantabria | 6 (1.33) | 4 (1.3) | 2 (1.3) |
| Castilla - La Mancha | 16 (3.54) | 10 (3.3) | 6 (3.9) |
| Castilla y León | 19 (4.2) | 11 (3.6) | 8 (5.2) |
| Cataluña | 96 (21.24) | 73 (24.4) | 23 (15) |
| Ceuta | 0 (0) | 0 (0) | 0 (0) |
| Extremadura | 12 (2.65) | 9 (3) | 3 (2) |
| Galicia | 27 (5.97) | 18 (6) | 9 (6) |
| Islas Baleares | 8 (1.77) | 7 (2.3) | 1 (0.7) |
| Islas Canarias | 16 (3.54) | 8 (2.7) | 8 (5.2) |
| La Rioja | 2 (0.44) | 1 (0.3) | 1 (0.6) |
| Madrid | 78 (17.26) | 49 (16.4) | 29 (19) |
| Melilla | 0 (0) | 0 (0) | 0 (0) |
| Murcia | 12 (2.65) | 7 (2.3) | 5 (3.3) |
| Navarra | 2 (0.44) | 2 (0.7) | 0 (0) |
| País Vasco | 29 (6.42) | 21 (7) | 8 (5.2) |
| Valencia | 54 (11.95) | 32 (10.7) | 22 (14.4) |
Expressed as number (percentage).
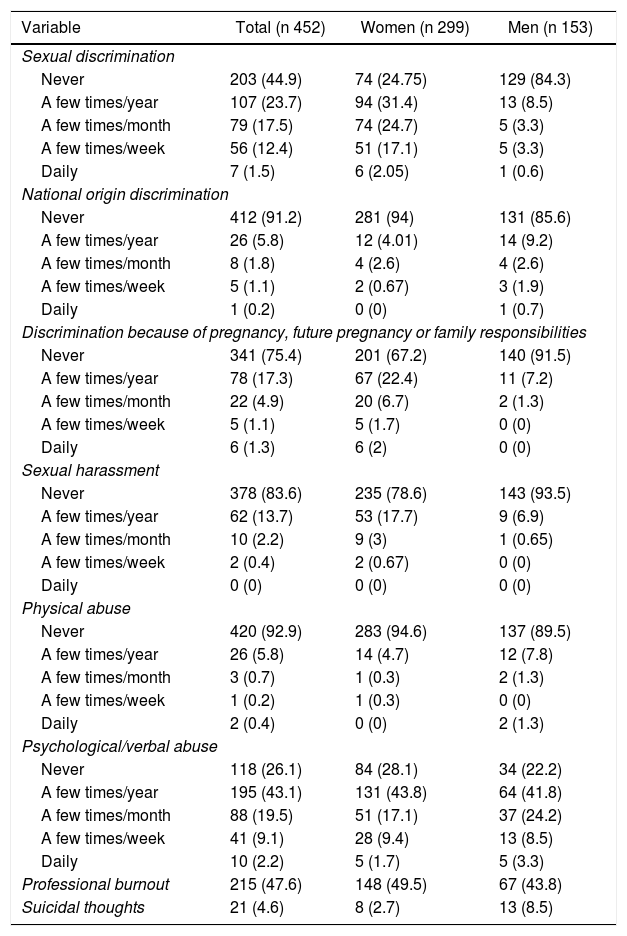
Tables 2 and 3 show the results for discrimination, abuse, and harassment reported by the participating residents. A total of 394 residents (87.2%) reported having experienced an episode of abuse.
Frequency of discrimination, harassment, abuse, professional burnout and suicidal thoughts among Gastrointestinal and General Surgery residents in Spain.
| Variable | Total (n 452) | Women (n 299) | Men (n 153) |
|---|---|---|---|
| Sexual discrimination | |||
| Never | 203 (44.9) | 74 (24.75) | 129 (84.3) |
| A few times/year | 107 (23.7) | 94 (31.4) | 13 (8.5) |
| A few times/month | 79 (17.5) | 74 (24.7) | 5 (3.3) |
| A few times/week | 56 (12.4) | 51 (17.1) | 5 (3.3) |
| Daily | 7 (1.5) | 6 (2.05) | 1 (0.6) |
| National origin discrimination | |||
| Never | 412 (91.2) | 281 (94) | 131 (85.6) |
| A few times/year | 26 (5.8) | 12 (4.01) | 14 (9.2) |
| A few times/month | 8 (1.8) | 4 (2.6) | 4 (2.6) |
| A few times/week | 5 (1.1) | 2 (0.67) | 3 (1.9) |
| Daily | 1 (0.2) | 0 (0) | 1 (0.7) |
| Discrimination because of pregnancy, future pregnancy or family responsibilities | |||
| Never | 341 (75.4) | 201 (67.2) | 140 (91.5) |
| A few times/year | 78 (17.3) | 67 (22.4) | 11 (7.2) |
| A few times/month | 22 (4.9) | 20 (6.7) | 2 (1.3) |
| A few times/week | 5 (1.1) | 5 (1.7) | 0 (0) |
| Daily | 6 (1.3) | 6 (2) | 0 (0) |
| Sexual harassment | |||
| Never | 378 (83.6) | 235 (78.6) | 143 (93.5) |
| A few times/year | 62 (13.7) | 53 (17.7) | 9 (6.9) |
| A few times/month | 10 (2.2) | 9 (3) | 1 (0.65) |
| A few times/week | 2 (0.4) | 2 (0.67) | 0 (0) |
| Daily | 0 (0) | 0 (0) | 0 (0) |
| Physical abuse | |||
| Never | 420 (92.9) | 283 (94.6) | 137 (89.5) |
| A few times/year | 26 (5.8) | 14 (4.7) | 12 (7.8) |
| A few times/month | 3 (0.7) | 1 (0.3) | 2 (1.3) |
| A few times/week | 1 (0.2) | 1 (0.3) | 0 (0) |
| Daily | 2 (0.4) | 0 (0) | 2 (1.3) |
| Psychological/verbal abuse | |||
| Never | 118 (26.1) | 84 (28.1) | 34 (22.2) |
| A few times/year | 195 (43.1) | 131 (43.8) | 64 (41.8) |
| A few times/month | 88 (19.5) | 51 (17.1) | 37 (24.2) |
| A few times/week | 41 (9.1) | 28 (9.4) | 13 (8.5) |
| Daily | 10 (2.2) | 5 (1.7) | 5 (3.3) |
| Professional burnout | 215 (47.6) | 148 (49.5) | 67 (43.8) |
| Suicidal thoughts | 21 (4.6) | 8 (2.7) | 13 (8.5) |
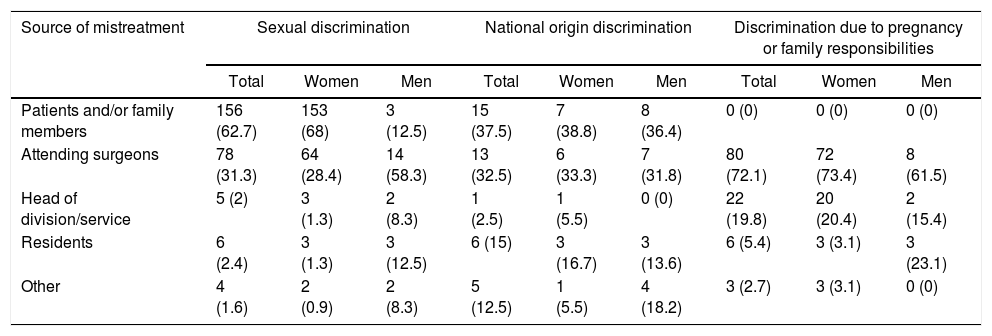
Source of discrimination, harassment and abuse in Gastrointestinal and General Surgery residents in Spain.
| Source of mistreatment | Sexual discrimination | National origin discrimination | Discrimination due to pregnancy or family responsibilities | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Total | Women | Men | Total | Women | Men | Total | Women | Men | |
| Patients and/or family members | 156 (62.7) | 153 (68) | 3 (12.5) | 15 (37.5) | 7 (38.8) | 8 (36.4) | 0 (0) | 0 (0) | 0 (0) |
| Attending surgeons | 78 (31.3) | 64 (28.4) | 14 (58.3) | 13 (32.5) | 6 (33.3) | 7 (31.8) | 80 (72.1) | 72 (73.4) | 8 (61.5) |
| Head of division/service | 5 (2) | 3 (1.3) | 2 (8.3) | 1 (2.5) | 1 (5.5) | 0 (0) | 22 (19.8) | 20 (20.4) | 2 (15.4) |
| Residents | 6 (2.4) | 3 (1.3) | 3 (12.5) | 6 (15) | 3 (16.7) | 3 (13.6) | 6 (5.4) | 3 (3.1) | 3 (23.1) |
| Other | 4 (1.6) | 2 (0.9) | 2 (8.3) | 5 (12.5) | 1 (5.5) | 4 (18.2) | 3 (2.7) | 3 (3.1) | 0 (0) |
| Source of mistreatment | Sexual harassment | Physical abuse | Verbal or psychological abuse | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Total | Women | Men | Total | Women | Men | Total | Women | Men | |
| Patients and/or family members | 15 (20.3) | 13 (20.3) | 2 (20) | 5 (15.6) | 2 (12.5) | 3 (18.8) | 37 (11.1) | 28 (13) | 9 (7.6) |
| Attending surgeons | 46 (62.2) | 43 (67.2) | 3 (30) | 24 (75) | 13 (81.2) | 11 (68.7) | 234 (70.1) | 144 (67) | 90 (75.6) |
| Head of division/service | 1 (1.4) | 1 (1.6) | 0 (0) | 2 (6.3) | 0 (0) | 2 (12.5) | 17 (5.1) | 10 (4.7) | 7 (5.9) |
| Residents | 3 (4.1) | 2 (3.1) | 1 (10) | 1 (3.1) | 1 (6.3) | 0 (0) | 26 (7.8) | 20 (9.3) | 6 (5) |
| Other | 9 (12.2) | 5 (7.8) | 4 (40) | 0 (0) | 0 (0) | 0 (0) | 20 (6) | 13 (6) | 7 (5.9) |
At some point, 249 residents (55.1%) have felt discriminated against because of their gender, 63 (25.3%) of whom have experienced discrimination weekly; most of those affected were women (225 [90.4%]). The most frequent sources of discrimination in women were patients and/or relatives (153; 68%), followed by attending surgeons or the head of the service (67; 29.7%), and other residents (3; 1.3%). In the case of men, on 14 occasions (58.3%) the sources were attending surgeons; in three (12.5%), other residents; and in another three (12.5%), patients and/or relatives.
Forty residents (8.8%), have been discriminated against due to their country of origin, including 18 women (6%) and 22 men (14.4%). Those responsible for discrimination in both sexes have been patients and/or relatives and attending surgeons (15 [37.5%] and 13 [32.5%] cases, respectively).
Some 111 residents (24.6%) have experienced discrimination for being or intending to become pregnant or for family-related responsibilities (98 women [32.8%] and 13 men [8.5%]). Attending surgeons (80; 72.1%) and the head of the department (22; 19.8%) were the most frequent sources of this type of discrimination.
On some occasion, 334 respondents (73.9%) have experienced verbal/psychological abuse. The main offenders were attending surgeons (144 in women [67%] and 90 in men [75.6%]) and patients and/or relatives (28 in women [13%] and 9 in men [7.6%]). Physical abuse occurred in 32 (7.1%) (16 women [5.4%] and 16 men [10.5%]); attending surgeons were most frequently responsible, on 24 occasions, representing 75% of the cases.
The number of residents who have suffered sexual harassment amounts to 74 (16.4%) (64 women [21.4%] and 10 men [6.5%]). The most common source of this abuse was attending surgeons in 46 cases (62.2%), followed by patients and/or relatives in 15 (20.3%), and other professionals in 9 (12.2%).
Burnout was experienced by 215 (47.6%) residents: 148 women (49.5%), and 67 men (43.8%). This was defined as emotional exhaustion by 205 (45.4%) or depersonalization by 48 (10.6%), either daily or weekly. The percentage of women and men who experienced burnout was similar, but depersonalization symptoms were more frequent in males and emotional exhaustion in females (Fig. 1). In the last year, 21 residents (4.6%) reporting having suicidal thoughts.

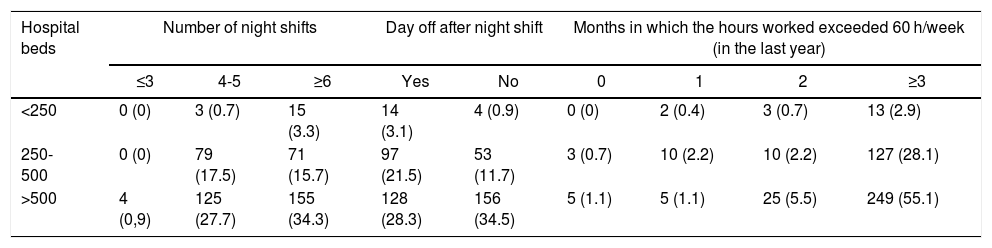
In Fig. 2, we can see the number of months in which the working hour limit (60 hours per week) was violated in the last year among surgical residents, the number of night shifts they performed per month, and whether they were given the following day off.
 among Gastrointestinal and General Surgery residents in Spain.")
Table 4 shows these variables broken down according to hospital size. Breach of work hours was reported by 389 respondents (86.1%) in at least three months; only eight (2%) did not exceed the 60-h limit. Regardless of the size of the hospital, the residents most frequently worked more hours than indicated for three months or more. In hospitals with fewer than 250 beds, there was not a single case in which the work hour limit was not violated. Likewise, 241 residents (53.3%) have had six or more night duties per month, and 207 (45.8%) have had four or five. Practically half of residents (213; 47.1%) did not have a day off after night duty, which is more frequent in large hospitals (> 500 beds). In small and medium-sized hospitals, it is more common to have a day of rest (14 [77.8%] and 97 [64.7%] cases, respectively).
Number of night shifts, days off after night duty, and months with work hour violations among Gastrointestinal and General Surgery residents in Spain, according to hospital size.
| Hospital beds | Number of night shifts | Day off after night shift | Months in which the hours worked exceeded 60 h/week (in the last year) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| ≤3 | 4-5 | ≥6 | Yes | No | 0 | 1 | 2 | ≥3 | |
| <250 | 0 (0) | 3 (0.7) | 15 (3.3) | 14 (3.1) | 4 (0.9) | 0 (0) | 2 (0.4) | 3 (0.7) | 13 (2.9) |
| 250-500 | 0 (0) | 79 (17.5) | 71 (15.7) | 97 (21.5) | 53 (11.7) | 3 (0.7) | 10 (2.2) | 10 (2.2) | 127 (28.1) |
| >500 | 4 (0,9) | 125 (27.7) | 155 (34.3) | 128 (28.3) | 156 (34.5) | 5 (1.1) | 5 (1.1) | 25 (5.5) | 249 (55.1) |
In the logistic regression analysis, the independent predictive factors of professional burnout are: being of Spanish nationality compared to being a foreign national (OR 2.95; 95% CI 1.5-6; P = .03), not having the day off after night duty (OR 2.37; 95% CI 1.6-3.5; P < .001) and exceeding work-hours (OR 1.66; 95% CI 0.9-3; P = .08).
DiscussionUsing a survey sent to all Gastrointestinal and General Surgery residents in Spain, we have tried to determine the prevalence of professional burnout in our country. In our study, 452 residents (61.2%) completed the survey. Although this response percentage is high, the results should be taken with caution since any survey that does not reach 70%-75% of responses may be affected by completion bias.7,8 Being anonymous makes the results more reliable.
After comparing our results with those obtained in the US study,5 there are several aspects to comment. The first is the lower response rate in our country (99.3 vs. 61.2%). This may be justified because the American survey was completed in parallel with the compulsory annual exam, while in our country it was voluntary. Although high, it is surprising that the response rate was not massive. This can be interpreted as a result of disinterest, or perhaps the survey was only completed by residents who had experienced situations compatible with abuse.
Another noteworthy aspect is that all types of abuse were more frequent in Spain than in the US, except discrimination by country of origin. The latter is probably due to the fact that there is a higher percentage of foreign residents in the US. In terms of gender, 55.1% of residents in Spain have felt discriminated against, along with 24.6% due to pregnancy/family responsibilities, versus 31.9% and 7.2% in the US, respectively. In Spain, 73.9% have suffered verbal/psychological abuse, 7.1% physical abuse and 16.4% sexual harassment, versus 30.2%, 2.2% and 10.3%, respectively, in the American survey.
The most frequent causes of discrimination in women were patients and/or relatives (153; 68%). These data reflect that there is a certain discriminatory mindset in our society towards the gender of physicians and specialists. In the US, there is less of this type of discrimination, at 49.2%. The differences observed may be justified by cultural dissimilarities that exist between the two countries. The definition of what is sexual discrimination or verbal/psychological abuse was not clarified.
The persons responsible for mistreatment were similar in both the American and Spanish studies, except when it comes to discrimination due to country of origin and sexual harassment. Racial discrimination in the US is caused more often by patients than by attending physicians. In Spain, both origins are equally frequent. The most frequent perpetrators of sexual harassment in Spain, regardless of gender, were attendings. In the US, there were differences: men reported harassment from the nursing staff and attendings, while women experienced it from patients and attendings.
In Spain, 47.5% of residents have experienced symptoms of burnout at least weekly, compared to 38.5% in the US. In our country, women also experience symptoms of emotional exhaustion more frequently than men. However, in the United States, depersonalization symptoms are equally prevalent in both sexes, while in Spain they predominate in the male gender.
Burnout would be expected in experienced surgeons, in whom their reality does not meet their expectations. In the case of residents, who have just started their professional career, it is a failure that this situation occurs. The significant percentage of its occurrence indicates that the work environment during this training period should be improved.
The percentage of residents who have had suicidal thoughts is very similar in both countries (4.5% in the US and 4.6% in Spain). These figures are lower than those observed in the general community of surgeons in the United States at 6.3%,3 but they are higher than in the general population, at 2%.9
The multivariate analysis has shown that the factors that independently promote professional burnout were Spanish nationality, no day off after a night shift, and exceeding the number of daily work-hours. In the American study,5 the predictive factors found were being first-year residents, experiencing abuse and, likewise, breaching work-hour limits.
In the US, 61% of residents did not exceed their workday hours; 25.2% have exceeded it in one or two months in the last six months; and 13.8% have exceeded it for three months or more. In Spain, only 2% have not exceeded their weekly working hour limit at any time, and 86% have exceeded it at least three months or more. A fundamental aspect to take into account is that the working hour limit in Spain is 60 hours a week, compared to 80 hours in the US. Almost all residents in Spain do at least four night shifts per month, and half of these do six or more. Half of the residents do not have a day off after a night shift, especially in large hospitals.
Exceeding the working hour limit in the US is associated with professional burnout, with an odds ratio (OR) of 1.82 if it is exceeded in one or two months, and with an OR of 2.1 if it is exceeded three months or more. In Spain, this factor has a lesser, although important, effect, with an OR of 1.6. Normalization of working hours implies the collaboration of the hospital administration. This circumstance justifies a widely supported request for medical training to be extended to a residency period of six years.
Kelz R.R. et al. and Ye L. et al.10,11 observed that limiting the working hours of US residents in training, from 100 to 80 hours per week, did not lead to an increase in postoperative complications in patients operated on by these residents. In other words, the excess of hours worked and the lack of rest after a night shift not only do not improve the training of residents, but they also favor their professional burnout. For proper training, the important thing is not the total number of hours worked, but the quality of the training.12
One of the most noteworthy findings of this survey is the high incidence of harassment in our environment, although the number of cases reported to the AEC or CNE is minimal. This may be because harassment situations are rarely reported. In the Freedman-Weiss MR et al.13 article, only 7.6% of residents who experienced sexual harassment reported the incident. The reasons for not reporting it were: considering that the action was not very harmful (62.1%), and believing that it would be a waste of time (47.7%). Other reasons include fear of retaliation and lack of certainty about what behaviors are considered harassment.13 McKinley S.K. et al.14 suggest that surgery department heads should establish institutional policies and create an independent mechanism to report inappropriate behavior. Residents should be educated to report them, with guarantees for confidentiality (both from those who experience them and from witnesses).
Our study has several limitations. As in the US study, harassment, abuse and discrimination were not clearly defined. We also did not evaluate other variables that may be relevant, such as the sexual orientation of residents. The differences in the responses of the residents were not assessed according to their year of residency (R1-5). The percentage of responses to the survey, while significant, was not optimal. Finally, we do not know how many surgical residents have discontinued their residency or changed specialty, or how many complaints there have been as a result of burnout.
ConclusionsIn conducting this study, we have observed that there is professional burnout in Gastrointestinal and General surgery residents in Spanish hospitals. This fact significantly affects residents and their training.
Excessive work hours and the absence of downtime after night shifts are factors that directly influence professional burnout. These are not anecdotal occurrences, as they were reported in 98% and 47% of participants, respectively. An effort must be made not to exceed weekly work hour limitations, and we must try to respect the need for rest after night shifts in order to avoid professional burnout.
The information obtained in this survey will be very useful in the design of the new surgical specialty training program based on objectives, as it should also consider the possible causes of professional burnout in the work environment of residents. The supervising surgeon will be responsible for identifying, monitoring and amending these possible situations, which undoubtedly are an obstacle to adequate training.
FundingThe authors have received no funding for this article.
Conflict of interestsThe authors have no conflicts of interests to declare.
The authors would like to thank all the surgical residents in Spain who completed the survey. Thanks also to the Secretary of the AEC for always being available and for distributing the survey. In addition, thanks go to the supervising surgeons and department heads of Spanish hospitals who encouraged us to conduct this survey.
The following is Supplementary data to this article:
Comisión Nacional de la Especialidad de Cirugía General y del Aparato Digestivo: Antonio José Torres García, David Pacheco Sánchez, José Luis Salvador Sanchís, Eugenio Hernández Antequera, José Luis Lucena de la Poza, José María Jover Navalón, José Luis Gallego, Manuel Bustamante Montalvo.
Please cite this article as: Lucas-Guerrero V, Pascua-Solé M, Ramos Rodríguez JL, Trinidad Borrás A, González de Pedro C, Jover Navalón JM, et al. Desgaste profesional o burnout en los residentes de Cirugía General. Encuesta de la Asociación Española de Cirujanos. Cir Esp. 2020;98:442–449.
Comité Sección de Formación AEC: María Socas Macías, Sergio Moreno, Ignacio Rey Simó, Sandra García Botella, Helena Vallverdú, Inés Rubio, Laura Armananzas, Ivan Arteaga, JM Miguelena, Vicenç Artigas Raventos, Enrique Mercader, Dieter Morales García, Monica Millan, María Dolores Frutos, Gonzalo de Castro, Manuel López Cano, Baltasar Pérez Saborido, Itziar Larrañaga.
