




D2 lymphadenectomy is standard treatment for gastric tumours, but there are still doubts about its extension, specifically the need to perform splenic hilar lymph node dissection with/without associated splenectomy. The use of lymph node mapping with ICG is able to define the D2 territories to be resected as well specific drainage areas for selective expansion. Fluorescence does not indicate the lymph node tumour involvement, but it can help determine the need to extend the dissection, and, in the specific case of the splenic hilum, it provides for its dissection without associated splenectomy.
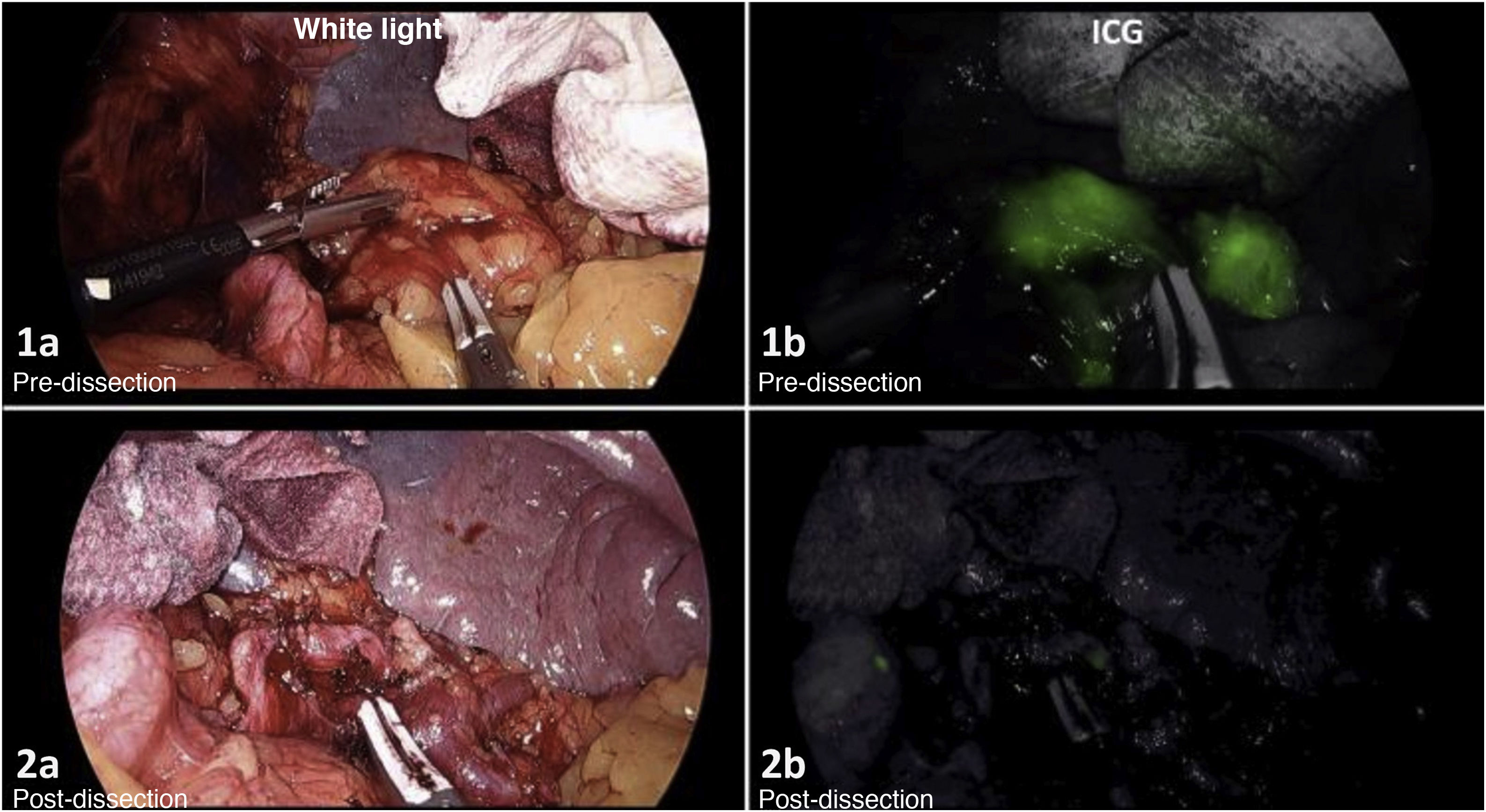
In this image, we can observe the splenic hilum (territory 10), which is not part of a D2 lymph node dissection. The pre-dissection image (Fig. 1a and b) shows the uptake of ICG in the fatty lymphoid tissue of the splenic hilum. After the directed lymphadenectomy, we confirmed adequate lymph node removal (Fig. 2a and b).

Personalized lymph node dissection would optimize the oncological results, minimizing unnecessary surgical procedures as well as the morbidity and mortality associated with gastric cancer surgery.
Please cite this article as: Martínez-Núñez S, Alarcón del Agua I, Senent Boza A, Morales-Conde S. Individualización de la linfadenectomía del hilio esplénico en el cáncer gástrico: valor del mapeo por ICG. Cir Esp. 2022;100:173.
